










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.2 Bogotá abr./jun. 2011
Hilar Cholangiocarcinoma (Klatskin tumor)
Rodrigo Castaño Llano, MD (1)
(1) Gastrointestinal Surgeon and Endoscopist. Professor in the Gastro-hepatology group at the Universidad de Antioquia. Professor of Surgery at the Universidad Pontificia Bolivariana. Hospital Pablo Tobón Uribe. Medellin, Colombia.
Received: 23-05-11 Accepted: 01-06-11
Abstract
This is a clinical case of a 71-year-old man with an obstructive lesion of the hepatic hilum, the clinical, imaging studies and the lab tests suggest a Klatskin tumor, which was managed by percutaneous biliary drainage to relieve the jaundice. In this review we consider the pathogenetic factors of these tumors, a new anatomic classification and the various alternative imaging studies, emphasizing the Bismuth-Corlette classification. Confront palliative alternatives, such as different types of endoscopic stents or percutaneous approach, drainage extension (uni or bilateral). Finally, we review the surgical aspects and possibilities of chemotherapy and radiotherapy in these tumors.
Key words
Hilar cholangiocarcinoma, endoscopic retrograde cholangiography, nuclear magnetic resonance cholangiography, hepatobiliary surgery.
CLINICAL CASE
A 71 year old male patient consulted after one month of suffering right upper quadrant pain associated with acholia, choluria and generalized jaundice with episodes of subjective fever.
Important antecedents included arterial hypertension and an open cholecystectomy 9 years earlier. In the examination of his systems, the fact that he had lost approximately 10k of weight stood out.
Upon physical examination the patient was found to be hemodynamically stable with generalized jaundice. Upon abdominal palpation the patient mentioned pain in the upper right quadrant, but with no signs of peritoneal irritation. No masses or organomegalies were felt. The rest of the physical examination was normal.
The following paraclinical test results should be highlighted: CBC without signs of anemia or abnormal leukocytes. Aspartate aminotransferase (AST) 61 U/L, Alanine aminotransferase (ALT) 92 U/L, Amylase 62 mg/dl, direct bilirubin 16 mg/dl, total bilirubin 22.8 mg/dl and alkaline phosphatase 253 U/L.
In hepatobiliary ultrasound images the liver appeared heterogeneous and oversized with intrahepatic and extrahepatic biliary ducts dilated to 13 mm. In addition the sonography showed that the patient suffered from postcholecystectomy syndrome. No possible etiologies for the dilated bile duct could be discerned from the sonograms. Magnetic resonance cholangiopancreaticography showed a dilated intrahepatic bile duct, but did not show the confluence of the hepatic ducts or the proximal common bile duct. Dilation of the distal common bile duct to a diameter of 8 mm was also observed. There were no gaps in the images which would suggest the presence of calculi. (Figures 1 and 2).
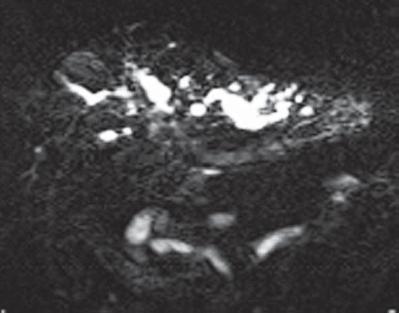
Figure 1. Marked dilated intrahepatic bile duct without the confluence of the hepatic ducts or the proximal common bile duct.
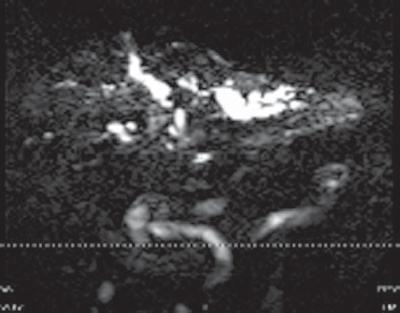
Figure 2. No confluence of the hepatic ducts or the proximal common bile duct, no filling defects that would suggest the presence of calculi.
Based on our findings the main possibility considered was a Bismuth-Corlette type IV Klatskin tumor. Tumor extension studies were performed. X-rays of the thorax showed no pulmonary parenchymal or pleural effusion. Abdominal CT scans showed neither liver compromise nor compromise of the lymph nodes, nor vascular involvement. Doppler ultrasound showed normal portal venous blood flow. Due to the high location of the hilar tumor an endoscopic bypass of the bile duct was not performed. Instead a percutaneous biliary bypass was performed. It showed a stenosing lesion at the hepatic duct confluence. The lesion was opened with a catheter, adequately bypassing the bile duct. (Figures 3 and 4).
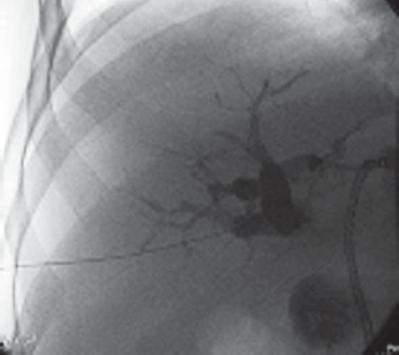
Figure 3. Percutaneous puncture of the right lobe with right hepatic amputation. The left side has been drained and the catheter can be seen.
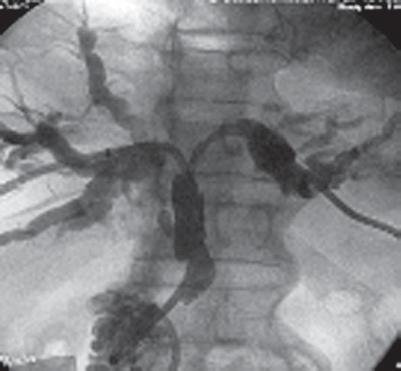
Figure 4. Right and left hepatic catheters with perceivable dilation of the secondary ducts of both lobes.
Due to the degree of intrahepatic involvement, it was determined that the patient was not a candidate for surgery; therefore, studies had to be completed on an outpatient basis (tumor markers, albumin and protein totals) to determine palliative chemotherapy. The patient has evolved satisfactorily and has been discharged.
INTRODUCTION
Bile duct carcinomas, or cholangiocarcinomas (CCs), originate in the epithelial cells of the intrahepatic and extrahepatic bile ducts. While these tumors have a low incidence, they have high mortality rates because the level of compromise is advanced when they appear. The most relevant controversial aspects related to the management of this tumor are reviewed below.
ANATOMY: CLASSIFYING AND STAGING A CHOLANGIOCARCINOMA
Tumors in the bile duct have traditionally been divided into gallbladder carcinoma, extrahepatic bile duct carcinoma and ampulla of Vater carcinoma. Intrahepatic tumors have been classified as primary biliary tumors (Figure 5).
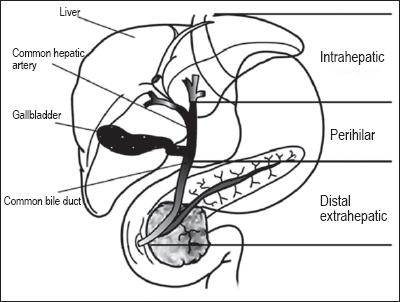
Figure 5. Classification of bile duct tumors.
More recently, the term "cholangiocarcinoma" has been used to refer to tumors in the intrahepatic bile ducts, perihilar bile ducts (Klatskin tumor) or distal bile ducts (extrahepatic). This term is not used for gallbladder tumors and tumors in the ampulla of Vater (1). Approximately 60% to 70% originate in the hepatic duct confluence. Although some studies mistakenly consider them to be intrahepatic, most recently they have been categorized based on their topographic place of origin (2). Extrahepatic tumors are divided into perihilar and distal with the boundary set at the common bile duct posterior to the duodenum.
Perihilar tumors were classified in 1965 by Klatskin (3). More recently the Bismuth-Corlette classification has classified them according to the involvement of one or both hepatic ducts (4) (Figure 6).
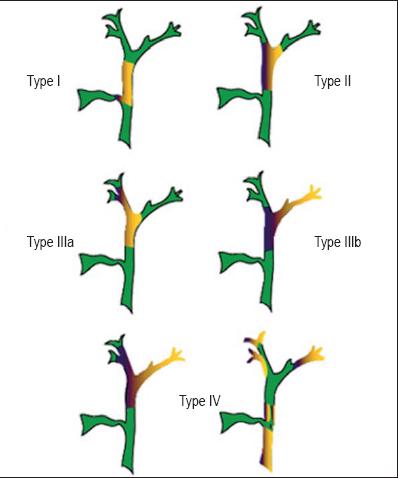
Figure 6. Bismuth-Corlette classification of perihilar cholangio-carcinomas. The yellow or purple areas represent the tumors. Green areas are normal. Type I: Below the hepatic confluence. Type II: involvement of the confluence. Type IIIa and IIIb: involvement of the confluence and the right lobe (a) or left lobe (b); and Type IV: Tumor in both hepatic lobes, multicentric.
Recently, the American Joint Committee on Cancer (AJCC) classification separated cholangiocarcinomas into intrahepatic, perihilar and extrahepatic or distal (5). Intrahepatic tumors are classified independently of hepatocellular carcinomas by different variables that affect their prognoses. An odd presentation combines characteristics of a hepatocellular carcinoma and CC and is intrahepatically located. This separation of perihilar and distal tumors aims to provide improved predictions of life expectancy with the TNM staging system which was created in response to criticism of previous classification systems that did not adequately predict the life expectancies of patients with these tumors (6).
What risk factors can lead to cholangiocarcinomas?
Although different risk factors have been suggested, primary sclerosing cholangitis (PSC) and common bile ductal cysts are amongst the most widely recognized. Nevertheless, for most patients including the one presented in this article, no clear risk factor is ever identified.
A. Primary sclerosing cholangitis (PSC) is an inflammatory disorder that causes fibrosis and stenosis in both intrahepatic and extrahepatic bile ducts. Forty to fifty percent of these patients present active ulcerative colitis. Close to 30% of CC cases have PSC with or without ulcerative colitis. The annual risk of CC associated with PSC is 0.6% to 1.5%. CC appears at earlier ages among patients with PSC (30 to 50 years old) (7). Tumor markers alone may indicate a mistaken diagnosis. Recently, in a study of patients with PSC and malignant appearing biliary stenoses, a value greater than 100 U/ml was set for performing adjuvant chemotherapy treatment without making histological diagnoses (8).
B. Polycystic liver disease. Congenital anomalies of the bile duct (Caroli disease, congenital hepatic fibrosis, common bile ductal cysts) have a 15% risk for the development of CC in adulthood. Common bile ductal cysts are an expansion of bile ducts while Carolis disease is a variation of common bile ductal cysts characterized by dilations of the intrahepatic biliary tree. The etiopathogenesis of cancer in these patients is related to biliary stenosis, chronic inflammation due to pancreatic reflux, unstable bile content or decomposed carcinogens (9).
C. Parasitic disease. In the East, there are recognized biliary parasites (Clonorchis sinensis and Opistorchis viverrini) associated with CC. They induce chronic inflammation which has been related to the malignant transformation of the epithelium (2).
D. Colelithiasis and hepatolithiasis. The relation between vesicular calculi and CC is not as B as that between cholethiasis and vesicular cancer. The clearest existing relation between hepothiliasis and CC is in Taiwan where 70% of the patients who have hepatic resections due to CC, also have hepatolithiasis (10).
E. Exposure to toxins. There is a clear association between exposure to Thorotrast (a radiological contrast agent used during the 60s) and the appearance of cholangiocarcinomas. Other agents implicated include plastics, chemicals and wood finishers. Studies on the relation of CCs to alcohol and cigarette use are contradictory (11).
F. Lynch syndrome and biliary papillomatosis. Lynch syndrome, or non-polyposis colorectal cancer, is a dominant autosomal hereditary disorder which has a high risk of leading not only to colon cancer, but also to ovarian, endometrial, brain and skin cancer related to the presence of CC (12). Biliary papillomatosis has been considered a preneoplastic condition since its first description. It is related to CC in up to 83% of patients (13).
G. Chronic liver disease. The hepatitis B virus (HBV), hepatitis C virus (HCV) and cirrhosis have all been associated with intrahepatic CC. Even though the risk is lower for hepatocellular carcinoma, it has been estimated that in Japan (14) HCV infections increased the risk 3.5 times over a 10 year period; while in the United States this risk is 2.55 times greater (15). A Danish study of 11,605 cirrhosis patients showed that cirrhosis patients have 10 times greater risk for CC than does the general population (16).
H. HIV infection. HIV infections have been associated with a risk of CC up to 6.4 times greater. The validity of this association is uncertain because of the small number of cases, and the possibility that there are unidentified coexisting risk factors such as HCV (17).
What are the clinical manifestations of cholangiocarcinomas? and what is the differential diagnosis for right upper quadrant pain?
CC is clinically expressed by obstruction of biliary drainage which leads to painless jaundice. Frequent symptoms include pruritus (66%), abdominal pain (40% to 50%), weight loss (40% to 50%) and fever (20%). There is constant dull pain in the upper right quadrant. In these cases, cholangitis is rare, as is painless gallbladder growth (sign of Courvoisier). Perihilar and distal lesions are manifested by jaundice while intrahepatic lesions are manifested by pain.
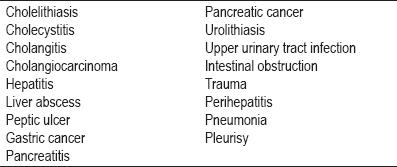
The triad of cholestasis, abdominal pain and weight loss suggests pancreatic or hepatobiliar neoplasia. Differential diagnoses of pain in the upper right quadrant are shown in Table 1.
Table 1. Causes of pain in the upper right quadrant.
Age plus clinical findings of jaundice, pain and notable weight loss led to a diagnosis of a neoplastic origin for this patients symptoms.
What is the role of paraclinical tests in diagnosing cholangiocarcinomas?
Laboratory findings in these cases suggest a cholestatic pattern with increased bilirubin at the expense of direct bilirubin with increased alkaline phosphatase and gamma glutamyl transpeptidase. Tumor markers are not specific. CA 19-9 is not a specific marker for CC since it is increased not only in cases of cholangiocarcinoma but also in gastric cancer, colorectal cancer, esophageal cancer, hepatocellular cancer; benign entities, and in acute cholangitis and pancreatitis. Use of the carcinoembryonic antigen and CA 19-9 as markers has been suggested when values are greater than 5.2 ng/ml and 180 U/ml since the sensitivity is 100% and the specificity is 78% (18).
What value do ultrasound, abdominal CAT scans using contrast agents, MRIs and endoscopic ultrasound have for the diagnosis of cholangiocarcinoma?
Imaging studies lead us to establish the cause of biliary obstruction by discriminating between benign and malignant lesions. In addition, they help us plan how to deal with our patient. Endoscopic cholangiography has a purely therapeutic role, hence is not included in the diagnosis of obstructive biliary lesions.
A. Abdominal ultrasound is indicated for initial study of any patient with jaundice. It is used to confirm whether or not there is any biliary dilation, and if there is, to confirm its location. It can also locate an obstruction and exclude or confirm the presence of gallbladder calculi. An evaluation for hilar or distal stenosis is slightly different. For hilar lesions, an MRI is the study of choice. An intrahepatic lesion appears as a mass while hilar or distal lesions are smaller and cannot be observed except through indirect signs such as when there are ductal dilations greater than 6mm in adults. Nevertheless, biliary dilation may not be apparent in PSC and cirrhosis (19).
B. Another contribution of ultrasound is that Doppler ultrasound makes it possible to evaluate vascular involvement resulting from compression, tumor invasion or portal thrombosis, and to evaluate compression and invasion of the hepatic artery. Invasion of the hepatic artery rules out surgery.
C. Abdominal CAT scans with contrast are useful for detecting intrahepatic lesions, determining the level of obstruction and for determining whether or not atrophy is present. The location of ductal dilation suggests the location of the obstruction:
- Bilobar ductal dilation with a contracted gallbladder or disjunction of the hepatic lobes, with or without thickening, suggests a Klatskin tumor. In contrast, a relaxed gallbladder with no dilation of the intrahepatic or extrahepatic bile ducts is most common in choledochal tumors, cancer of the ampulla of Vater, and pancreatic cancer.
- The dilation of the bile ducts in an atrophic lobe paired with compensatory contralateral hypertrophy suggests an invasion of the portal vein (20).
Three phase helical CT scans allow better discrimination of intrahepatic biliary stenoses, especially in the portal vein phase. They also allow visualization of hilar lymph nodes. However, even though multiphase CT is still superior to MRI (21) for evaluating the magnitude of intraductal involvement and the resectability of a lesion (22), its utility is still limited.
D. Magnetic Resonance Imaging. Magnetic resonance cholangiopancreatography (MRCP) has replaced retrograde endoscopic cholangiography (REC) as a diagnostic method. Besides being able to evaluate parenchymal and intrahepatic lesions, it can create a three dimensional image of the biliary tree which allows us to evaluate the bile duct above and below an obstruction. Series that compare endoscopic cholangiography to MRI show that while both methods show 100% of an obstruction, MRIs are superior for defining anatomical involvement and causes of jaundice (23). Known limitations of MRIs include an underestimation of obstruction by up to 20% and a requirement for highly trained personnel almost exclusively dedicated to performing this procedure with a high degree of reliability.
E. Cholangiography may be endoscopic or percutaneous. The choice is largely defined by availability and the experience of the institution. Cholangiography is indicated for biliary obstructions for drainage of a bile duct when needed. Many surgeons prefer images from endoscopic or percutaneous cholangiography over MRIs for defining the extent of surgery. Another option for endoscopic cholangiography is brushing for a cytological study or a biopsy, but different series have shown inconsistent results. Locally, the only experience with this technique has been with brushing distal lesions (24) (Figure 7).

Figure 7. Sequence of biliary brushing of malignant appearing stenoses . A. Biliary stenosis and Bismuth-Corlette (III a) tumor in the confluence. B. The transpapillary guide and the trail of the brush can be observed. C. Path of the brush and a plastic stent in biliary stenosis.
After biliary biopsy or brushing a stent must be placed to guarantee biliary drainage.
F. Endoscopic ultrasound. Although its utility for evaluating hilar involvement is limited, for distal neoplasias it allows the extension of a tumor to be determined and, through fine needle aspiration, lets us determine the state of the lymph nodes with even greater sensitivity than biliary brushing. It also avoids the contamination of the bile duct observed with ERCP (25). In addition, it has also been found to be more sensitive than CAT scans and angiography for evaluating portal vascular involvement (26).
G. Positron emission tomography (PET) allows CCs to be visualized because of their high glucose uptake (27). PET scans are very useful in nodular formulas even when lesions are less than a centimeter, but they are less useful for infiltrating lesions. However, their primary role lies in identifying hidden metastases (28).
What preoperative drainage imply?
Preoperative biliary drainage does not interfere with additional surgery the future. However, the benefits of preoperative endoscopic drainage for the outcome of surgery are debatable (29, 30). Whether or not stents should be used is debated because they can cause local distortions in images used for evaluation. According to some surgeons the presence of the stent does not allow determination of the proximal extension of the tumor during resection. Stents are also related to a greater incidence of post-surgical infections. Arguments in favor of decompression using stents include the facts that placement of stents rapidly stabilizes cholestasis, hepatic dysfunction and biliary cirrhosis following an obstruction while continued hepatic dysfunction after resection conditions greater post operative morbidity and mortality (31). Western groups prescribe stenting for biliary drainage very selectively only when the duration of jaundice is greater than two weeks, the level of bilirubin is greater than10gr/dl), cholangitis is present, or when the size of the hepatic remnant will be less than 30% (32). In contrast, Asian authors almost always prescribe stenting. Patients who are less than 60 years old whose nutritional status is good (albumin greater than 3.5 gr/dl) can be operated on when their bilirubin levels are higher than 10 gr/ dl as long as no biliary infection is present. In contrast to preoperative biliary bypass according to Whipple, preoperative biliary bypasses in hepatic resections seem to benefit from previous biliary drainage (33).
Which method is preferable, endoscopic or percutaneous?
I share Costamagnas opinion (34) that endoscopic drainage should always be tried first, but if it is not feasible percutaneous drainage should be tried. Ideally, there should be a good evaluation of the lesions images prior to determining resectability and placement of a stent. Definite surgical intervention in resectable cases is recommended when bilirubin levels are less than 3 gr/dl. A recent study of ours showed no differences in morbidity, mortality and life expectancy between proximal malignant biliary obstructions and distal malignant biliary obstructions (35).
Which stent is indicated: plastic or metal, covered or uncovered?
Studies suggest that metallic stents are preferable to plastic ones (36, 37), although doubts and controversies regarding the use of covered or uncovered stents remain. Studies that compare both stents in distal obstructions do not show either type of stent to have greater permeability than the other, however covered stents have a greater tendency to migrate than do uncovered ones. When the cystic ostium is occluded in patients with gallbladders in situ the use of uncovered stents is preferable in order to avoid cholecystitis. Uncovered stents are also preferable in cases of obstructions due to extrinsic compression of the hepatic hilum, and they prevent occlusion of contralateral drainage.
Should drainage by stenting of one or both hepatic lobes be preferred?
In most cases drainage of one lobe is sufficient since drainage of 30% of the liver is enough to relieve jaundice. Nevertheless, relief of jaundice will not be complete, leaving a risk for cholangitis. A good study of images of the lesion prior to the procedure should determine the dominant obstruction in case only one side can be drained. Da Palmas (38) work is the only prospective and randomized study which compares unilateral stents and bilateral stents. That study does not demonstrate lower morbidity and mortality rates for bilobar drainage which is why routine bilateral drainage is not recommended. Recently, Viennes study (39) has suggested that success of a procedure is determined more by which segment is chosen for drainage than it is by the number of stents used. More than 30% of hepatic volume must be drained, and life expectancy increases when drained volume is greater than 50%.
When is surgery indicated for a patient with cholangiocarcinoma?
Patients with these tumors have poor prognoses: only 10% have life expectancies of five years. Surgery is the only feasible option. 90% of distal CCs are require surgery, more than cholangiocarcinomas in any other location, while hilar cholangiocarcinomas require resection in 56% of cases, the least of any location (40). (Figure 5).
Resections, including those intended to cure, have clear margins in only 20% to 40% of proximal CC cases and in only 50% of distal tumor cases. This number is reduced, especially in proximal tumors, if it is considered that a 5 mm margin is necessary for the procedure. However, resectability rates in these tumors have increased due to a more aggressive surgical strategy and broader criteria for respectability (41). The American criteria for CC resection are:
- Absence of tumor involvement in the retropancreatic lymph nodes and the celiac artery and absence of distant metastases
- No invasion of the portal vein of the main hepatic artery (even though some institutions perform vascular reconstruction in these cases)
- Absence of invasion in neighboring organs
- No disseminated disease
Despite the above, true resectability is only determined in surgery. This is especially true for perihilar tumors (Klatskin) for which laparoscopic staging has increasingly more limited value because of the consolidation of imaging studies (42). At the time of surgery, the main negative determinants for the patients prognosis are the presence of lymph nodes and a positive tumor margin (43, 44).
The extent of the surgery depends on the Bismuth-Corlette classification (Figure 6) for type I and type II lesions. The procedure consists in both removal en bloc of the extrahepatic bile ducts and the biliary gallbladder with a margin no less than 5 mm, and a regional lymphadenectomy with Roux-en-Y hepaticojejunostomy. Type III lesions also require hepatic lobectomies. Some even require surgery of the caudate lobe because of its frequent involvement (41). These operations should be performed in institutions with trained specialists and particular interests in these lesions.
Other factors that imply poor prognoses include transmural involvement including the biliary gallbladder, adenosquamous carcinomas (which are more aggressive than papillary histologic carcinomas), male gender (men have shorter life expectancies in these cases), preoperative albumin levels lower than 3 gr/ dl and bilirubin levels over 10 mg/dl.
What is the role of chemotherapy in treating cholangiocarcinomas?
Between 60% and 90% of CC patients are not suitable for resection at the moment they are diagnosed (40). The life expectancy of these patients is only a few months, and palliation is oriented toward controlling pain, jaundice and pruritus. The optimum management of patients with advanced inoperable or recurrent CC is uncertain. Management guides from expert groups such as the National Comprehensive Cancer Network (NCCN) (45) suggest:
- Extrahepatic Cholangiocarcinoma: Fluoropyrimidine or gemcitabine based chemotherapy is recommended together with palliative care for patients with unresectable disease.
Patients with a positive margin after resection should receive chemotherapy with fluoropyrimidine.
- Intrahepatic Cholangiocarcinoma: For patients with unresectable disease fluoropyrimidine or gemcitabine based chemotherapy is recommended together with palliative care or ablative therapy (radio frequency, cryotherapy or microwave ablation). Patients with a positive margin after resection should receive re-resection, ablation or radio therapy, with or without chemotherapy with fluoropyrimidine or gemcitabine.
On the other hand, the European Society of Medical Oncology (ESMO) (46) suggests:
- After non-healing surgery for intrahepatic or extrahepatic CC, palliative care and chemotherapy and/or radiotherapy.
- For unresectable CCs, photodynamic therapy with palliative chemoradiotherapy
Are liver transplants indicated for patients with hilar cholangiocarcinoma?
Orthotopic liver transplantations (OLTs) have had varied results when performed for tumors at the hepatic confluence and for intrahepatic CC (47, 48). In some cases, patients have received transplants because of sclerosing cholangitis and CCs were found incidentally. Interest in OLTs arose from the experience of the Mayo Clinic which reported that 82% of a group of patients in their study had five year life expectancies. These patients had CCs associated with sclerosing cholangitis and had been declared inoperable. After receiving chemotherapy laparotomies were performed to rule out metastases then these patients received orthotopic liver transplantations (8). Nevertheless, it is striking that no viable tumor was found in 16 of the explants while seven these patients had not been diagnosed histologically to discovery of their tumors. This suggests the possibility of prior erroneous diagnoses. A more recent intention to treat (ITT) analysis from the Mayo Clinic of patients in the protocol, transplanted or not, found life expectancies ranging from 1.3 to 5 years in 82%, 63% and 55% (49).
A systematic review by the Agency for Healthcare Research Quality highlights the following conclusions:
- An analysis of studies which included ten or more patients (a total of 543 patients) concluded that average life expectancy was 11.8 months. 63% of the patients in those studies had life expectancies of one year, 46% had life expectancies of three years, and 22% had life expectancies of five years. For patients who underwent OLTS for hepatitis C, 79% had life expectancies of one year, 79% had life expectancies of three years, and 66% had life expectancies of five years.
- The rate of relapse was 52%. 58% of these patients had life expectancies of one year, 22% had life expectancies of three years, and 13% had life expectancies of five years.
- There was not enough data to determine whether CC or OLT led to a better or worse prognosis. However, patients who had no incidental findings, were negative for lymph node metastases and had no residual disease had better outcomes.
In conclusion, OLT should not yet be considered as standard therapy for localized CCs. It should only be considered for select cases of patients with inoperable hilar lesions who have completed rigorous staging with neoadjuvant therapy which is only possible in a few institutions performing OLTs (50).
REFERENCES
1. Welzel TM, McGlynn KA, Hsing AW, OBrien TR, Pfeiffer RM. Impact of classification of hilar cholangiocarcinomas (Klatskin tumors) on the incidence of intra- and extrahepatic cholangiocarcinoma in the United States. Journal of the National Cancer Institute 2006; 98: 873-5.
2. Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD. Cholangiocarcinoma. Lancet 2005; 366: 1303-14.
3. Klatskin G. Adenocarcinoma of the Hepatic Duct at Its Bifurcation within the Porta Hepatis. An Unusual Tumor with Distinctive Clinical and Pathological Features. The American journal of medicine 1965; 38: 241-56.
4. Bismuth H, Corlette MB. Intrahepatic cholangioenteric anastomosis in carcinoma of the hilus of the liver. Surg Gynecol Obstet 1975; 140: 170-8.
5. Edge SB, Byrd DR, Compton CC. Cancer Staging Manual AJCC (American Joint Committee on Cancer) 7ed. New York: Springer; 2010.
6. Farges O, Fuks D, Le Treut YP, et al. AJCC 7th edition of TNM staging accurately discriminates outcomes of patients with resectable intrahepatic cholangiocarcinoma: By the AFC-IHCC-2009 study group. Cancer 2011; 117: 2170-7.
7. Tyson GL, El-Serag HB. Risk factors of cholangiocarcinoma. Hepatology 2011.
8. Rea DJ, Heimbach JK, Rosen CB, et al. Liver transplantation with neoadjuvant chemoradiation is more effective than resection for hilar cholangiocarcinoma. Ann Surg 2005; 242: 451-8; discussion 8-61.
9. De Martel C, Plummer M, Franceschi S. Cholangiocarcinoma: descriptive epidemiology and risk factors. Gastroenterol Clin Biol 2010; 34: 173-80.
10. Patel T. Cholangiocarcinoma-controversies and challenges. Nature reviews Gastroenterology & hepatology 2011; 8: 189-200.
11. Shaib YH, El-Serag HB, Nooka AK, et al. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: a hospital-based case-control study. Am J Gastroenterol 2007; 102: 1016-21.
12. Mecklin JP, Jarvinen HJ, Virolainen M. The association between cholangiocarcinoma and hereditary nonpolyposis colorectal carcinoma. Cancer 1992; 69: 1112-4.
13. Lee SS, Kim MH, Lee SK, et al. Clinicopathologic review of 58 patients with biliary papillomatosis. Cancer 2004; 100: 783-93.
14. Kobayashi M, Ikeda K, Saitoh S, et al. Incidence of primary cholangiocellular carcinoma of the liver in japanese patients with hepatitis C virus-related cirrhosis. Cancer 2000; 88: 2471-7.
15. El-Serag HB, Engels EA, Landgren O, et al. Risk of hepatobiliary and pancreatic cancers after hepatitis C virus infection: A population-based study of U.S. veterans. Hepatology 2009; 49: 116-23.
16. Sorensen HT, Friis S, Olsen JH, et al. Risk of liver and other types of cancer in patients with cirrhosis: a nationwide cohort study in Denmark. Hepatology 1998; 28: 921-5.
17. Shaib YH, El-Serag HB, Davila JA, Morgan R, McGlynn KA. Risk factors of intrahepatic cholangiocarcinoma in the United States: a case-control study. Gastroenterology 2005; 128: 620-6.
18. Siqueira E, Schoen RE, Silverman W, et al. Detecting cholangiocarcinoma in patients with primary sclerosing cholangitis. Gastrointest Endosc 2002; 56: 40-7.
19. Friman S. Cholangiocarcinoma--current treatment options. Scand J Surg 2011; 100: 30-4.
20. Hann LE, Getrajdman GI, Brown KT, et al. Hepatic lobar atrophy: association with ipsilateral portal vein obstruction. AJR Am J Roentgenol 1996; 167: 1017-21.
21. Feydy A, Vilgrain V, Denys A, et al. Helical CT assessment in hilar cholangiocarcinoma: correlation with surgical and pathologic findings. AJR Am J Roentgenol 1999; 172: 73-7.
22. hang Y, Uchida M, Abe T, Nishimura H, Hayabuchi N, Nakashima Y. Intrahepatic peripheral cholangiocarcinoma: comparison of dynamic CT and dynamic MRI. J Comput Assist Tomogr 1999; 23: 670-7.
23. Yeh TS, Jan YY, Tseng JH, et al. Malignant perihilar biliary obstruction: magnetic resonance cholangiopancreatographic findings. Am J Gastroenterol 2000; 95: 432-40.
24. Ruiz MH, Castaño R, Alvarez O, et al. Evaluación de la citología por cepillado en las estenosis biliares y pancreáticas durante la colangiografía endoscópica retrógrada. Revista Col de Gastroenterol 2002; 17: 222-5.
25. Coelho-Prabhu N, Baron TH. Endoscopic retrograde cholangiopancreatography in the diagnosis and management of cholangiocarcinoma. Clin Liver Dis 2010; 14: 333-48.
26. Sugiyama M, Hagi H, Atomi Y, Saito M. Diagnosis of portal venous invasion by pancreatobiliary carcinoma: value of endoscopic ultrasonography. Abdom Imaging 1997; 22: 434-8.
27. Lee SW, Kim HJ, Park JH, et al. Clinical usefulness of 18F-FDG PET-CT for patients with gallbladder cancer and cholangiocarcinoma. J Gastroenterol 2010; 45: 560-6.
28. Breitenstein S, Apestegui C, Clavien PA. Positron emission tomography (PET) for cholangiocarcinoma. HPB (Oxford) 2008; 10: 120-1.
29. Laurent A, Tayar C, Cherqui D. Cholangiocarcinoma: preoperative biliary drainage (Con). HPB (Oxford) 2008; 10: 126-9.
30. Nimura Y. Preoperative biliary drainage before resection for cholangiocarcinoma (Pro). HPB (Oxford) 2008; 10: 130-3.
31. Su CH, Tsay SH, Wu CC, et al. Factors influencing postoperative morbidity, mortality, and survival after resection for hilar cholangiocarcinoma. Ann Surg 1996; 223: 384-94.
32. Rocha FG, Matsuo K, Blumgart LH, Jarnagin WR. Hilar cholangiocarcinoma: the Memorial Sloan-Kettering Cancer Center experience. J Hepatobiliary Pancreat Sci 2010; 17: 490-6.
33. Cherqui D, Benoist S, Malassagne B, Humeres R, Rodriguez V, Fagniez PL. Major liver resection for carcinoma in jaundiced patients without preoperative biliary drainage. Arch Surg 2000; 135: 302-8.
34. Costamagna G, Mutignani M, Perri V, et al. Results of endoscopic biliary drainage in primary tumors of the common bile duct (cholangiocarcinoma). Chir Ital 1995; 47: 18-23.
35. Castaño R, Ricardo A, Velásquez L, Ruiz MH, Ruiz LM. Desempeño del stent plástico para la paliación en la obstrucción biliar maligna proximal versus distal. Rev Col Gastroenterol 2011; en prensa.
36. Perdue DG, Freeman ML, DiSario JA, et al. Plastic versus self-expanding metallic stents for malignant hilar biliary obstruction: a prospective multicenter observational cohort study. J Clin Gastroenterol 2008; 42: 1040-6.
37. Raju RP, Jaganmohan SR, Ross WA, et al. Optimum palliation of inoperable hilar cholangiocarcinoma: comparative assessment of the efficacy of plastic and self-expanding metal stents. Dig Dis Sci 2011; 56: 1557-64.
38. De Palma GD, Galloro G, Siciliano S, Iovino P, Catanzano C. Unilateral versus bilateral endoscopic hepatic duct drainage in patients with malignant hilar biliary obstruction: results of a prospective, randomized, and controlled study. Gastrointest Endosc 2001; 53: 547-53.
39. Vienne A, Hobeika E, Gouya H, et al. Prediction of drainage effectiveness during endoscopic stenting of malignant hilar strictures: the role of liver volume assessment. Gastrointest Endosc 2010; 72: 728-35.
40. van Gulik TM, Ruys AT, Busch OR, Rauws EA, Gouma DJ. Extent of liver resection for hilar cholangiocarcinoma (klatskin tumor): how much is enough? Dig Surg 2011; 28: 141-7.
41. Tsao JI, Nimura Y, Kamiya J, et al. Management of hilar cholangiocarcinoma: comparison of an American and a Japanese experience. Ann Surg 2000; 232: 166-74.
42. Ruys AT, Busch OR, Gouma DJ, van Gulik TM. Staging Laparoscopy for Hilar Cholangiocarcinoma: Is it Still Worthwhile? Ann Surg Oncol 2011.
43. Li H, Qin Y, Cui Y, Chen H, Hao X, Li Q. Analysis of the Surgical Outcome and Prognostic Factors for Hilar Cholangiocarcinoma: A Chinese Experience. Dig Surg 2011; 28: 226-31.
44. Guglielmi A, Ruzzenente A, Campagnaro T, et al. Prognostic significance of lymph node ratio after resection of peri-hilar cholangiocarcinoma. HPB (Oxford) 2011; 13: 240-5.
45. Benson AB, 3rd, Abrams TA, Ben-Josef E, et al. NCCN clinical practice guidelines in oncology: hepatobiliary cancers. J Natl Compr Canc Netw 2009; 7: 350-91.
46. Eckel F, Jelic S. Biliary cancer: ESMO clinical recommendation for diagnosis, treatment and follow-up. Ann Oncol 2009;20 Suppl 4:46-8.
47. Robles R, Marin C, Pastor P, et al. Liver transplantation for Klatskins tumor: contraindicated, palliative, or indicated? Transplant Proc 2007; 39: 2293-4.
48. Kaiser GM, Sotiropoulos GC, Sgourakis G, et al. Surgical treatment of Klatskin tumor: liver resection versus transplantation. Hepatogastroenterology 2010; 57: 1337-40.
49. Rosen CB, Heimbach JK, Gores GJ. Surgery for cholangiocarcinoma: the role of liver transplantation. HPB (Oxford) 2008; 10: 186-9.
50. Gu J, Bai J, Shi X, et al. Efficacy and safety of liver transplantation for patients with cholangiocarcinoma: A systematic review and meta-analysis. Int J Cancer 2011.
1. Welzel TM, McGlynn KA, Hsing AW, OBrien TR, Pfeiffer RM. Impact of classification of hilar cholangiocarcinomas (Klatskin tumors) on the incidence of intra- and extrahepatic cholangiocarcinoma in the United States. Journal of the National Cancer Institute 2006; 98: 873-5. [ Links ]
2. Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD. Cholangiocarcinoma. Lancet 2005; 366: 1303-14. [ Links ]
3. Klatskin G. Adenocarcinoma of the Hepatic Duct at Its Bifurcation within the Porta Hepatis. An Unusual Tumor with Distinctive Clinical and Pathological Features. The American journal of medicine 1965; 38: 241-56. [ Links ]
4. Bismuth H, Corlette MB. Intrahepatic cholangioenteric anastomosis in carcinoma of the hilus of the liver. Surg Gynecol Obstet 1975; 140: 170-8. [ Links ]
5. Edge SB, Byrd DR, Compton CC. Cancer Staging Manual AJCC (American Joint Committee on Cancer) 7ed. New York: Springer; 2010. [ Links ]
6. Farges O, Fuks D, Le Treut YP, et al. AJCC 7th edition of TNM staging accurately discriminates outcomes of patients with resectable intrahepatic cholangiocarcinoma: By the AFC-IHCC-2009 study group. Cancer 2011; 117: 2170-7. [ Links ]
7. Tyson GL, El-Serag HB. Risk factors of cholangiocarcinoma. Hepatology 2011. [ Links ]
8. Rea DJ, Heimbach JK, Rosen CB, et al. Liver transplantation with neoadjuvant chemoradiation is more effective than resection for hilar cholangiocarcinoma. Ann Surg 2005; 242: 451-8; discussion 8-61. [ Links ]
9. De Martel C, Plummer M, Franceschi S. Cholangiocarcinoma: descriptive epidemiology and risk factors. Gastroenterol Clin Biol 2010; 34: 173-80. [ Links ]
10. Patel T. Cholangiocarcinoma-controversies and challenges. Nature reviews Gastroenterology & hepatology 2011; 8: 189-200. [ Links ]
11. Shaib YH, El-Serag HB, Nooka AK, et al. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: a hospital-based case-control study. Am J Gastroenterol 2007; 102: 1016-21. [ Links ]
12. Mecklin JP, Jarvinen HJ, Virolainen M. The association between cholangiocarcinoma and hereditary nonpolyposis colorectal carcinoma. Cancer 1992; 69: 1112-4. [ Links ]
13. Lee SS, Kim MH, Lee SK, et al. Clinicopathologic review of 58 patients with biliary papillomatosis. Cancer 2004; 100: 783-93. [ Links ]
14. Kobayashi M, Ikeda K, Saitoh S, et al. Incidence of primary cholangiocellular carcinoma of the liver in japanese patients with hepatitis C virus-related cirrhosis. Cancer 2000; 88: 2471-7. [ Links ]
15. El-Serag HB, Engels EA, Landgren O, et al. Risk of hepatobiliary and pancreatic cancers after hepatitis C virus infection: A population-based study of U.S. veterans. Hepatology 2009; 49: 116-23. [ Links ]
16. Sorensen HT, Friis S, Olsen JH, et al. Risk of liver and other types of cancer in patients with cirrhosis: a nationwide cohort study in Denmark. Hepatology 1998; 28: 921-5. [ Links ]
17. Shaib YH, El-Serag HB, Davila JA, Morgan R, McGlynn KA. Risk factors of intrahepatic cholangiocarcinoma in the United States: a case-control study. Gastroenterology 2005; 128: 620-6. [ Links ]
18. Siqueira E, Schoen RE, Silverman W, et al. Detecting cholangiocarcinoma in patients with primary sclerosing cholangitis. Gastrointest Endosc 2002; 56: 40-7. [ Links ]
19. Friman S. Cholangiocarcinoma--current treatment options. Scand J Surg 2011; 100: 30-4. [ Links ]
20. Hann LE, Getrajdman GI, Brown KT, et al. Hepatic lobar atrophy: association with ipsilateral portal vein obstruction. AJR Am J Roentgenol 1996; 167: 1017-21. [ Links ]
21. Feydy A, Vilgrain V, Denys A, et al. Helical CT assessment in hilar cholangiocarcinoma: correlation with surgical and pathologic findings. AJR Am J Roentgenol 1999; 172: 73-7. [ Links ]
22. Hang Y, Uchida M, Abe T, Nishimura H, Hayabuchi N, Nakashima Y. Intrahepatic peripheral cholangiocarcinoma: comparison of dynamic CT and dynamic MRI. J Comput Assist Tomogr 1999; 23: 670-7. [ Links ]
23. Yeh TS, Jan YY, Tseng JH, et al. Malignant perihilar biliary obstruction: magnetic resonance cholangiopancreatographic findings. Am J Gastroenterol 2000; 95: 432-40. [ Links ]
24. Ruiz MH, Castaño R, Alvarez O, et al. Evaluación de la citología por cepillado en las estenosis biliares y pancreáticas durante la colangiografía endoscópica retrógrada. Revista Col de Gastroenterol 2002; 17: 222-5. [ Links ]
25. Coelho-Prabhu N, Baron TH. Endoscopic retrograde cholangiopancreatography in the diagnosis and management of cholangiocarcinoma. Clin Liver Dis 2010; 14: 333-48. [ Links ]
26. Sugiyama M, Hagi H, Atomi Y, Saito M. Diagnosis of portal venous invasion by pancreatobiliary carcinoma: value of endoscopic ultrasonography. Abdom Imaging 1997; 22: 434-8. [ Links ]
27. Lee SW, Kim HJ, Park JH, et al. Clinical usefulness of 18F-FDG PET-CT for patients with gallbladder cancer and cholangiocarcinoma. J Gastroenterol 2010; 45: 560-6. [ Links ]
28. Breitenstein S, Apestegui C, Clavien PA. Positron emission tomography (PET) for cholangiocarcinoma. HPB (Oxford) 2008; 10: 120-1. [ Links ]
29. Laurent A, Tayar C, Cherqui D. Cholangiocarcinoma: preoperative biliary drainage (Con). HPB (Oxford) 2008; 10: 126-9. [ Links ]
30. Nimura Y. Preoperative biliary drainage before resection for cholangiocarcinoma (Pro). HPB (Oxford) 2008; 10: 130-3. [ Links ]
31. Su CH, Tsay SH, Wu CC, et al. Factors influencing postoperative morbidity, mortality, and survival after resection for hilar cholangiocarcinoma. Ann Surg 1996; 223: 384-94. [ Links ]
32. Rocha FG, Matsuo K, Blumgart LH, Jarnagin WR. Hilar cholangiocarcinoma: the Memorial Sloan-Kettering Cancer Center experience. J Hepatobiliary Pancreat Sci 2010; 17: 490-6. [ Links ]
33. Cherqui D, Benoist S, Malassagne B, Humeres R, Rodriguez V, Fagniez PL. Major liver resection for carcinoma in jaundiced patients without preoperative biliary drainage. Arch Surg 2000; 135: 302-8. [ Links ]
34. Costamagna G, Mutignani M, Perri V, et al. Results of endoscopic biliary drainage in primary tumors of the common bile duct (cholangiocarcinoma). Chir Ital 1995; 47: 18-23. [ Links ]
35. Castaño R, Ricardo A, Velásquez L, Ruiz MH, Ruiz LM. Desempeño del stent plástico para la paliación en la obstrucción biliar maligna proximal versus distal. Rev Col Gastroenterol 2011; en prensa. [ Links ]
36. Perdue DG, Freeman ML, DiSario JA, et al. Plastic versus self-expanding metallic stents for malignant hilar biliary obstruction: a prospective multicenter observational cohort study. J Clin Gastroenterol 2008; 42: 1040-6. [ Links ]
37. Raju RP, Jaganmohan SR, Ross WA, et al. Optimum palliation of inoperable hilar cholangiocarcinoma: comparative assessment of the efficacy of plastic and self-expanding metal stents. Dig Dis Sci 2011; 56: 1557-64. [ Links ]
38. De Palma GD, Galloro G, Siciliano S, Iovino P, Catanzano C. Unilateral versus bilateral endoscopic hepatic duct drainage in patients with malignant hilar biliary obstruction: results of a prospective, randomized, and controlled study. Gastrointest Endosc 2001; 53: 547-53. [ Links ]
39. Vienne A, Hobeika E, Gouya H, et al. Prediction of drainage effectiveness during endoscopic stenting of malignant hilar strictures: the role of liver volume assessment. Gastrointest Endosc 2010; 72: 728-35. [ Links ]
40. van Gulik TM, Ruys AT, Busch OR, Rauws EA, Gouma DJ. Extent of liver resection for hilar cholangiocarcinoma (klatskin tumor): how much is enough? Dig Surg 2011; 28: 141-7. [ Links ]
41. Tsao JI, Nimura Y, Kamiya J, et al. Management of hilar cholangiocarcinoma: comparison of an American and a Japanese experience. Ann Surg 2000; 232: 166-74. [ Links ]
42. Ruys AT, Busch OR, Gouma DJ, van Gulik TM. Staging Laparoscopy for Hilar Cholangiocarcinoma: Is it Still Worthwhile? Ann Surg Oncol 2011. [ Links ]
43. Li H, Qin Y, Cui Y, Chen H, Hao X, Li Q. Analysis of the Surgical Outcome and Prognostic Factors for Hilar Cholangiocarcinoma: A Chinese Experience. Dig Surg 2011; 28: 226-31. [ Links ]
44. Guglielmi A, Ruzzenente A, Campagnaro T, et al. Prognostic significance of lymph node ratio after resection of peri-hilar cholangiocarcinoma. HPB (Oxford) 2011; 13: 240-5. [ Links ]
45. Benson AB, 3rd, Abrams TA, Ben-Josef E, et al. NCCN clinical practice guidelines in oncology: hepatobiliary cancers. J Natl Compr Canc Netw 2009; 7: 350-91. [ Links ]
46. Eckel F, Jelic S. Biliary cancer: ESMO clinical recommendation for diagnosis, treatment and follow-up. Ann Oncol 2009;20 Suppl 4:46-8. [ Links ]
47. Robles R, Marin C, Pastor P, et al. Liver transplantation for Klatskins tumor: contraindicated, palliative, or indicated? Transplant Proc 2007; 39: 2293-4. [ Links ]
48. Kaiser GM, Sotiropoulos GC, Sgourakis G, et al. Surgical treatment of Klatskin tumor: liver resection versus transplantation. Hepatogastroenterology 2010; 57: 1337-40. [ Links ]
49. Rosen CB, Heimbach JK, Gores GJ. Surgery for cholangiocarcinoma: the role of liver transplantation. HPB (Oxford) 2008; 10: 186-9. [ Links ]
50. Gu J, Bai J, Shi X, et al. Efficacy and safety of liver transplantation for patients with cholangiocarcinoma: A systematic review and meta-analysis. Int J Cancer 2011. [ Links ]

