










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.2 Bogotá abr./jun. 2011
Laparoscopic-assisted percutaneous endoscopic gastrostomy: case report
Raúl Eduardo Pinilla Morales, MD (1), Juan David Hernández Restrepo, MD (2)
(1) General Practitioner at El Bosque University, 1999. General surgeon at University Hospital La Samaritana Pontificia Universidad Javeriana. 2003. Fellowship in Gastroenterology and Digestive Endoscopy at San Jose Hospital, Fundación Universitaria de Ciencias de la Salud. Hospital Central de la Policía Nacional, Bogotá, Colombia.
(2) General Surgeon at University Hospital La Samaritana, Pontificia Universidad Javeriana. Chief of General Surgery Department at Hospital Central de la Policía Nacional, Associate professor at Los Andes University. Bogotá, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 22-11-10 Accepted: 06-04-11
Abstract
Percutaneous endoscopic gastrostomy (PEG) is the choice technique to establish a feeding route for patients that requiring special nutritional support for more than 4 weeks; however, to be an intervention performed percutaneously, the inability to demonstrate transillumination of the abdominal wall and the failure to obtain convexity with the finger-pressure are usually considered contraindications for its realization.
This report is about a case in which spite of a major contraindication for PEG, it was performed under laparoscopic guidance, thus providing a minimally invasive alternative, avoiding the realization of an open surgical procedure.
Keywords
PEG, percutaneous endoscopic gastrostomy, laparoscopy
INTRODUCTION
Since its introduction in 1980, percutaneous endoscopic gastrostomy (PEG) has become the procedure of choice for establishing a feeding route for patients who require more than 30 days of special nutrition (1-3). The procedure is performed successfully in 95% of the cases (4).
Nevertheless, certain characteristics of a patient can absolutely contraindicate this procedures performance. When it is impossible to move the anterior gastric wall until it makes contact with the abdominal wall, transillumination of the stomach is impeded for different reasons. These include obesity, severe scoliosis, peritoneal adhesions secondary to surgery, prior gastric resection, ascites and hepatomegaly (5, 6). Complications from this procedure are not infrequent and have been classified by Schapiro as major and minor complications (7). An example of a minor complication is a leak through a stoma which is present in up to 78% of these cases (8). Major complications appear in 3% of cases (9, 10). They include aspiration, peritonitis, hemorrhaging, catheter migration, gastrointestinal cutaneous fistulas, and serious infections of lesions with necrotizing fasciitis. They also include rarer rare ones such as tumor seeding in stoma of patients with oropharyngeal neoplasias, aortic-gastric fistulas, intrahepatic catheter placement, gastric volvulus, subcutaneous emphysema and persistent pneumoperitoneum (11).
Even though there have been reports of laparoscopic-assisted PEG (12-16), various management guides do not contemplate this procedure as an alternative when there is no safe access to the gastric cavity. According to these guides, this procedure is contraindicated under these circumstances resulting in a recommendation of open surgical gastrostomies for these cases (1, 5, 17,18).
CASE PRESENTATION
The subject was a 23 year old male patient who had suffered multiple episodes of pneumonia. Patient records indicated they had been caused by bronchial aspiration due to neurological aftereffects of neonatal hypoxia. Nissen gastroesophageal antireflux surgery had been performed during his childhood. Physical examination showed a considerable xiphoid-umbilical scar (Figure 1).
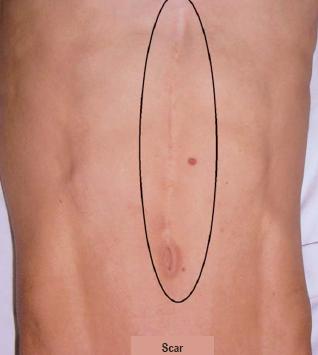
Figure 1. Xiphoid-umbilical scar.
Given the neurological condition of the patient, esophagogastroduodenoscopy was performed under general anesthesia. Finding no suitable site for safe trans-abdominal ultrasound-guided puncture, we decided to perform an infraumbilical incision by introducing 10mm trocar using the open technique. Next, the patient was insufflated with carbon dioxide to allow performance of a laparoscopy. This allowed us to detect that the left hepatic lobe had adhered to the abdominal wall and that there were other omental parietal adhesions that explained the difficulty of locating a safe puncture zone (Figure 2).
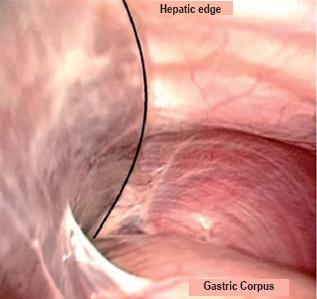
Figure 2. Laparoscopic view showing hepatic edge adhering to front abdominal wall.
Under laparoscopic vision, we continued to proceed with another endoscopic approach to perform the PEG using the "pull" technique. We were able to see the puncture site in the abdominal wall without jeopardizing the liver of the patient which had been previously observed (Figure 3 and 4). The patient´s immediate postoperative evolution was optimal, and the patients condition remained optimal during two monthly follow-up check-ups after discharge.
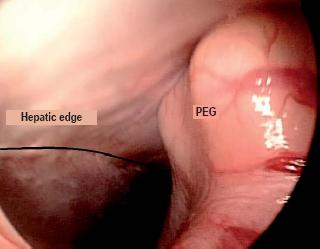
Figure 3. Laparoscopic view showing final location of gastrostomy.
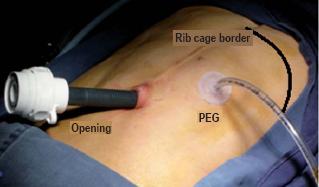
Figure 4. External view showing final location of gastrostomy.
DISCUSSION
Percutaneous endoscopic gastrostomy, despite being the procedure of choice for patients who require prolonged special nutrition, still presents morbidity rates which are far from negligible. Although the superiority of this procedure over the laparoscopic and open techniques is evident (3), certain groups of patients with anatomical alterations may be at high risk from this procedure (7).
In 1998, in response to the impossibility of providing illumination adequate for identifying a gastric puncture site, Stewart described a technique which consists of using a syringe with 10cc of saline solution to puncture and continually aspirate in a manner that prevents the entrance of air prior to the needle reaching the gastric cavity. This method allowed the puncture to be completed safely in a way that avoided puncturing any other organ prior to reaching the stomach, thus demonstrating that the absence of illumination should no longer be considered an absolute contraindication to performance of a PEG (19). Nevertheless, no controlled studies were ever conducted concerning this method. Moreover, since it is not infallible patients continue to be referred for conventional surgery.
The availability of different technical resources for treat organs within the abdomen, in this case a hybrid gastroscopic-assisted laparoscopic procedure, provides an advantage to patients, who do not have to be submitted to open surgical procedures with their high morbidity rates, extensive incisions in the abdominal wall, and resulting adhesions. Consequently, endoscopic-assisted intervention which once entailed the risks mentioned earlier in this article, is becoming a safer procedure, free of complications derived from a blind approach and with minimal invasive surgery.
Acknowledgements
Thanks to Dr. Héctor José Cardona Villamizar, Chief of Gastroenterology at the Central Hospital of the National Police for his presence and logistical support.
REFERENCES
1. American Gastroenterological Association Medical Position Statement: guidelines for the use of enteral nutrition. Gastroenterology 1995; 108(4): 1280-1.
2. Gauderer MW, Ponsky JL, Izant RJ, Jr. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg 1980; 15(6): 872-5.
3. Bankhead RR, Fisher CA, Rolandelli RH. Gastrostomy tube placement outcomes: comparison of surgical, endoscopic, and laparoscopic methods. Nutr Clin Pract 2005; 20(6): 607-12.
4. Larson DE, Burton DD, Schroeder KW, DiMagno EP. Percutaneous endoscopic gastrostomy. Indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology 1987; 93(1): 48-52.
5. Eisen GM, Baron TH, Dominitz JA, Faigel DO, Goldstein JL, Johanson JF, et al. Role of endoscopy in enteral feeding. Gastrointest Endosc 2002; 55(7): 794-7.
6. Gauderer MW. Experience with a hybrid, minimally invasive gastrostomy for children with abnormal epigastric anatomy. J Pediatr Surg 2008; 43(12): 2178-81.
7. Schapiro GD, Edmundowicz SA. Complications of percutaneous endoscopic gastrostomy. Gastrointest Endosc Clin N Am 1996; 6(2): 409-22.
8. Rogers SN, Thomson R, OToole P, Lowe D. Patients experience with long-term percutaneous endoscopic gastrostomy feeding following primary surgery for oral and oropharyngeal cancer. Oral Oncol 2007; 43(5): 499-507.
9. Lin HS, Ibrahim HZ, Kheng JW, Fee WE, Terris DJ. Percutaneous endoscopic gastrostomy: strategies for prevention and management of complications. Laryngoscope 2001; 111(10): 1847-52.
10. DiSario JA. Endoscopic approaches to enteral nutritional support. Best Pract Res Clin Gastroenterol 2006; 20(3): 605-30.
11. Potack JZ, Chokhavatia S. Complications of and controversies associated with percutaneous endoscopic gastrostomy: report of a case and literature review. Medscape J Med 2008; 10(6): 142.
12. Kohler H, Razeghi S, Spychalski N, Behrens R, Carbon R. Laparoscopic-assisted percutaneous endoscopic gastrostomy--rendez-vous PEG--in infants, children and adolescents. Endoscopy 2007; 39 Suppl 1: E136.
13. Hii MW, Fox AM, Cade RJ. Laparoscopy-assisted percutaneous-endoscopic gastrostomy tube insertion. ANZ J Surg 2008; 78(11): 1047.
14. Charlesworth P, Hallows M, van der Avoirt A. Single-center experience of laparoscopically assisted percutaneous endoscopic gastrostomy placement. J Laparoendosc Adv Surg Tech A 2010; 20(1): 73-5.
15. Lopes G, Salcone M, Neff M. Laparoscopic-assisted percutaneous endoscopic gastrostomy tube placement. JSLS 2010; 14(1): 66-9.
16. Denzer U, Mergener K, Kanzler S, Kiesslich R, Helmreich-Becker I, Galle PR, et al. Mini-laparoscopically guided percutaneous gastrostomy and jejunostomy. Gastrointest Endosc 2003; 58(3): 434-8.
17. Loser C, Aschl G, Hebuterne X, Mathus-Vliegen EM, Muscaritoli M, Niv Y, et al. ESPEN guidelines on artificial enteral nutrition--percutaneous endoscopic gastrostomy (PEG). Clin Nutr 2005; 24(5): 848-61.
18. Greff M. Guidelines of the French Society of Digestive Endoscopy (SFED): endoscopic gastrostomy. Endoscopy 1999; 31(2): 207-8.
19. Stewart JA, Hagan P. Failure to transilluminate the stomach is not an absolute contraindication to PEG insertion. Endoscopy 1998; 30(7): 621-2.
1. American Gastroenterological Association Medical Position Statement: guidelines for the use of enteral nutrition. Gastroenterology 1995; 108(4): 1280-1. [ Links ]
2. Gauderer MW, Ponsky JL, Izant RJ, Jr. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg 1980; 15(6): 872-5. [ Links ]
3. Bankhead RR, Fisher CA, Rolandelli RH. Gastrostomy tube placement outcomes: comparison of surgical, endoscopic, and laparoscopic methods. Nutr Clin Pract 2005; 20(6): 607-12. [ Links ]
4. Larson DE, Burton DD, Schroeder KW, DiMagno EP. Percutaneous endoscopic gastrostomy. Indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology 1987; 93(1): 48-52. [ Links ]
5. Eisen GM, Baron TH, Dominitz JA, Faigel DO, Goldstein JL, Johanson JF, et al. Role of endoscopy in enteral feeding. Gastrointest Endosc 2002; 55(7): 794-7. [ Links ]
6. Gauderer MW. Experience with a hybrid, minimally invasive gastrostomy for children with abnormal epigastric anatomy. J Pediatr Surg 2008; 43(12): 2178-81. [ Links ]
7. Schapiro GD, Edmundowicz SA. Complications of percutaneous endoscopic gastrostomy. Gastrointest Endosc Clin N Am 1996; 6(2): 409-22. [ Links ]
8. Rogers SN, Thomson R, OToole P, Lowe D. Patients experience with long-term percutaneous endoscopic gastrostomy feeding following primary surgery for oral and oropharyngeal cancer. Oral Oncol 2007; 43(5): 499-507. [ Links ]
9. Lin HS, Ibrahim HZ, Kheng JW, Fee WE, Terris DJ. Percutaneous endoscopic gastrostomy: strategies for prevention and management of complications. Laryngoscope 2001; 111(10): 1847-52. [ Links ]
10. DiSario JA. Endoscopic approaches to enteral nutritional support. Best Pract Res Clin Gastroenterol 2006; 20(3): 605-30. [ Links ]
11. Potack JZ, Chokhavatia S. Complications of and controversies associated with percutaneous endoscopic gastrostomy: report of a case and literature review. Medscape J Med 2008; 10(6): 142. [ Links ]
12. Kohler H, Razeghi S, Spychalski N, Behrens R, Carbon R. Laparoscopic-assisted percutaneous endoscopic gastrostomy--rendez-vous PEG--in infants, children and adolescents. Endoscopy 2007; 39 Suppl 1: E136. [ Links ]
13. Hii MW, Fox AM, Cade RJ. Laparoscopy-assisted percutaneous-endoscopic gastrostomy tube insertion. ANZ J Surg 2008; 78(11): 1047. [ Links ]
14. Charlesworth P, Hallows M, van der Avoirt A. Single-center experience of laparoscopically assisted percutaneous endoscopic gastrostomy placement. J Laparoendosc Adv Surg Tech A 2010; 20(1): 73-5. [ Links ]
15. Lopes G, Salcone M, Neff M. Laparoscopic-assisted percutaneous endoscopic gastrostomy tube placement. JSLS 2010; 14(1): 66-9. [ Links ]
16. Denzer U, Mergener K, Kanzler S, Kiesslich R, Helmreich-Becker I, Galle PR, et al. Mini-laparoscopically guided percutaneous gastrostomy and jejunostomy. Gastrointest Endosc 2003; 58(3): 434-8. [ Links ]
17. Loser C, Aschl G, Hebuterne X, Mathus-Vliegen EM, Muscaritoli M, Niv Y, et al. ESPEN guidelines on artificial enteral nutrition--percutaneous endoscopic gastrostomy (PEG). Clin Nutr 2005; 24(5): 848-61. [ Links ]
18. Greff M. Guidelines of the French Society of Digestive Endoscopy (SFED): endoscopic gastrostomy. Endoscopy 1999; 31(2): 207-8. [ Links ]
19. Stewart JA, Hagan P. Failure to transilluminate the stomach is not an absolute contraindication to PEG insertion. Endoscopy 1998; 30(7): 621-2. [ Links ]

