










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.2 Bogotá Apr./June 2011
Intestinal intussusception due to benign lesions in adults
Charles Elleri Bermúdez, MD (1), Luis Carlos Domínguez, MD (2), Diego Buitrago, MD (1), David Gómez, MD (1)
(1) Department of Surgery Hospital Universitario de San Ignacio. Pontificia Universidad Javeriana. Bogotá, Colombia.
(2) Department of Surgery Hospital Universitario de San Ignacio. Pontificia Universidad Javeriana, Bogotá. Department of Surgery Universidad de la Sabana. Chía, Cundinamarca, Colombia.
Correspondence: cebermudez@husi.org.co, chebermud@yahoo.com
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 14-12-10 Accepted: 06-04-11
Abstract
Intestinal intussusception in adults occurs infrequently. In this study we describe two cases of acute surgical events characterized by abdominal pain, masses and obstructive symptoms. One of these cases occurred in an 18 year old woman with jejuno-jejunal intussusceptions due to a hamartomatous polyp. The other case was a 40 year woman with a colo-colonic intussusception due to a submucosal lipoma in the descending colon.
Key words
Intussusception, adult, intestinal obstruction, hamartomatous polyp, bowel lipoma, surgery.
INTRODUCTION
Intestinal intussusception is infrequent in adults. In the majority of the cases there is an identifiable mechanical cause. It is usually a benign or malignant tumor which conditions a acute abdominal pain more often than chronic or episodic pain. The small intestine is more frequently compromised than the colon or gastroduodenal portion of the intestines. Since this entity occurs infrequently, we decided to report two cases of intussusception which caused intestinal obstructions. One of these cases had a compromised jejunum and the other had a compromised colon. We will simultaneously present the cases and review the literature with emphasis on the most important aspects of this pathology.
CASE 1
An 18 year old female patient entered the emergency service of the University Hospital of San Ignacio in Bogota, Colombia after enduring 24 hours of severe and continuous anterior abdominal pain, multiple episodes of vomiting, fever and a sensation of abdominal mass. The patients only antecedent was an appendectomy for acute appendicitis 2 years earlier. A physical examination found HR: 120 /min RR: 20 /min BP: 130/80, and T 37.9. The patient was dehydrated, but her cardiopulmonary condition was normal. An abdominal examination showed pain upon palpation in the mesogastrium and left flank, but without irritation or defense. There was evidence of 10 x 10 cm mass at the mesogastric level. A rectal examination was normal.
At admittance the patients complete blood count showed 22,000 leukocytes/ml with 91% neutrophilia and 1% band neutrophils; HB 13.5; PQ interval 260; creatinine 0.68; blood urea nitrogen (BUN) 7.2; K 3.35; Na 137; CL 108; GA: PH 7.46; PCO2 32; HCO3 19; BEF -6.3 and PO2 64. A simple abdominal x-ray showed unspecified changes related to the ileum. Computerized axial tomography (CAT) demonstrated a noticeable proximal expansion of thin intestinal loops to the middle jejunum with an image suggestive of jejuno-jejunal intussusceptions and bowel wall edema with no pneumatosis intestinalis or pneumoperitoneum (Figure 1).
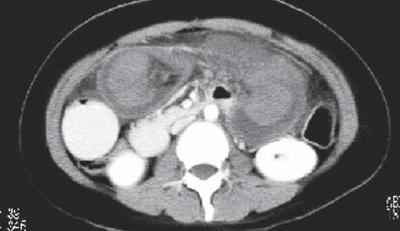
Figure 1. The image shows a noticeable proximal expansion of the small intestine with the presence of jejuno-jejunal intussusceptions associated with edema of the wall of the bowel loop.
Based on clinical findings and imaging, we performed a laparotomy which revealed a 30 centimeter segment of the proximal jejunum which was severely stretched with ischemic zones in the serous membrane, Impending intestinal perforation and internal mass sensation located approximately 60 cm from the ligament of Treitz. The mesenterium evidenced edema and ingurgitation. We performed resected a block of the compromised segment and manually performed lateral anastomosis along a plane using 3-0 vascular polypropylene sutures. The length of the surplus in situ small intestine was two meters. The patients postoperative evolution was satisfactory, and the patient was discharged four days after surgery with suitable oral tolerance and signs of complete intestinal transit.
When the resected piece was opened, a two meter long intussusception of the small intestine was found. A pathological report showed the presence of intestinal intussusception with transmural ischemic necrosis secondary to a 9.5 cm jejunal hamartomatous polyp.
CASE 2
A 40 year old female patient came to the emergency service of the University Hospital of San Ignacio (Bogotá, Col) after enduring three days of diffuse abdominal colic with multiple episodes of feculent vomiting, abdominal distension, diminution in the passage of flatulence and absence of defecation. Twenty days earlier the patient had had an abdominal CAT scan as a part of a study of a chronic abdominal pain. The CAT scan showed a 4cm mass in the transverse colon suggestive of lipoma. This mass was the head of a colocolic intussusception which was not endoscopically evaluated. The patients only antecedent was a uterine tubal ligation 6 years earlier. Physical examination found HR: 90, RR: 20, BP 120/80, T: 36.8, dehydration, and normal cardiopulmonary indications. The abdominal examination showed diffuse pain upon palpation with generalized defense and irritation. Further palpation revealed a 15cm x 15 cm mass in the mesogastrium and left flank.
A complete blood count at admittance showed 17,100 leukocytes/ml with 85% neutrophilia, Hb 13.5, PQ interval 260, creatinine 0.68, BUN 7.2, K 3.35, Na 137, CL 108, GA: PH 7.46, PCO2 32, HCO3 19, BEF 6.3, and PO2 64. A simple abdominal x-ray evidenced extremely high air fluid levels and distension of small bowel loops. There was no evidence of distal gas in the rectum ampulla.
With these findings we performed a laparotomy that showed a colocolonic intussusception that compromised the transverse and part of the descending colon. The transverse colon was perforated and partially everted with mucosal edema. The descending colon showed a necrosed 10 cm x 10 cm mass associated with multiple adenopathies in the mesenterium. The cecum reached a 14 cm diameter without macroscopic ischemic changes. A subtotal colectomy, a Hartmanns procedure and an ileostomy were performed. The patients postoperative evolution was satisfactory, and the patient was discharged seven days after surgery when the oral route had been reestablished. Complete signs of intestinal transit were found. Drainage due to the ileostomy was regulated by means of adjusting the dosage of loperamide.
The final pathology diagnosis reported that there had been an intussusception of the transverse colon secondary to a 5.5 cm diameter submucosal lipoma, perforated proximal ischemic colitis with peritonitis. Twenty two lymph nodes were negative for malignancy.
DISCUSSION
Telescoping of a segment of the gastrointestinal tract together with its mesenterium (intussuceptum) into the lumen (intussuscipiens) of a contiguous segment is called intussusception (1-5). Although its exact mechanism is unknown, the physiopathology suggests that intraluminal lesions alter normal peristalsis of the compromised segment and acts as the head of the intussuceptum.
Although this is a very frequently occurring pediatric pathology which is the main cause of intestinal obstruction in 6-18 month old patients (2), in adults intussusception is infrequent. Adult cases represent only about 6% of all cases of intussusceptions, while 94% are pediatric cases (1). Its incidence is 2 to 3 cases per year per million adults which accounts for only 0.003% to 0.02% of hospital admissions and only 1% of all cases of intestinal obstruction among adults (2-4).
Intussusception is commonly classified according to the segment of the gastrointestinal tract which is compromised. If only the small intestine is compromised, it is called enteric or enteroenteric. If only the large intestine is compromised, then it is colonic or colocolonic. If the cecum invaginates the terminal ileum, it is called ilecolic. If the ileocecal valve acts as the head of the intussuceptum, it is called ileocecal. Other less frequent types are those which involve the stomach, duodenum and surgical stomas.
Ninety per cent of these cases occur in the small and large intestines while the other 10% are gastroduodenal or intussusceptions of surgical stoma (5). There are definable pathological causes in 90% of all cases of intussusceptions in adults. Benign or malignant tumors account for 65% of cases (8). Colocolonic intussusceptions, which represent 8% to 19% of intussusception cases, are less common than those in the longer and more mobile small intestine. Its etiology is malignant in 50% to 80% of cases (1-4, 6). Cases in the descending colon are rare due to its fixed retroperitoneal position (10).
The most common symptoms are the same as those for intestinal obstructions. In some series intestinal obstruction was the preoperative diagnosis in 50% of patients (4). A series of cases at Massachusetts General Hospital by Chance et al. describes the clinical characteristics of 58 cases of intussusception that occurred between 1964 and 1993. The average age at presentation was 54 years old with a greater prevalence among males than females (1.8 to 1). The average duration of symptoms before the diagnosis was 37.4 days. They reported nausea, vomiting and abdominal pain in 78% of these patients and melena/rectal bleeding in only 29%. Thirty-two per cent of the patients were diagnosed with intussusception prior to surgery. In recent series with a greater use of abdominal CAT scans the rate of preoperative diagnosis has increased to 51% (7).
In both of the cases we have reported here, the presence of recently formed abdominal masses associated with severe abdominal pain and early signs of systemic inflammatory response were notable findings in the physical examinations. In one case symptoms were acute. The case of colocolonic intussusception documented a history of chronic abdominal pain and distension. The incidental CAT scan finding of the intussusception corroborated the chronicity and episodic presentation which this entity sometimes has.
In abdominal CAT scans the image of a loop within a loop, with or without the presence of vessels and mesenteric fat, is a pathognomonic finding of intussusception. Abdominal CAT scans are the most sensitive imaging technique for diagnosing intussusception as evidenced in the two cases presented. Visualization of fat is reported in 68% to 76% of all cases, and visualization of mesenteric vessels is reported in 54% to 61% of cases (9). The intususceptum is the center while the intussuscipiens edematous corresponds to the external ring of the characteristic image in Diana. The presence and configuration of the head of the intussusceptum, the degree of edema of the intussuscipiens wall, and the amount of invaginated mesenterium are factors that can distort these characteristic radiological findings (5). Another useful imaging method for diagnosis of colonic intussusception is a barium enema which has a reported sensitivity of 73% (7).
Warshauer and colleagues summarize the findings of eight observational studies that evaluated the causes of intussusception in 236 patients. One hundred twenty five cases (53%) had enteric locations while 111 (47%) had colonic locations. Ninety three cases (39%) were malignant tumoral and 63 (27%) were benign. Twenty nine cases were idiopathic (12%). Other cases with causes other than tumors were 29 post surgical bridles in 27 patients (11%) and 14 cases if Meckels diverticulum (6%) (9).
Both of the cases we report on in this article had benign mechanical factors related to intussusception. Although whether or not the size of a lesion is related to intussusception probability has yet to be defined, it is worth noting that both of the lesions we found were proportionally very large in relation to the portions of the gastrointestinal tract where they were located. In the first case a 9.5 cm hamartomatous polyp was located in the jejunum while in the second case a 10cm submucosal lipoma was found in the descending colon.
Adenomatous polyps and lipomas are two of the primary benign causes of intussusception. Lipomas are the primary benign etiology of coloconic intussusception, and the second most common benign colon tumor. Their reported prevalence is between 0.2% and 3% according to autopsy reports (8). Colonic lipomas are slow growing mesenchymal tumors which occur predominately in females, most frequently in the sixth decade of life. Ninety per cent of them are solitary submucosal cases. Their frequency diminishes outside of the colon. They are clinically invisible until their diameter is greater than 2cm. They may be suspected prior to surgery by the presence of a well delimited mass with greasy attenuation (-40 to -120 HU) that acts as the head of the intususceptum (5, 8). Nevertheless, the main colocolonic causes of intussusception are malignant primary colonic tumors such as adenocarcinoma, lymphoma and metastases (5).
Intussusception in adults is handled surgically. The main debate revolves around whether block resections are necessary, or whether reduction is a possibility. Although the reduction allows more limited resection, it should not be performed because of the theoretical risk of perforation and sowing of tumor cells and/or micro organisms into the peritoneal cavity (3, 6, 7).
Block resections of compromised segments were performed on the patients in both cases presented in this article. We did not perform any reduction of the segments involved during surgery. In both cases we found that the intususceptum had necrosed. We think that the maneuver we used is preferable to other options because it limits the risk of perforation, contamination, reperfusion injuries and bacterial translocation.
Although a greater incidence of right side colo-colonic intussusception, something which permits primary anastomosis in a non-prepared colon, has been reported, for left side lesions, such as the one of those reported in this article, it is preferable to perform a left hemicolectomy, a terminal colostomy and a Hartmman procedure with repetition of anastomosis at another time whenever this surgery is required in an emergency (4).
REFERENCES
1. Cavalleri A, Perrin H, Brunner P, et al. Colocolic tumoral intussusception in the adult: value of multi-slice spiral CT imaging. Clin Imaging 2007; 31(6): 428-30.
2. Correia JD, Lefebvre K, Gray DK. Surgical images: soft tissue. Transverse colonic intussusception. Can J Surg 2007; 50(1): 60-1.
3. Yalamarthi S, Smith RC. Adult intussusception: case reports and review of literature. Postgrad Med J 2005; 81(953): 174-7.
4. Azar T, Berger DL. Adult intussusception. Ann Surg 1997; 226(2): 134-8.
5. Kim YH, Blake MA, Harisinghani MG, et al. Adult intestinal intussusception: CT appearances and identification of a causative lead point. Radiographics 2006; 26(3): 733-44.
6. Erkan N, Haciyanli M, Yildirim M, et al. Intussusception in adults: an unusual and challenging condition for surgeons. Int J Colorectal Dis 2005; 20(5): 452-6. Epub 2005 Mar 10.
7. Barussaud M, Regenet N, Briennon X, et al. Clinical spectrum and surgical approach of adult intussusceptions: a multicentric study. Int J Colorectal Dis 2006; 21(8): 834-9. Epub 2005 Jun 11.
8. Gürses B, Kabakci N, Akyuz U, et al. Imaging features of a cecal lipoma as a lead point for colo-colonic intussusception. Emerg Radiol 2007.
9. Warshauer DM, Lee JK. Adult intussusception detected at CT or MR imaging: clinical-imaging correlation. Radiology 1999; 212(3): 853-60.
10. Jaremko JL, Rawat B. Colo-colonic intussusception caused by a solitary Peutz-Jeghers polyp. Br J Radiol 2005; 78(935): 1047-9.
1. Cavalleri A, Perrin H, Brunner P, et al. Colocolic tumoral intussusception in the adult: value of multi-slice spiral CT imaging. Clin Imaging 2007; 31(6): 428-30. [ Links ]
2. Correia JD, Lefebvre K, Gray DK. Surgical images: soft tissue. Transverse colonic intussusception. Can J Surg 2007; 50(1): 60-1. [ Links ]
3. Yalamarthi S, Smith RC. Adult intussusception: case reports and review of literature. Postgrad Med J 2005; 81(953): 174-7. [ Links ]
4. Azar T, Berger DL. Adult intussusception. Ann Surg 1997; 226(2): 134-8. [ Links ]
5. Kim YH, Blake MA, Harisinghani MG, et al. Adult intestinal intussusception: CT appearances and identification of a causative lead point. Radiographics 2006; 26(3): 733-44. [ Links ]
6. Erkan N, Haciyanli M, Yildirim M, et al. Intussusception in adults: an unusual and challenging condition for surgeons. Int J Colorectal Dis 2005; 20(5): 452-6. Epub 2005 Mar 10. [ Links ]
7. Barussaud M, Regenet N, Briennon X, et al. Clinical spectrum and surgical approach of adult intussusceptions: a multicentric study. Int J Colorectal Dis 2006; 21(8): 834-9. Epub 2005 Jun 11. [ Links ]
8. Gürses B, Kabakci N, Akyuz U, et al. Imaging features of a cecal lipoma as a lead point for colo-colonic intussusception. Emerg Radiol 2007. [ Links ]
9. Warshauer DM, Lee JK. Adult intussusception detected at CT or MR imaging: clinical-imaging correlation. Radiology 1999; 212(3): 853-60. [ Links ]
10. Jaremko JL, Rawat B. Colo-colonic intussusception caused by a solitary Peutz-Jeghers polyp. Br J Radiol 2005; 78(935): 1047-9. [ Links ]

