










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.2 Bogotá abr./jun. 2011
A pancreatic intraductal papillary mucinous neoplasm: A case report and literature review
Martín A. Gómez Z., MD (1), Cristian Melgar, MD (2), Germán Junca, MD (3)
(1) Gastroenterology Professor, Faculty of Medicine, Universidad Nacional de Colombia. Gastroenterologist, Hospital Tunal. Bogotá, Colombia.
(2) Gastroenterology Resident. Universidad Nacional de Colombia. Bogotá, Colombia.
(3) Gastrointestinal Surgeon INC. Assistant Professor of Surgery. Universidad Nacional de Colombia. Bogotá, Colombia.
Translated by T.A. Zuur and The Language Workshop
Received: 12-08-10 Accepted: 06-06-11
Abstract
Intraductal papillary mucinous neoplasms (IPMNs) are rare pancreatic tumors that are diagnosed more and more frequently as imaging for evaluation of the pancreas becomes more widespread. Patients with these tumors may arrive at an emergency room with acute abdominal pain that often becomes chronic, accompanied by repeated episodes of pancreatitis. In this paper we describe the case a patient with IPMN which was a cause of acute pancreatitis. This patient came to the emergency room for severe abdominal pain.
Key words
Intraductal papillary mucinous neoplasms (IPMNs), pancreatic tumors, acute abdominal pain, pancreatitis.
Intraductal papillary mucinous neoplasms (IPMNs) are rare pancreatic tumors that are diagnosed more and more frequently as imaging for evaluation of the pancreas becomes more widespread (1). Patients with these tumors may arrive at an emergency room with acute abdominal pain that often becomes chronic and may be accompanied by repeated episodes of pancreatitis (2).
In this paper we describe the case of a patient with IPMN which was a cause of acute pancreatitis. This patient came to the emergency room for severe abdominal pain.
CASE REPORT
A 51 year old male patient was admitted to the emergency room after suffering abdominal pain for 7 days. The pain was located in the epigastrium and radiated to lumbar region of the back. The patient was referred because of nausea and severe vomiting. During the patient interview patient said he did not use alcohol, drugs or tobacco. The physical examination showed signs of dehydration, tachycardia and abdominal pain upon palpitation, but no peritoneal irritation.
Patient was rehydrated in the emergency department and paraclinical tests were performed. Blood count, liver function tests (ALT, AST, total bilirubin, direct bilirubin) and triglycerides were normal, patients amylase level was 1100 mg/dl, and a total abdominal ultrasound was also normal. Based on the clinical presentation, physical examination findings and paraclinical tests, idiopathic acute pancreatitis was diagnosed.
Biliopancreatic endoscopic ultrasonography was chosen to study the etiology of acute pancreatitis. A 3 mm lesion was found in the uncinate process within the dilated pancreatic duct. The pancreatic parenchyma evidenced increased echogenicity without focal abnormalities, dilation of the duct of Wirsung measuring 5mm extended throughout the pancreatic head. After diagnostic imaging a pancreatic intraductal papillary mucinous neoplasm (IPMN) along with secondary acute pancreatitis was diagnosed (Figure 1).

Figure 1. The lower left quadrant shows the lesion. Notice that the common bile duct is normal, but the duct of Wirsung is dilated and has a small solid lesion within it.
Magnetic resonance imaging revealed a dilated pancreatic duct with a pancreatic head lesion, but no bile duct lesions (Figure 2).
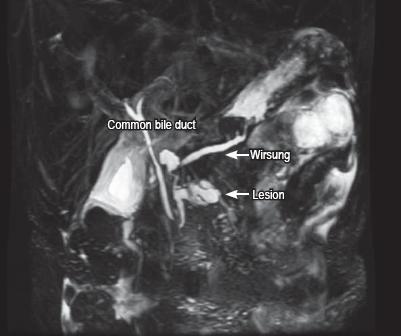
Figure 2. Magnetic resonance imaging revealed a lesion and dilatation of the primary pancreatic duct.
Once the patient had recovered from a mild case of acute pancreatitis it was decided to perform a Whipple procedure (pancreatoduodenectomy) (Figure 3).
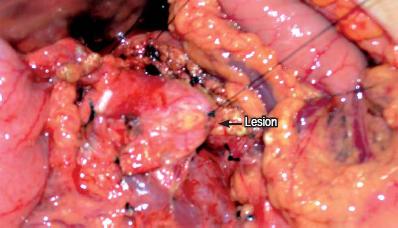
Figure 3. Surgical resection of lesion
The piece removed was sent to pathology which reported an IPMN with carcinoma in situ that involved the head of the pancreas. The tumor was 2.5 cm x 2 cm x 2 cm without infiltrating compromise or lymphovascular or peri-neural invasion. The margins of the section tumor-free, and the lymph nodes were negative for malignancy (Figure 4).

Figure 4. Pathology revealed a lesion and a dilated pancreatic duct.
The patient evolved successfully, was released from the hospital, and is now considered to be cured of the disease.
LITERATURE REVIEW
In 1996 Ohhashi et al. (1) described intraductal papillary mucinous neoplasms of the pancreas (IPMN) for the first time. They called them "mucus-secreting pancreatic cancer." Unlike other mucinous cystic neoplasms of the pancreas, IPMNs are produce lesions which directly communicate with the duct of Wursing and have no ovarian type stroma (2). IPMNs are also characterized by the presence of segmental dilatation in the primary pancreatic duct and/or in secondary branches. These are coated with a mucin-producing dysplastic villous epithelium (3). Cysts form in the compromised ducts.
The natural histories of these tumors differ from ductal adenocarcinomas since 90% to 100% of these cases are resectable. The survival rate ranges between 80% and 90% when a carcinoma in situ is resected, falls to 50% to 70% for invasive carcinomas, and falls further to 40% to 50 % when the carcinoma has already metastasized to the lymph nodes (4).
These lesions typically occur in men between 60 and 80 years of age and occur most frequently in the pancreatic head (5) (as occurred in our patient). Nevertheless, in 30% of cases they widely affect the entire gland (6).
Two forms of IPMNs have been proposed: primary duct and secondary branch IPMNs. When the tumor affects the secondary branches, differentiation can be difficult especially for mucinous cystic neoplasms. For this reason, histological, imaging and other diagnostic tools should be used to differentiate among the various types of pancreatic cystic tumors of inflammatory origin before any invasive management procedures are performed. Ninety percent of pancreatic cystic lesions are inflammatory pseudocysts, while the remaining ten percent are non-inflammatory lesions (7).
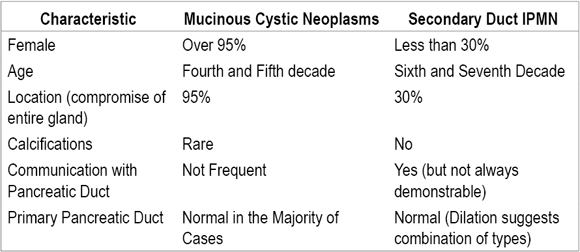
Table 1 describes the basic features of tumor markers in mucinous fluid of non-inflammatory cystic lesions of the pancreas. And in table 2, the typical characteristics of mucinous cystic neoplasms and secondary branch IPMNs are differentiated.
Table 1. Tumor markers in cyst fluids of non-inflammatory cystic lesions of the pancreas.

Table 2. Typical features of cystic mucinous neoplasms and secondary duct IPMNs.
Because of their indolent and nonspecific clinical characteristics, IPMNs are usually discovered incidentally (8). Sometimes they are found in patients with chronic abdominal pain or recurrent episodes of acute pancreatitis that could be related to intermittent obstruction of the pancreatic duct by mucinous conglomerates (9, 10, 21).
Thirty percent of the invasive tumors are found in asymptomatic patients (13). The general features of these malignant lesions include the presence of mural nodules, pancreatic duct diameters greater than 15 mm and lesion sizes greater than 3 cm (12).
Characteristics of images that should lead the physician to suspect IPMN include segmentation of the pancreatic duct, dilatation of secondary branch ducts and communication of the tumor with the primary pancreatic duct (11).
The most important elements for classification of IPMNs are the differences in the degree of compromise of the primary pancreatic duct and of the secondary branches (14). This determination is based on images or histological findings. Duct dilatation of more than one centimeter suggests a principal duct IPMN, while the presence of a pancreatic mucinous cyst communicating with the pancreatic duct without dilatation of the duct suggests a secondary duct IPMN. However, the primary distinction between these two conditions is determined with the histological specimen (13).
This difference is of vital importance for the prevalences of these two types of cancerous lesions. According to the results of more than one series, primary duct IPMNs (The case discussed herein was a primary duct IPMN.) have a prevalence ranging between 57% and 92% while the prevalence of secondary duct IPMNs is between 6% and 46% (14, 15).
The definitive prognosis of an IPMN occurs once it is reclassified after resection into one of three categories: adenomas, borderline tumors and neoplasias. Adenomas have atypical histological features and are low grade or benign. Borderline tumors are moderately atypical, and neoplasias are severely atypical and may show evidence of invasion (13, 14).
When a primary duct IPMN is identified in a patient with a long life expectancy who has no contraindications, the current recommendation is surgical management (used to treat our patient) (13-18). This is supported by the high prevalence of malignancy in these tumors, ranging up to 70%, and the risk of invasion of other organs (15-17).
Clear characteristics have been described in patients with secondary duct IPMNs that support immediate nonsurgical management for lesions smaller than 3 cm and for asymptomatic patients. These groups have lower prevalences of malignancies, but for symptomatic patients with lesions larger than 3 cm, surgical management is recommended. The approach flow chart for pancreatic cystic lesions shows current management of these patients (figure 5) (13, 19, 20, 22).
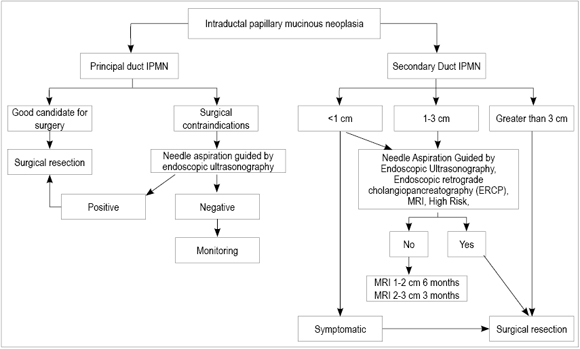
Figure 5. Flow chart of approaches to intraductal papillary mucinous neoplasias. Modified from (11, 13).
CONCLUSIONS
In the case presented in this article, the patient apparently had idiopathic acute pancreatitis, but during the diagnostic evaluation the patient evidenced an IPMN. 20% to 30% of pancreatitis cases are classified as idiopathic because of biliary etiology, alcohol, drugs and hypertriglyceridemia. However, other causes are usually not evaluated. Therefore, our group believes that all patients with acute pancreatitis should undergo a biliopancreatic endoscopy as this not only allows assessment with certainty of biliary etiology, but also rules out a structural lesion of the pancreas (as in this case).
REFERENCES
1. Kloppel G, Solcia E, Capella C. Histological typing of tumors of the exocrine pancreas. Springer, Berlin 1996.
2. Baiocchi G, Portolani N, Missale G. Intraductal papillary mucinous of the pancreas (IPMN): clinicopathological correlations and surgical indications. World journal of surgical oncology 2010; 8: 2-7.
3. Scheiman JM. Cystic lesion of the pancreas. Gastroenterology 2005; 128: 463- 9.
4. Salvia R, Fernández del Castillo C. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg 2004; 239: 678-85.
5. Fernández del Castillo C, Targarona J, Thayer SP. Incidental pancreatic cysts: clinicopathologic characteristics and comparison with symptomatic patients. Arch Surg 2003; 138: 427-433.
6. Zamboni G, Scarpa A, Bogina G. Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Am J Surg Pathol. 1999; 23: 410- 22.
7. William R. Brugge, Gregory Y. Cystic Neoplasms of the Pancreas. N Engl J Med 2004; 351: 1218-26.
8. Procacci C, Carbognin G, Accordini S, Biasiutti C, Guarise A, Lombardo F, Ghirardi C, Graziani R, Pagnotta N, De Marco R. CT features of malignant mucinous cystic tumors of the pancreas. Eur Radiol 2001; 11: 1626-1630.
9. Fernández del Castillo C, Taragona J. Incidental Pancreatic cystic: Clinicopathologic characteristics and comparasion with symptomatic patients. Arch Surg 2003; 138: 427-30.
10. Sugiyama M, Izumisato Y, Abe N. Predictive factors for malignancy in intraductal papillary mucinous tumours of the pancreas. Br J Surg 2003; 90: 1244- 9.
11. Vargas Lorenzo MJ. Ultrasonografía endoscópica. Aplicaciones diagnósticas y terapéuticas. Cap. 12, 1 edición. Editorial Médica Panamericana. 2008 p. 141-168.
12. Edward V, Loftus Jr., Olivares P. Intraductal Papillary-Mucinous tumors of the Pancreas: Clinicopathologic Features, Outcome and Nomenclature, Gastroenterology 1996; 110: 1909-1918.
13. Masao T, Suresh C, Volkan A. International Consensus Guidelines for management of Intraductal Papillary Mucinous Neoplasms and Mucinous Cystic Neoplasms of the Pancreas. Pancreatology 2006; 6: 17-32.
14. Terris B, Ponsot P, Paye F, Hammel P. Intraductal papillary mucinous tumors of the pancreas confi ned to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol 2000; 24: 1372-1377.
15. Doi R, Fujimoto K, Wada M, Imamura M. Surgical management of intraductal papillary mucinous tumor of the pancreas. Surgery 2002; 132: 80-85.
16. Farrell JJ, Brugge WR. Intraductal papillary mucinous tumor of the pancreas. Gastrointest Endosc 2002; 55: 701.
17. Choi BS, Kim TK, Kim AY, Kim KW, Park SW, Kim PN, Ha HK, Lee MG, Kim SC. Differential diagnosis of benign and malignant intraductal papillary mucinous tumors of the pancreas: MR cholangio-pancreatography and MR angiography. Korean J Radiol 2003; 4: 157-162.
18. Sohn TA, Yeo CJ, Cameron JL, Hruban RH, Fukushima N, Campbell KA, Illemoe KD. Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Ann Surg 2004; 239: 788-799.
19. Kobari M, Egawa S, Shibuya K, Shimamura H, Sunamura M, Takeda K, Atsuno S, Furukawa T. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg 1999; 134: 1131-1136.
20. Kimura W. IHPBA in Tokyo, 2002: Surgical treatment of IPMT vs. MCT: a Japanese experience. J Hepatobiliary Pancreat Surg 2003; 10: 156-162.
21. Daniel A Ringold, Puneet Shroff. Pancreatitis is frequent among patients with side-branch intraductal papillary mucinous neoplasia diagnosed by EUS. Gastrointest Endosc 2009; 70: 488-94.
22. McGrath K, Krasinskas A. Intraductal Papillary Mucinous Neoplasia. Gastroenterol Clin N Am 2007; 36: 377-390.
1. Kloppel G, Solcia E, Capella C. Histological typing of tumors of the exocrine pancreas. Springer, Berlin 1996. [ Links ]
2. Baiocchi G, Portolani N, Missale G. Intraductal papillary mucinous of the pancreas (IPMN): clinicopathological correlations and surgical indications. World journal of surgical oncology 2010; 8: 2-7. [ Links ]
3. Scheiman JM. Cystic lesion of the pancreas. Gastroenterology 2005; 128: 463- 9. [ Links ]
4. Salvia R, Fernández del Castillo C. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg 2004; 239: 678-85. [ Links ]
5. Fernández del Castillo C, Targarona J, Thayer SP. Incidental pancreatic cysts: clinicopathologic characteristics and comparison with symptomatic patients. Arch Surg 2003; 138: 427-433. [ Links ]
6. Zamboni G, Scarpa A, Bogina G. Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Am J Surg Pathol. 1999; 23: 410- 22. [ Links ]
7. William R. Brugge, Gregory Y. Cystic Neoplasms of the Pancreas. N Engl J Med 2004; 351: 1218-26. [ Links ]
8. Procacci C, Carbognin G, Accordini S, Biasiutti C, Guarise A, Lombardo F, Ghirardi C, Graziani R, Pagnotta N, De Marco R. CT features of malignant mucinous cystic tumors of the pancreas. Eur Radiol 2001; 11: 1626-1630. [ Links ]
9. Fernández del Castillo C, Taragona J. Incidental Pancreatic cystic: Clinicopathologic characteristics and comparasion with symptomatic patients. Arch Surg 2003; 138: 427-30. [ Links ]
10. Sugiyama M, Izumisato Y, Abe N. Predictive factors for malignancy in intraductal papillary mucinous tumours of the pancreas. Br J Surg 2003; 90: 1244- 9. [ Links ]
11. Vargas Lorenzo MJ. Ultrasonografía endoscópica. Aplicaciones diagnósticas y terapéuticas. Cap. 12, 1 edición. Editorial Médica Panamericana. 2008 p. 141-168. [ Links ]
12. Edward V, Loftus Jr., Olivares P. Intraductal Papillary-Mucinous tumors of the Pancreas: Clinicopathologic Features, Outcome and Nomenclature, Gastroenterology 1996; 110: 1909-1918. [ Links ]
13. Masao T, Suresh C, Volkan A. International Consensus Guidelines for management of Intraductal Papillary Mucinous Neoplasms and Mucinous Cystic Neoplasms of the Pancreas. Pancreatology 2006; 6: 17-32. [ Links ]
14. Terris B, Ponsot P, Paye F, Hammel P. Intraductal papillary mucinous tumors of the pancreas confi ned to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol 2000; 24: 1372-1377. [ Links ]
15. Doi R, Fujimoto K, Wada M, Imamura M. Surgical management of intraductal papillary mucinous tumor of the pancreas. Surgery 2002; 132: 80-85. [ Links ]
16. Farrell JJ, Brugge WR. Intraductal papillary mucinous tumor of the pancreas. Gastrointest Endosc 2002; 55: 701. [ Links ]
17. Choi BS, Kim TK, Kim AY, Kim KW, Park SW, Kim PN, Ha HK, Lee MG, Kim SC. Differential diagnosis of benign and malignant intraductal papillary mucinous tumors of the pancreas: MR cholangio-pancreatography and MR angiography. Korean J Radiol 2003; 4: 157-162. [ Links ]
18. Sohn TA, Yeo CJ, Cameron JL, Hruban RH, Fukushima N, Campbell KA, Illemoe KD. Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Ann Surg 2004; 239: 788-799. [ Links ]
19. Kobari M, Egawa S, Shibuya K, Shimamura H, Sunamura M, Takeda K, Atsuno S, Furukawa T. Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg 1999; 134: 1131-1136. [ Links ]
20. Kimura W. IHPBA in Tokyo, 2002: Surgical treatment of IPMT vs. MCT: a Japanese experience. J Hepatobiliary Pancreat Surg 2003; 10: 156-162. [ Links ]
21. Daniel A Ringold, Puneet Shroff. Pancreatitis is frequent among patients with side-branch intraductal papillary mucinous neoplasia diagnosed by EUS. Gastrointest Endosc 2009; 70: 488-94. [ Links ]
22. McGrath K, Krasinskas A. Intraductal Papillary Mucinous Neoplasia. Gastroenterol Clin N Am 2007; 36: 377-390. [ Links ]

