










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.2 Bogotá Apr./June 2011
Large balloon papillary dilation (LBPD) for choledocholithiasis
Rómulo Vargas Rubio MD (1), Gerardo Guzmán, MD (2)
(1) Gastroenterologist. Hospital Universitario de San Ignacio. Clínica de Marly. Bogotá, Colombia.
(2) Internist Training resident in Gastroenterology. Pontificia Universidad Javeriana. Hospital Universitario de San Ignacio. Bogotá, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 01-06-11 Accepted: 15-06-11
Abstract
Background. Difficult bile duct stones of over 15 mm diameter cause choledocholithiasis in significant numbers of patients. This condition requires the use of techniques such as mechanical lithotripsy (ML) which are more complex than sphincterotomy and which also require more time to accomplish. This increases the potential for complications.
Objective. To describe our experience with attempted papillary dilations with large balloons to treat difficult bile duct stones.
Design. Observational study. Descriptive research. Case series.
Results. Endoscopic retrograde cholangiopancreatography (ERCP) and LBPD procedures were attempted in 20 patients aged 43 to 91. Of these patients 11 were men, and 14 were women. ERCPs and ESTs had previously been performed on 14 of these patients (70%), while this was the first time for the other 6 patients (30%). Indications for performing LBPDs were bile duct stones ≥ 15 mm in 11 patients (55%), disproportion between common the bile duct and the papillary orifice in 12 patients (60%), and both conditions in 3 patients (15%). The total success rate for resolution of choledocholithiasis was 95%. Removal of bile duct stones in a single session was accomplished in 17 patients (85%) while two additional sessions each were required to remove the stones in two patients (10%). It was not possible to completely remove one patients stones (5%) endoscopically. Only 7 patients (35%) required lithotripsy. The total complication rate was estimated at approximately 10%. One patient (5%) presented a small amount of bleeding after the sphincterotomy, but no intervention was required. Another patient (5%) presented a mild post-ERCP pancreatitis which evolved satisfactorily.
Conclusions. This is the first case series report of the use of LBPD to treat difficult bile duct stones as a new alternative for resolving choledocholithiasis. It obtained a 95% success rate. Thanks to this technique, we avoided treatment with mechanical lithotripsy in 65% of these cases and also obtained an acceptable rate of complications. The clinical findings reported in this study correlate well other case series reports and clinical trials published in the literature. Although this is a preliminary study, these results suggest that the LBPD is a safe and effective technique for treating difficult bile duct stones.
Key words
Choledocholithiasis, difficult bile duct stones, ERCP, LBPD.
INTRODUCTION
Choledocholithiasis is a common condition which occurs in up to 10% of the worlds population (1, 2). This condition develops in 10% to 20% of the patients who present cholelithiasis. The literature suggests that from 3% to 10% of the patients who undergo cholecystectomies have stones in the common bile duct (1, 2).
Most bile duct stones are treated via endoscopic sphincterotomies (ESTs), followed by stone removal using a balloon catheter or a dormia basket (3). Nevertheless, patients with large and difficult stones (≥ 15 mm diameter), or stones whose sizes exceed the diameter of the ampullary orifices, generally require additional intervention with methods such as mechanical lithotripsy (ML) (9). Consequently, techniques other than EST and ML have been developed to treat difficult bile duct stones.
Endoscopic papillary large balloon dilation (EPLBD) after a sphincterotomy has recently been shown to be effective and relatively safe for removal of large stones. Most patients have not needed additional procedures such as MLs (11).
The aim of this study was to describe our experience using ELBPD for patients who had stones which were impossible to remove via EST or conventional techniques such as balloon catheter or the dormia basket, or even after the use of difficult techniques such as ML.
PATIENTS AND METHODS
Patients
Our study brings together valuable data from a series of patients who received care at Hospital de San Ignacio and at the Clinica de Marly in Bogota between 2007 and 2011. All the patients underwent ERCPs. Twenty of these patients, all over the age of 18, decided to undergo dilation with large balloons following sphincterotomies (repeat or de novo) to remove difficult bile duct stones. Stone removal in these patients was not possible via balloon catheter or dormia basket, although appropriate sphincterotomies were accomplished. Technical difficulty in removing stones was defined as the presence of giant stones in the choledochus (over 15 mm) and/or disproportion between the size of the stone and the papillary orifice or the distal choledochus. All patients had indications for ERCPs due to alterations in hepatic function tests and biliary route abnormalities seen in images. Previous ERCPs had failed to resolve the choledocholithiases of some patients. Coagulation tests were performed on all patients prior to the procedure.
All patients knew the possible risks and benefits of participating in this study and had signed informed consent forms prior to the procedure.
Procedure
All ERCP procedures were performed by Rómulo Vargas MD, a specialist in endoscopy, using a therapeutic duodenoscope (Olympus V-Scope TJF-160VF). All ERCP procedures were monitored during sedation. Selective cannulation of the biliary route was performed on all patients using a pre-curved guided Autotome Rx Cannulating Sphincterotome (Ultratome XL, Boston Scientific). After obtaining images from cholangiography, limited sphincterotomies were performed on patients who had had no previous ERCPs. The security folds were used as points of reference. Electrocauterization was used to make the endoscopic cut.
Afterwards, a CRE™ controlled radial expansion balloon dilator (Boston Scientific) was used to insert the balloon into a ten to twenty mm diameter in the biliary duct. Two thirds of a balloon was introduced into the distal choledochus while one third was allowed to remain outside in the papillary orifice. The balloon was gradually inflated to 10 mm. Maximum expansion of the balloon was determined by the size of the stone, diameter of the choledochus and the diameter of the papillary orifice. The inflated balloon was held in position for 30 seconds and then deflated. After papillary expansion with the balloon, we removed stones using 8.5 to 15 mm balloon catheters and/or a dormia basket. In cases in which removal with these devices was not possible we performed mechanical lithotripsy using the Litocrush BML-201Q (Olympus).
Results
ERCPs with large balloon (large ≥ 10 mm balloon) papillary dilatation were conducted on a total of 20 patients including 11 men (55%) and 9 women (45%) whose ages ranged between 43 and 91 years (average age 74.5 years). Sixteen patients (80%) had had previous cholecystectomies, fourteen patients (70%) had had previous ERCPs which failed to remove all stones. Stent had been placed in 11 out of these patients (79%) as a transitory biliary route detours. Mechanical lithotripsies (ML) had been attempted on three patients (21%) without solving their choledocholithiases. Clinical characteristics of the patients upon whom LBPDs were performed are summarized in Table 1.
Table 1. Patients’ clinical characteristics.
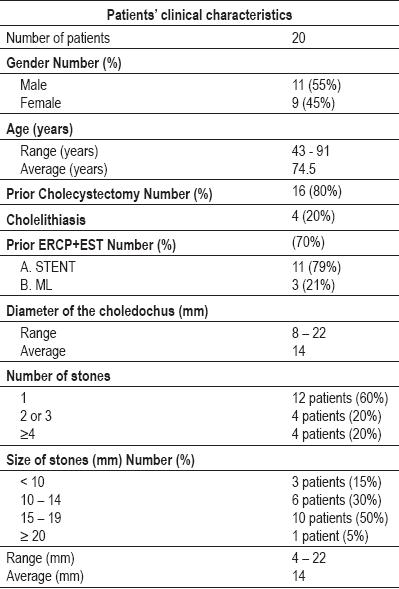
The average diameter of the choledochus ducts studied was 14mm, while the range was from 8 mm to 22 mm. Single stones were found in the choledochus ducts of twelve patients (60%), two or three bile duct stones in the ducts of four patients (20%), and four or more stones were found in the ducts of four patients. Ten patients (50%) presented stones of between 15mm and 19 mm, six patients (30%) had stones of between 10 mm and 14 mm, and three patients had stones of approximately 10 mm. One patient had stones larger than 20 mm. The average size of patients bile duct stones was 14 mm.
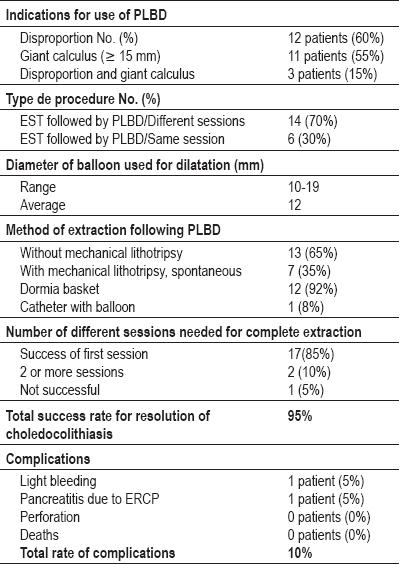
The main indications for performing LBPDs were the presence of stones ≥ 15mm, found in 11 out of the 20 patients (55%), and disproportion between stone size and the papillary orifice, found in 12 patients (60%). Three patients (15%) presented both indications.
Fourteen patients (70%) had ESTs related to earlier ERCPs. For these patients LBPDs were performed in a separate session. ESTs followed by LBPDs were performed in a single session on 6 patients (30%). The average balloon diameter used for papillary expansion was 12 mm, and the range was from 10 mm to 19 mm. MLs to remove stones were not performed on 13 patients (65%) after LBPDs. In 12 out of theses 13 patients (92%), we used the dormia basket-assisted method, while we used the catheter balloon-assisted method for 1 patient (8%). A total of 7 patients (35%) needed MLs to solve choledocholithiases. Spontaneous passage of bile duct stones did not occur in any of the patients studied after the LBPDs were performed.
The choledocholithiasis resolution rate was 95% Seventeen patients (85%) required only a single session to solve the condition, while two patients (10%) needed two or more sessions to completely remove the stones, and it was not possible to attempt endoscopic removal of the stones in the choledochus in the case of one patient (5%).
Complications occurred in two patients (10%). One patient (5%) presented melena after the procedure. Another endoscopy, conducted to check the cause of the melena, found bleeding originating from the EST. However, the bleeding stopped without the necessity of further intervention. Another patient showed post-ERCP pancreatitis with amylase levels elevated four times during the first 24 hours. The patient improved with medical treatment. The results of LBPDs are summarized in Table 2.
Table 2. Results from papillary large balloon dilation (PLBD).
DISCUSSION
Endoscopic treatment is the first-line method for managing bile duct stones (10). Endoscopic sphincterotomies (EST), the most commonly used technique (6), can remove 90% of bile duct stones when a balloon catheter or a dormia basket is used afterwards (10).
Despite the effectiveness of ESTs for removal of bile duct stones, they cannot be performed in the presence of certain kinds of stones. Key factors which complicate removal include stones > 15 mm, barrel shaped stones, and narrowness in the distal choledochus duct (13). In these cases additional procedures, such as mechanical lithotripsy, are required to completely remove the bile duct stones (13). Normally most large-sized and difficult stones can be removed using mechanical lithotripsy. However, this is a long and complex procedure which may require several sessions for complete removal. In recent years a sphincterotomy combined with large balloon papillary dilatation has emerged as a different alternative for treatment of difficult bile duct stones.
Endoscopic large balloon papillary dilatation is different from ordinary endoscopic papillary balloon dilation (EBD) which is performed alone with a smaller balloon and without a sphincterotomy. EBD is performed to expand the ampullary orifice with a balloon that measures less than 10 mm diameter, and as just mentioned, without conducting an endoscopic sphincterotomy (3). This procedure has the advantage of preserving the functioning of the Sphincter of Oddi, and some authors consider this method important, especially for young patients (4). Many clinical studies in Japan have concluded that EBDs are a safe and effective method for removal of difficult stones without serious complications or mortality. Despite the popularity of this procedure in Japan, the safety of this method has been criticized in the West because other studies have shown that it is associated with high incidences of pancreatitis. Furthermore, in cases of large stones EBD is limited, and endoscopic sphincterotomies combined with MLs are required (3, 11, 12).
LBPDs are useful primarily for removal of large stones located in the choledochus duct whose extraction would otherwise only be possible using mechanical lithotripsy. Ten to twenty mm diameter balloons are used to expand the distal choledochus duct and the papilla (3,11).
The aim of the LBPD is to avoid or to reduce the use of mechanical lithotripsy and to diminish the total number of sessions needed to completely remove stones.
Several reports which include technical descriptions of LBPDs are available in the literature. Once a balloon is inflated, the biliary duct will acquire a uniform cylindrical structure from the middle of the choledochus duct to the papillary orifice. In practice, with the aid of endoscopic and fluoroscopic vision, half of the balloon is positioned in the ampullary orifice. The disappearance of the "waist" of the balloon as air pressure increases must be detected after the injection of contrast media (3, 11). Once the waist disappears, the balloon must remain inflated for 60 seconds.
This technique was first reported by Ersoz et al. in Turkey in 2003. Their retrospective study of the use of LBPDs in 58 patients had an 89% success rate in patients with narrowed distal choledochus ducts, and a 95% success rate in patients who had difficult large stones which could not be extracted using conventional methods such as ESTs and the dormia basket-assisted method. Rates of complication such as pancreatitis and bleeding were acceptable (13). Large bile duct stones usually require ML even after sphincterotomies have been performed. In contrast, LBPDs require secondary techniques much less frequently for removal of bile duct stones.
A study by Minami et al. in Japan demonstrated that a combination of a small endoscopic sphincterotomy plus LBPD prevented eliminated the need to use MLs in 99% of their patients with large bile duct stones. In addition, the rate of pancreatitis that resulted was only 1% (14). Another Japanese group led by Itoi reported similar results. They demonstrated that by performing LBPDs, MLs were much less frequently required (25% versus 6%), plus procedure times were shorter (35 versus 40 minutes), and fluoroscopy performance times were also shorter (13 versus 22minutes) than when the EST method was used (8). In India, Maydeo and Bhandari reported a series of 60 patients treated with LBPDs after unsuccessful attempts at stone removal using sphincterotomies and balloon or basket-assisted methods. They were able to completely remove all stones in 57 of these patients (95%). Three patients needed additional mechanical lithotripsy to remove their stones. Slight to moderate bleeding presented in 8.3% of these patients (10). Misra and Dwivedi in India performed LBPDs on 50 patients using 15 to 20 mm diameter balloons after sphincterotomies had been performed and after attempts using balloon and dormia basket methods had failed. The stones were then removed with balloon or dormia basket methods from 29 patients (58%). MLs were only required for 5 patients (10%). Bleeding which stopped without intervention occurred in 16 patients (32%), while one patient who suffered severe bleeding required surgical treatment. Mild acute pancreatitis occurred in 4 patients (8%). No perforations or deaths were reported in this study (9).
A multicentric study of 103 patients with large bile duct stones performed in the United States by Attasaranya et al. reported the potential efficacy of using balloons over 12mm in diameter following endoscopic sphincterotomies. Their combined techniques had a 95% success rate for stone removal during the first session. Twenty-nine patients (27%) required mechanical lithotripsy. Six out of the 103 (5.4%) patients developed some kind of complication, including one patient who developed severe bleeding and one who suffered a severe perforation of the cystic duct (5). Although these studies have shown the usefulness of this technique for treating difficult bile duct stones, controlled clinical assays must be done to determine the efficacy and safety of LBPDs alone and to compare this method with ESTs. In a recent study, Heo et al. in Korea randomized 200 consecutive patients who had bile duct stones into two groups of 100 patients in order to compare the results after performance of complete sphincterotomies on one group of patients and small sphincterotomy (a third of the last group) followed by LBPDs using 12 to 20 mm diameter balloons. The results were similar for the two groups: 97% vs. 98% success rates for the removal of stones (>15 mm), 94.4% vs. 96.7% success rates for the removal of large stones, and 8% vs. 9% of patients who required the use of mechanical lithotripsy. Complication rates were also similar in both groups (6).
In a recent study published by a group from Greece, 90 patients with large bile duct stones (12-20 mm) were randomized for treatment with the EST followed by either ML or LBPD. The group treated with LBPDs had a 97.7% success rate for complete stone removal while the success rate for the group treated with ML was 91.1% (P = 0.36). Complication rates for pancreatitis and similar hemorrhaging were similar for both groups (15).
During the first clinical assays of LBPD the main concern was the risk of developing pancreatitis following the procedure. However, to date there have been no reports of severe pancreatitis, and the incidence of pancreatitis is similar to that observed followings ESTs. Digestive bleeding has been the most frequent complication in studies of LBPD, but in most cases it has been a mild complication which has not required surgical intervention. Perforation is another complication that has been described in some studies. Nevertheless, its incidence has been rare and it can be avoided by following certain indications and by adequately choosing patients who will undergo LBPDs.
To date only a few publications world-wide have evaluated the effectiveness and safety of LBPD after the performance of sphincterotomies. This is the first publication in our community about the use of this technique.
This was a retrospective study of 20 patients who had undergone LBPD to remove bile duct stones. Most of these patients had had previous ERCPs combined with sphincterotomies and the use of conventional devices such as the dormia basket which had not successfully removed stones. ML had also been used in some cases without success. The presence of large bile duct stones and disproportion between the size of the stones and the papillary orifice are indications to for using the LBPD technique. The resolution rate of choledocholithiasis using LBPD in this study was 95%, and most removals were accomplished in one session. 63% of the patients did not require the use of ML for total stone removal. This is important since one of our aims was to avoid the use of ML for treatment of large bile duct stones.
The main complications were digestive bleeding and pancreatitis which occurred in 10% of the patients. However, these complications were mild and all patients evolved satisfactorily. Our rate of complications using this technique correlates to those described in the literature. Pancreatitis, a complication that concerned many authors when this procedure began to be used, developed in only one patient in this study, and it was a mild case. This result supports the concept that attempting an EST prior to the use LBPD diminishes the risk of pancreatitis. Neither severe complications, such as perforations, nor deaths occurred among the patients studied.
In conclusion, even though this was a preliminary study, the results show that LBPD is an efficacious and safe technique for treating difficult cholecholithiasis. Moreover, most patients had no need for the use of other techniques such as mechanical lithotripsy for the removal of large bile duct stones.
REFERENCES
1. Freitas ML, Bell RL, Duffy AJ. Choledocholithiasis: Evolving standards for diagnosis and management. World J Gastroenterol 2006; 12(20): 3162-3167.
2. van Erpecum KJ. Complications of bile-duct stones: acute cholangitis and pancreatitis. Best Practice & Research Clinical Gastroenterology 2006; 20: 1139e1152.
3. Lee DK, Jahng JH. Alternative methods in the endoscopic management of difficult common bile duct stones. Digestive Endoscopy 2010; 22(Suppl 1): S79-S84.
4. Hisatomi K, Ohno A, Tabei K, Kubota K, Matsuhashi N. Effects of large-balloon dilation on the major duodenal papilla and the lower bile duct: histological evaluation by using an ex vivo adult porcine model. Gastrointestinal Endoscopy 2010; 72(2): 366-72.
5. Siriboon Attasaranya, Young Koog Cheon, Harsha Vittal, Douglas A. Howell, et al. Large-diameter biliary orifice balloon dilation to aid in endoscopic bile duct stone removal: a multicenter series. Gastrointestinal Endoscopy 2008; 67(7): 1046-52.
6. Heo JH, Kang DH, Jung HJ, Kwon DS, et al. Endoscopic sphincterotomy plus large-balloon dilation versus endoscopic sphincterotomy for removal of bile-duct stones. Gastrointestinal Endoscopy 2007; 66(4): 720-6; quiz 768, 771.
7. Kim Hyun Gun, Cheon Young Koog, Cho Young Deok, Moon Jong Ho, et al. Small sphincterotomy combined with endoscopic papillary large balloon dilation versus sphincterotomy. World J Gastroenterol 2009; 15(34): 4298-304.
8. Tsuji S, Ikeuchi N, Moriyasu F. Endoscopic Sphincterotomy Combined with Large Balloon Dilation can reduce the Procedure Time and Fluoroscopy Time for Removal of Large Bile Duct Stones. Am J Gastroenterol 2009; 104: 560-565; doi: 10.1038/ajg.2008.67; published online 27 January 2009.
9. Misra SP, Dwivedi M. Large-diameter balloon dilation after endoscopic sphincterotomy for removal of difficult bile duct stones. Endoscopy 2008; 40: 209-213.
10. Maydeo A, Bhandari S. Balloon sphincteroplasty for removing difficult bile duct stones. Endoscopy 2007; 39: 958-961.
11. Rajeev Attam, Martin L. Freeman. Endoscopic papillary large balloon dilation for large common bile duct stones. J Hepatobiliary Pancreat Surg 2009; 16: 618-623.
12. Kyeong Ok Kim, Tae Nyeun Kim, Si Hyung Lee. Endoscopic papillary large balloon dilation for the treatment of recurrent bile duct stones in patients with prior sphincterotomy. J Gastroenterol DOI 10.1007/s00535-010-0284-7.
13. Ersoz G, Tekesin O, Ozutemiz AO, Gunsar F. Biliary sphincterotomy plus dilation with a large balloon for bile duct stones that are difficult to extract. Gastrointest Endosc 2003; 57: 156-159.
14. Minami A, Hirose S, Nomoto T, Hayakawa S. Small sphincterotomy combined with papillary dilation with large balloon permits retrieval of large stones without mechanical lithotripsy. World J Gastroenterol 2007; 13(15): 2179-2182.
15. Stefanidis G, Viazis N, Pleskow D, Manolakopoulos S, Theocharis L, Christodoulou C, et al. Large Balloon Dilation vs. Mechanical Lithotripsy for the Management of Large Bile Duct Stones. A Prospective Randomized Study. Am J Gastroenterol advance online publication, 2 November 2010; doi: 10.1038/ajg.2010.421.
1. Freitas ML, Bell RL, Duffy AJ. Choledocholithiasis: Evolving standards for diagnosis and management. World J Gastroenterol 2006; 12(20): 3162-3167. [ Links ]
2. van Erpecum KJ. Complications of bile-duct stones: acute cholangitis and pancreatitis. Best Practice & Research Clinical Gastroenterology 2006; 20: 1139e1152. [ Links ]
3. Lee DK, Jahng JH. Alternative methods in the endoscopic management of difficult common bile duct stones. Digestive Endoscopy 2010; 22(Suppl 1): S79-S84. [ Links ]
4. Hisatomi K, Ohno A, Tabei K, Kubota K, Matsuhashi N. Effects of large-balloon dilation on the major duodenal papilla and the lower bile duct: histological evaluation by using an ex vivo adult porcine model. Gastrointestinal Endoscopy 2010; 72(2): 366-72. [ Links ]
5. Siriboon Attasaranya, Young Koog Cheon, Harsha Vittal, Douglas A. Howell, et al. Large-diameter biliary orifice balloon dilation to aid in endoscopic bile duct stone removal: a multicenter series. Gastrointestinal Endoscopy 2008; 67(7): 1046-52. [ Links ]
6. Heo JH, Kang DH, Jung HJ, Kwon DS, et al. Endoscopic sphincterotomy plus large-balloon dilation versus endoscopic sphincterotomy for removal of bile-duct stones. Gastrointestinal Endoscopy 2007; 66(4): 720-6; quiz 768, 771. [ Links ]
7. Kim Hyun Gun, Cheon Young Koog, Cho Young Deok, Moon Jong Ho, et al. Small sphincterotomy combined with endoscopic papillary large balloon dilation versus sphincterotomy. World J Gastroenterol 2009; 15(34): 4298-304. [ Links ]
8. Tsuji S, Ikeuchi N, Moriyasu F. Endoscopic Sphincterotomy Combined with Large Balloon Dilation can reduce the Procedure Time and Fluoroscopy Time for Removal of Large Bile Duct Stones. Am J Gastroenterol 2009; 104: 560-565; doi: 10.1038/ajg.2008.67; published online 27 January 2009. [ Links ]
9. Misra SP, Dwivedi M. Large-diameter balloon dilation after endoscopic sphincterotomy for removal of difficult bile duct stones. Endoscopy 2008; 40: 209-213. [ Links ]
10. Maydeo A, Bhandari S. Balloon sphincteroplasty for removing difficult bile duct stones. Endoscopy 2007; 39: 958-961. [ Links ]
11. Rajeev Attam, Martin L. Freeman. Endoscopic papillary large balloon dilation for large common bile duct stones. J Hepatobiliary Pancreat Surg 2009; 16: 618-623. [ Links ]
12. Kyeong Ok Kim, Tae Nyeun Kim, Si Hyung Lee. Endoscopic papillary large balloon dilation for the treatment of recurrent bile duct stones in patients with prior sphincterotomy. J Gastroenterol DOI 10.1007/s00535-010-0284-7. [ Links ]
13. Ersoz G, Tekesin O, Ozutemiz AO, Gunsar F. Biliary sphincterotomy plus dilation with a large balloon for bile duct stones that are difficult to extract. Gastrointest Endosc 2003; 57: 156-159. [ Links ]
14. Minami A, Hirose S, Nomoto T, Hayakawa S. Small sphincterotomy combined with papillary dilation with large balloon permits retrieval of large stones without mechanical lithotripsy. World J Gastroenterol 2007; 13(15): 2179-2182. [ Links ]
15. Stefanidis G, Viazis N, Pleskow D, Manolakopoulos S, Theocharis L, Christodoulou C, et al. Large Balloon Dilation vs. Mechanical Lithotripsy for the Management of Large Bile Duct Stones. A Prospective Randomized Study. Am J Gastroenterol advance online publication, 2 November 2010; doi: 10.1038/ajg.2010.421. [ Links ]

