










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.2 Bogotá abr./jun. 2011
Comparison of the performance of plastic stents in palliation of proximal and distal malignant biliary obstructions
Rodrigo Castaño, MD (1), Andrés Ricardo, MD (2), Lina Velásquez MD (2), Mario H. Ruiz MD (1), Luis M. Ruiz (3)
(1) Cirugía Gastrointestinal y Endoscopia, HPTU-Gastrohepatología U de A, Medellín, Colombia.
(2) Residente de Cirugía General, Universidad Pontificia Bolivariana, Medellín, Colombia.
(3) Estudiante Medicina, Universidad Pontificia Bolivariana, Medellín, Colombia.
Correspondencia: Dr. Rodrigo Castaño Llano rcastanoll@une.net.co
Received: 16-11-10 Accepted: 06-04-11
Abstract
Aim: To compare the efficacy of plastic stents in the treatment of distal and proximal stricture of biliary tract neoplasms.
Methods: From January 2002 to February 2009, 70 patients (37 males, 33 females) with non surgically resectable malignant biliary obstruction who received plastic stent implantation were reviewed retrospectively. The stents were inserted by endoscopy. The endoscopist implants one or more stents if he considers this necessary. The end points of the study were stent occlusion and patient death.
Results: The mean time of stent patency was 81 ± 75 days in the group of proximal stricture (group 1) and 130 ± 68 days in the group of distal stricture (group 2), (p 0.40, with CI 95% 0.47-1.37). The mean survival time was 126 days in group 1 and 159 days in group 2. There was not a significant difference between the two groups.
Conclusion: Plastic stent implantation is a feasible, palliative method for unresectable malignant biliary obstruction. The overall survival and obstruction with the use of plastic stent in patients with distal stenoses compared with proximal obstruction was not significantly different in our study.
Key words
Stents, Biliary Tract Neoplasm, ERCP.
INTRODUCTION
Biliary stenting is currently the treatment of choice for proximal or distal malignant biliary obstructions caused by inoperable primary or metastatic biliary tumors (1-3).
There are two types of stents used for treating malignant biliary stenosis: plastic prosthetics (PP) and self expanding metallic stents. PPs were originally developed as simple polyethylene tubes which were placed in the biliary duct to allow drainage of bile. These devices have undergone certain modifications such as the addition of lateral orifices to optimize drainage and flaps to avoid migration. Nevertheless, PPs have presented long term permeability problems due to the formation of bacterial biofilm on them. This leads to occlusion within approximately 3 months for 10 11.5 French stents (4). Consequently, unplanned stent replacements are needed for approximately 50% of the patients (4, 5).
Self expanding metallic stents (SEMS), which are made from either titanium alloy (45%) or nickel (55%), have had better performance in relation to long term permeability, ease of implantation in bile ducts with stenosis and in relation to cost efficiency in patients whose estimated survival time is greater than 6 months (6-11)
Despite this, the use of plastic prosthetics continues to be the rule since there are great limitations of administrative capacity. Moreover, experience in safely implanting metallic prosthetics is also limited at some medical centers.
In a prospective series of 61 patients who had had SEMS implanted to treat malignant biliary obstructions, Chen et al. (3), found that these stents retained their permeability longer in cases proximal tumors (421 days) than in cases of distal tumors (168 days). Also, the survival time was significantly greater in the group with proximal obstructions (574 days vs. 182 days) which is probably associated with the type of tumor.
This study aims to evaluate the permeability of stents, and the life expectancy of patients who had inoperable both proximal or distal biliary stenoses and who had been treated with endoscopically placed plastic stents at a level four center locally known treating hepatobiliary pathologies.
MATERIALS AND METHODS
From January 2002 to February, 2009, the cases of seventy patients (37 men and 33 women) who had had plastic biliary stents implanted at the Pablo Tobon Uribe Hospital in Medellin, Colombia, and who were over the age of 18 years, were retrospectively reviewed. All of these patients had been treated for inoperable malignant obstructions (primary or metastatic) which had been diagnosed by MRIs, endoscopically and/or pathologically.
Endoscopic retrograde cholangiopancreatography (ERCP) was performed on all patients with their informed consent. One or several stents were placed according to the amount required to palliate the obstruction. Two different types of 8.5 or 10 French polyethylene stents (Figure 1) were used depending on availability at the moment procedures were performed.

Figure 1. Plastic stents placed in patients in this study. A. Biliary Stent variety Cotton-Leung 10 FR. Cook Medical Inc., Winston-Salem, NC. B. Plastic biliary stent in situ for palliation of malignant biliary obstruction. C. 10 FR Biliary stent. RX Biliary System. Boston Scientific Corporation, Natick, Mass.
Lesions were defined as distal stenoses if the tumor was located under in the area from union of the cystic duct to the bile duct. They were defined as proximal stenoses if the tumor was located above that same anatomical region.
Occlusion of the stent was defined as the recurrence of jaundice or, the presence of cholangitis with evidence of the stents occlusion requiring biliary intervention after the successful placement of one or several PPs.
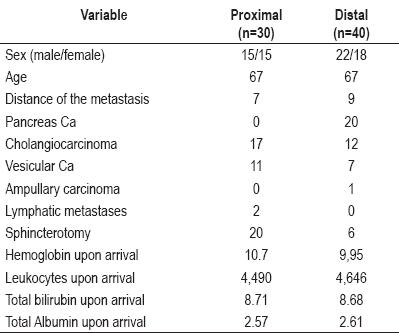
The duration of a stents permeability was calculated as the time elapsed from the placement of the stent until its occlusion or the patients death. The stents cumulative permeability and the patients life expectancy were evaluated using the Kaplan-Meier technique. The studys main objectives were to evaluate the permeability of biliary stents in the palliation of malignant biliary obstructions and to compare the life expectancies of patients with proximal obstructions with those of patients with distal obstructions. Table 1 shows patients demographic information together with types of tumors and each groups paraclinical data.
Table 1. Basal characteristics of patients according to type of porcedure
Patients were chosen from the data base of procedures performed by the Endoscopy Unit at the Pablo Tobon Uribe Hospital. The data was directly extracted by the investigators from the informative clinical files at the Pablo Tobon Uribe Hospital. Calls were made to patients or their relatives in order to complete the monitoring and to determine life expectancy.
RESULTS
Patient selection and characteristics
Seventy patients were selected for this study. They were divided into two groups according to level of bile duct obstruction. The 30 patients in Group 1 had obstructions above the cystic duct ostium. The patients in the group collectively had 17 cholangiocarcinomas, and 11 gallbladder carcinomas. Two patients had hilar lymph node metastases from other tumors (colon carcinoma). The 40 patients in Group 2 had stenoses below the junction of the choledochous and cystic ducts. It included 12 patients with distal cholangiocarcinoma, 20 patients with pancreatic cancers, 1 patient with a ampullary carcinoma and 7 patients with gallbladder cancer. If at any moment during the monitoring there was any suspicion of a stent occlusion, another ERCP was performed and the stent was replaced or an additional stent was inserted. No stent replacements were programmed in advance. Table 2 shows variables in relation to tumor locations.
Table 2. Estimated risk according to type of procedure (proximal or distal) and related variables.

STENT PERMEABILITY AND LIFE EXPECTANCY
The median time stent permeability was maintained was 81 ± 75 days in the proximal stenosis group (Group 1) and 130 ± 69 days in the distal stenosis group (Group 2). The difference was not significant with P = 0.40, and a 95% CI of 0.47 to 1.37. Average life expectancy was 126 ± 83 days in Group 1 and 159 ± 60 days in Group 2.
Although there was no significant difference in life expectancy at the end of the monitoring period, the life expectancy graphs show some differences up until day 110 in Figure 2 and until the 150th day in Figure 3.
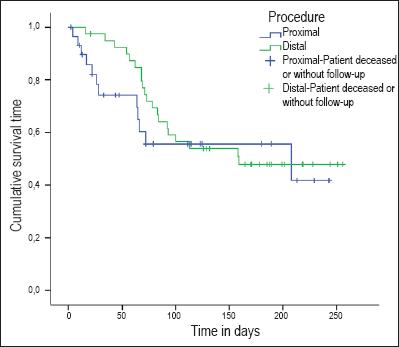
Figure 2. Cumulative patient survival time prior to stent obstruction according to tumor location.
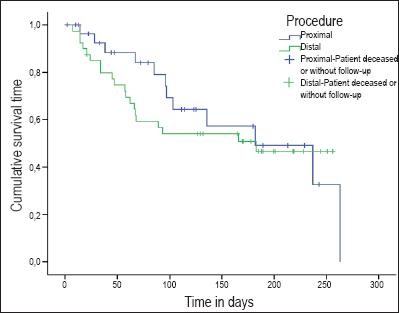
Figure 3. Cumulative patient survival time after stent obstruction according to type of procedure.
The patients cumulative permeability time and life expectancies according to the Kaplan-Meier life chart are shown in Figures 2 and 3.
EARLY COMPLICATIONS
Early complications were defined as complications which occurred within 30 days of stent placement. 18 patients developed early complications. Six of them belonged to the distal stenosis group and twelve belonged to the proximal stenosis group.
LATE COMPLICATIONS
Late complications were defined as complications which occurred more than 30 days after placement of the stent. There were two categories of late complications. The most important consists of stent obstructions which occurred in 23 patients (32.9%), 11 in Group 1 and 12 in Group 2. The second category of late complications was gastric obstruction. This occurred in 5 cases, all in the distal obstruction group.
DISCUSSION
The clinical behavior and the natural history of intrahepatic and extrahepatic bile duct neoplasias have different determinants. These include the type of tumor, its clinical status, and the absence or presence of metastases. One factor that must be considered for management of these neoplasias is location within the bile duct. Those found from the secondary hepatic ducts to the confluence of the common hepatic duct with the cystic duct are considered proximal, while those located from the cystic duct to the juncture of the common bile duct in the duodenum are considered distal (1, 3, 12, 13).
Criteria for inoperability in cases of cholangiocarcinomas include bilateral compromise of the secondary hepatic bile ducts, atrophy of a hepatic lobule combined with compromise of the contralateral portal vein, and an atrophy of a lobule combined with compromise of a contralateral secondary bile duct. Bilateral portal compromise, or compromise of the portal vein, is also a classic counter indication for surgical resection, as is bilateral compromise of the hepatic artery.
Whether or not involvement of the local lymph node is a counter indication is more controversial. The results obtained in other studies do not counter indicate surgery in these cases, although distant lymph node metastases do.
On the other hand behavior, type of patient, and comorbidities including cirrhosis and systemic cardiovascular diseases, must be taken into account when a patient is referred for surgery due to the high morbidity and mortality rates in high risk patients during curative procedures.
Historically, palliative treatment using biliary prostheses for of unresectable distal tumors has had more favorable characteristics than has their use in cases of inoperable proximal tumors (3, 9). Nevertheless, recent studies have demonstrated favorable results in proximal tumor palliation through biliary prosthesis, especially in terms of stent permeability time and the patient life expectancy (3). To date, these reports have relied solely on data related to SEMS which are rare resource in our working environment. Moreover, there are no known studies of comparing the performance of the more common plastic stents for palliation of malignant stenoses in different locations.
This study attempts to compare the performance of PPs in the treatment of proximal malignant biliary with their performance in the treatment of distal obstructions in terms of life expectancy, value for relief of bile obstructions and duration of permeability. Two homogeneous groups of patients with malignant bile obstructions were compared. The classification criteria used to assign patients to groups were tumor location: proximal or distal to the cystic duct implantation.
In the proximal obstruction group, cholangiocarcinomas were the most frequent type of tumor with 17 cases. This was followed by 11 cases of gallbladder carcinomas and two cases of patients with hilar lymph node metastases from other tumors. In the distal obstruction group, pancreatic carcinomas were the most frequent tumor with 20 cases, followed by cholangiocarcinoma with 12 cases.
These differences in the etiologies of the obstructions are considered to be initial determinants of life expectancy because the variability of the prognoses depends on the types of tumors. Nevertheless, we included these factors in the analysis because the total life expectancy was considered as a variable in other studies. This resulted in finding statistically significant differences in favor of palliation of proximal tumors (3), although the analysis in our study did not find statistically significant differences in total life expectancies. This leads us to think that the histological origin of the tumors that cause this type of biliary obstruction does not determine life expectancy. This finding may also be explained by the advanced state of the disease in the study patients. The patients in both groups had notably short life expectancies which were probably related more closely to the stages of the diseases than to the type of tumors.
The objectives related to stent permeability show that a median of 81 ± 75 days in the group with proximal stenosis compared to 130 ± 69 days in the group with distal stenosis. Although suggests more favorable behavior of plastic stents in patients with distal stenosis than in other patients, the difference was not statistically significant implying that no matter whether tumors are distal or proximal, patients with inoperable malignant biliary obstructions benefit from palliative treatment with these prostheses. The tumors location should not affect a decision to place a stent.
Twelve patients from the proximal obstruction group presented early complications which was a significant difference from the early complication rate in the distal obstruction group (P= 0.027, 95% CI from 1.07 to 7.26). Nevertheless, this difference disappeared when late complications occurring 30 days after placement of stents were considered. The most important late complication was stent obstruction which occurred in 11 patients in the proximal obstruction group and in 12 in the distal obstruction group. This suggests that the long term security of the stent is similar for both tumor locations without any increase in the risk of complication in either group.
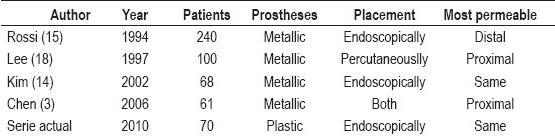
Many factors, including the affects of proximal and distal tumor locations, have been studied in the attempt to predict whether or not early stent obstruction will occur. Kim (14) found no differences between proximal and distal obstructions. Rossi (15) found higher rates of permeability in the prostheses used for distal stenosis than in those used to treat proximal stenosis, while Chen (3) found longer lasting permeability in stents placed for malignant proximal obstructions. Kim (14) detected that appropriate stent expansion 24 hours after the insertion and the passing of a large diameter device through the stenosis before the placement of the stent were parameters which were significantly related to stent permeability.
Whether or not it is best to place a stent near or through the sphincter of Oddi is a matter of debate, as are the relation to proximal and distal locations of the lesion and the frequency of complications. Tarnasky (16) found that the rate of occurrence of pancreatitis increased in patients with proximal biliary stenosis without prior sphincterotomies after the placement of a transpapillary stent. This was probably due to lesions acting as supports which caused stents to deflect into the distal extreme thus compromising the pancreatic orifice. Patients with proximal biliary stenosis who had not had sphincterotomies had significantly higher risks of post ERCP pancreatitis than did patients with distal stenosis who had not had sphincterotomies.
Malignant obstruction of the bile duct is a late complication of different types of neoplasias that occurs in the topography of the biliopancreatic crossing. Its prognosis depends upon multiple factors. In cases where there is no cure, palliation with endoscopic biliar prostheses has proven to be safe. It is currently considered to be the standard palliative treatment, although analysis of how proximity of the biliary obstruction to the porta hepatis has not been fully developed. There are few studies that compare the behavior of prostheses in proximal and distal malignant biliary stenoses. Those which do have normally studied metallic prostheses (3, 14, 18), have evaluated both malignant and benign stenoses (16), and have studied stents which were placed both endoscopically and percutaneously (18).
In this study, there were no significant differences in the permeability of prostheses which were related to the locations of the obstruction. However, as shown in Table 3, findings in earlier studies vary.
Table 3. Studies of positions of prostheses and duration of permeability
Clear conclusions that are applicable to all cases are not yet available. Additional studies are still needed to allow us to draw certain conclusions regarding the development of plastic and metallic stents for palliation of different types of malignant biliary obstructions and thus to modify the indications for treatment.
REFERENCES
1. Blechacz BR, Gores GJ. Cholangiocarcinoma. Clin Liver Dis 2008; 12(1): 131-50.
2. Larghi A, Tringali A, Lecca PG, Giordano M, Costamagna G. Management of hilar biliary strictures. Am J Gastroenterol 2008; 103(2): 458-73.
3. Chen JH, Sun CK, Liao CS, Chua CS. Self-expandable metallic stents for malignant biliary obstruction: efficacy on proximal and distal tumors. World J Gastroenterol 2006; 12(1): 119-22.
4. Stern N, Sturgess R. Endoscopic therapy in the management of malignant biliary obstruction. Eur J Surg Oncol 2008; 34(3): 313-7.
5. Prat F, Chapat O, Ducot B, Ponchon T, Pelletier G, Fritsch J, et al. A randomized trial of endoscopic drainage methods for inoperable malignant strictures of the common bile duct. Gastrointest Endosc 1998; 47(1): 1-7.
6. Rieber A, Brambs HJ. Metallic stents in malignant biliary obstruction. Cardiovasc Intervent Radiol 1997; 20(1): 43-9.
7. Davids PH, Groen AK, Rauws EA, Tytgat GN, Huibregtse K. Randomized trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet 1992; 340(8834-8835): 1488-92.
8. Castaño R, Lopes TL, Alvarez O, Calvo V, Luz LP, Artifon EL. Nitinol biliary stent versus surgery for palliation of distal malignant biliary obstruction. Surg Endosc 2010; 24(9): 2092-8.
9. Castaño R, Nuñez E, Ruiz MH, Juliao F, Sanin E, Erebrie F. A New Nitinol Stent Produced Locally Versus Surgery in Palliation of Distal Malignant Biliary Obstruction. Gastrointestinal Endoscopy 2007; 65(5): AB220.
10. Artifon EL, Castaño R, Álvarez O, Aparicio DP, Sakai C, Paione JB. Fully covered self-expandable Metal Stent versus plastic stent in the treatment of biliary leaks after cholecystectomy: a multicenter study. Gastroint Endosc 2010; 71(5): AB310.
11. Castaño R, Álvarez O, García A, Quintero V, Sanín E, Erebrie F, Nuñez E, Calvo V, García LH. Stent metálico versus plástico en la obstrucción biliar maligna distal. Rev Col Gastroenterol 2009; 24(3): 248-255.
12. Polydorou AA, Cairns SR, Dowsett JF, Hatfield AR, Salmon PR, Cotton PB, et al. Palliation of proximal malignant biliary obstruction by endoscopic endoprosthesis insertion. Gut 1991; 32(6): 685-9.
13. Dowsett JF, Polydorou AA, Vaira D. Endoscopic Stenting for malignant biliary obstruction: how good really? A review of 641 consecutive patients. Gut 1988; 29: 1458.
14. Kim HS, Lee DK, Kim HG, Park JJ, Park SH, et al. Features of malignant biliary obstruction affecting the patency of metallic stents: a multicenter study. Gastrointestinal Endoscopy 2002; 55(3): 359-365.
15. Rossi P, Bezzi M, Rossi M, Adam A, Chetty N, Rodie ME, et al. Metallic stents in malignant biliary obstruction: results of a multicenter European study of 240 patients. J Vas Interv Radiol 1994; 5: 279-285.
16. Tarnasky PR, Cunningham JT, Hawes RH, Hoffman BJ, Uflacker R, et al. Transpapillary stenting of proximal biliary strictures: does biliary sphincterotomy reduce the risk of postprocedure pancreatitis? Gastrointestinal Endoscopy 1997; 45(1): 46-51.
17. Giogio PD, Luca LD. Comparison of treatment outcomes between biliary plastic stent placements with and without endoscopic sphincterotomy for inoperable malignant common bile duct obstruction. World J Gastroenterol 2004; 10(8): 1212-1214.
18. Lee B, Choe D, Lee J, Kim K, Chin S. Metallic stents in malignant biliary obstruction: Prospective long-term clinical results. AJR 1997; 168: 741-745.
1. Blechacz BR, Gores GJ. Cholangiocarcinoma. Clin Liver Dis 2008; 12(1): 131-50. [ Links ]
2. Larghi A, Tringali A, Lecca PG, Giordano M, Costamagna G. Management of hilar biliary strictures. Am J Gastroenterol 2008; 103(2): 458-73. [ Links ]
3. Chen JH, Sun CK, Liao CS, Chua CS. Self-expandable metallic stents for malignant biliary obstruction: efficacy on proximal and distal tumors. World J Gastroenterol 2006; 12(1): 119-22. [ Links ]
4. Stern N, Sturgess R. Endoscopic therapy in the management of malignant biliary obstruction. Eur J Surg Oncol 2008; 34(3): 313-7. [ Links ]
5. Prat F, Chapat O, Ducot B, Ponchon T, Pelletier G, Fritsch J, et al. A randomized trial of endoscopic drainage methods for inoperable malignant strictures of the common bile duct. Gastrointest Endosc 1998; 47(1): 1-7. [ Links ]
6. Rieber A, Brambs HJ. Metallic stents in malignant biliary obstruction. Cardiovasc Intervent Radiol 1997; 20(1): 43-9. [ Links ]
7. Davids PH, Groen AK, Rauws EA, Tytgat GN, Huibregtse K. Randomized trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet 1992; 340(8834-8835): 1488-92. [ Links ]
8. Castaño R, Lopes TL, Alvarez O, Calvo V, Luz LP, Artifon EL. Nitinol biliary stent versus surgery for palliation of distal malignant biliary obstruction. Surg Endosc 2010; 24(9): 2092-8. [ Links ]
9. Castaño R, Nuñez E, Ruiz MH, Juliao F, Sanin E, Erebrie F. A New Nitinol Stent Produced Locally Versus Surgery in Palliation of Distal Malignant Biliary Obstruction. Gastrointestinal Endoscopy 2007; 65(5): AB220. [ Links ]
10. Artifon EL, Castaño R, Álvarez O, Aparicio DP, Sakai C, Paione JB. Fully covered self-expandable Metal Stent versus plastic stent in the treatment of biliary leaks after cholecystectomy: a multicenter study. Gastroint Endosc 2010; 71(5): AB310. [ Links ]
11. Castaño R, Álvarez O, García A, Quintero V, Sanín E, Erebrie F, Nuñez E, Calvo V, García LH. Stent metálico versus plástico en la obstrucción biliar maligna distal. Rev Col Gastroenterol 2009; 24(3): 248-255. [ Links ]
12. Polydorou AA, Cairns SR, Dowsett JF, Hatfield AR, Salmon PR, Cotton PB,et al. Palliation of proximal malignant biliary obstruction by endoscopic endoprosthesis insertion. Gut 1991; 32(6): 685-9. [ Links ]
13. Dowsett JF, Polydorou AA, Vaira D. Endoscopic Stenting for malignant biliary obstruction: how good really? A review of 641 consecutive patients. Gut 1988; 29: 1458. [ Links ]
14. Kim HS, Lee DK, Kim HG, Park JJ, Park SH, et al. Features of malignant biliary obstruction affecting the patency of metallic stents: a multicenter study. Gastrointestinal Endoscopy 2002; 55(3): 359-365. [ Links ]
15. Rossi P, Bezzi M, Rossi M, Adam A, Chetty N, Rodie ME, et al. Metallic stents in malignant biliary obstruction: results of a multicenter European study of 240 patients. J Vas Interv Radiol 1994; 5: 279-285. [ Links ]
16. Tarnasky PR, Cunningham JT, Hawes RH, Hoffman BJ, Uflacker R, et al. Transpapillary stenting of proximal biliary strictures: does biliary sphincterotomy reduce the risk of postprocedure pancreatitis? Gastrointestinal Endoscopy 1997; 45(1): 46-51. [ Links ]
17. Giogio PD, Luca LD. Comparison of treatment outcomes between biliary plastic stent placements with and without endoscopic sphincterotomy for inoperable malignant common bile duct obstruction. World J Gastroenterol 2004; 10(8): 1212-1214. [ Links ]
18. Lee B, Choe D, Lee J, Kim K, Chin S. Metallic stents in malignant biliary obstruction: Prospective long-term clinical results. AJR 1997; 168: 741-745. [ Links ]

