










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.3 Bogotá set. 2011
Comparison of sequential therapy for eradication of Helicobacter pylori with standard triple therapy
Martín Gómez Zuleta (1), Christian Melgar Burbano (2), William Otero Regino (3)
(1) Assistant Professor of Gastroenterology at the Universidad Nacional de Colombia, Gastroenterologist at the Hospital El Tunal, Clínica Universitaria Carlos Lleras Restrepo, Bogotá, Colombia.
(2) Internist, Gastroenterology Fellow at the Universidad Nacional de Colombia. Bogotá, Colombia.
(3) Associate Professor of Gastroenterology at the Universidad Nacional de Colombia, Gastroenterologist at the Clínica Fundadores, Hospital El Tunal, Clínica Universitaria Carlos Lleras Restrepo. Bogotá, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 25-01-11 Accepted: 02-08-11
Abstract
Introduction: Helicobacter pylori are involved in a large number of pathologies. Although first line therapies were developed to achieve high eradication rates, in recent years they have lost effectiveness. This has lead to the use of new therapies such as sequential therapy. This study compares eradication rates and collateral effects of sequential therapy (ST) and standard triple therapy (STT).
Methods: This is a prospective randomized study of patients at El Tunal Hospital performed between November 2008 and September 2010. The study included patients with functional dyspepsia or peptic ulcers between 19 and 70 years of age who had undergone high digestive endoscopy for dyspeptic symptoms. Patients had not received H. Pylori eradication treatments for at least three months prior to endoscopies nor had they received antisecretory medications, bismuth or antibiotics during the previous month. Statistical calculations were done with SPSS.
Results: At the end of the study 165 patients were included: 85 in the STT group (Group A) and 80 in the ST group (Group B). In group A 60 out of 80 patients (75 %) completed the treatment, but the infection was eradicated in only 51 patients for an 85% efficacy rate according to the protocol (95% CI: 7392) and 63.75 % according to intention to treat (95% CI: 5274). In Group B 70 out of 85 patients (82 %) completed the treatment, but the infection was eradicated in only 53 patients for a 75% efficacy rate according to the protocol (95% CI: 6385) and 62% according to intention to treat (95% CI: 51-72).
Conclusions: This study found low success rates with both STT and TS using generic medications in a population in Bogota. We consider it necessary to conduct similar studies using original medications and to conduct research about resistance to currently recommended antimicrobials in this population.
Keywords
Helicobacter pylori, eradication, sequential therapy, triple therapy.
On a world-wide level Helicobacter pylori (H. Pylori) represents an important cause of morbidity and mortality. It is the main etiological agent of diverse gastrointestinal diseases such as gastric and duodenal peptic ulcers, gastric cancer and gastric MALT lymphoma (1-3). In addition, two extra intestinal entities, iron deficiency anemia (4) and immune thrombocytopenic purpura (5), are currently considered to be related to this infection. H. Pylori infects more than a half of the population of the world, but its prevalence is greater in developing countries (6) where it affects more than 80% of adults in contrast to only 20 to 50% in developed countries (7,8). Considering the link that this infection has with various entities mentioned, it is considered that eradication is indicated for infected patients (1). The eradication therapy that has been most frequently recommended by experts and scientific associations is "standard triple therapy" (STT) (9-12), which consists of the simultaneous administration of a pump proton inhibitor (PPI), clarithromycin (CL) and for seven to ten days. Metronidazole is substituted for amoxicillin when there is allergy to amoxicillin (MTD).
Many early studies in different parts of the world demonstrated that the average effectiveness of STT was 90% (9, 13.14). This level of effectiveness was also found here in Colombia (15-17). Nevertheless in the last 15 years, success with this therapy has dramatically decreased, reaching a range of 57% to 73% in seven day therapies and 67% to 79% in ten days therapies (14). The reduction in its effectiveness has been essentially attributed to the development of resistance to clarithromycin and metronidazole (1,14). In Colombia this resistance is over 15% for clarithromycin and 80% for metronidazole (18-20). Considering, the magnitude of this loss of efficacy, it has been recommended that STT be replaced with the sequential therapy (ST) developed by Zullo in Italy (21) and later studied by other authors (22-24). It consists of PPI treatment for ten days combined with 1gram of amoxicillin twice a day for the first five days and then 500 mgs of clarithromycin plus 500 mgs of Tinidazole twice a day for the last five days. The efficacy of ST has been higher than 90% (22-26). Recent metaanalyses have concluded that the crude rate of efficacy of this therapy is 93.4% whereas that of STT is only 76.9% (21). When resistance to clarithromycin is present ST continues to be effective, eradicating 90% of these infections in contrast to only 28.6% for standard triple therapy (23). A more recent study in Spain (26) found 84% efficacy by intention to treat and 90% by protocol while another recent study in Korea showed that sequential therapy was effective in 80.8% of cases (27).
We decided to undertake this study for the following reasons:
1. No studies of the efficacy of STT have been conducted. Its effectiveness remains unknown even though the rate of resistance to Clarithromycin in Colombia surpasses the 40% level which is considered to be the limit for its use as a first line therapy (1).
2. Until now there is no data on the rate of successes for ST. We wanted to determine if this therapy is effective in a country with high prevalence of resistance to metronidazole.
3. Medicines used in the current social security system of Colombia are essentially generic. Therefore it would be of interest to establish the effectiveness of therapeutic schemes that use them to eradicate H. Pylori. The objective of the present work is to establish and to compare the effectiveness of an STT scheme with ST using the generic medicines of the current obligatory health plans in Colombia (POS).
MATERIALS AND METHODS
This is a prospective randomized study of patients at El Tunal Hospital performed between November 2008 and September 2010. The report of this study follows all CONSORT (Consolidated Standards of Reporting Trials) recommendations for clinical test quality in parallel groups (29).
Inclusion criteria
The study included patients with functional dyspepsia or peptic ulcers who were between 19 and 70 years of age who had been referred for high digestive endoscopy for dyspeptic symptoms. Patients had not received previous H. Pylori eradication treatments within the three months prior to the referral and had not received antisecretory drugs, bismuth or antibiotics for one month prior to referral. Functional dyspepsia is defined here as postprandial distress (B1a) or abdominal pain (B1b) according to the 2006 ROMA III criteria (30).
Exclusion criteria
Patients with serious concomitant diseases including congestive cardiac failure (CCF), cerebrovascular disease (CVD), decompensated diabetes, coagulation alterations, and cirrhosis were excluded. Patients who had had prior gastric surgery, or had allergies to penicillin or IBP, or were addicted to drugs or alcohol, or who had psychiatric illnesses were also excluded. In addition, women in their reproductive years who were not using birth control or who were pregnant or lactating were excluded.
After receiving a complete and detailed explanation of the study, patients who were included in the study signed an informed consent form before entering the study. A specifically designed form was used to record demographic and other variables that were included in the study. The protocol and the informed consent were approved by the ethics committees of the participating institutions.
Two of the authors (MG and WO) performed the upper digestive endoscopies (UDEs). UDEs were performed the morning after a patient had fasted for a minimum of six hours. Patients were in left lateral position and were no sedated. The pharynx of each patient was anaesthetized with two 20 mg applications of lidocaine spray (roxicaina topical solution, Ropsohn Therapeutics®). An Olympus Exera CB 145 was used for all UDEs. During each upper digestive endoscopy two biopsies were taken from locations in the antrum two centimeters from the pylorus (one from the greater curvature and the other from the lesser curvature), and two additional biopsies were taken from locations in the corpus eight centimeters from the cardia, one from the anterior wall and one from the posterior wall. One biopsy was taken from the angular incisure. All biopsies followed the protocol recommended by experts (31) which has demonstrated that it can identify H pylori in all infected patients. All biopsies were immersed in 10% buffered formalin and sent to the pathology laboratory. Biopsies were colored with hematoxylin and eosin to identify H. Pylori. When this did not identify the infection, Giemsa coloring was used. A diagnosis of H. Pylori infection was established when the microorganism was identified in any of the patient's biopsies. The pathology group did not know the characteristics of the patients. The patients included in the study were randomized for treatment. Patients were informed of the type of treatment they would undergo in a written notification delivered in an envelope by a doctor who was not part of the study. The envelopes' contents were unknown to the investigators. At the moment a patient was informed of his/her treatment procedures, s/he was also informed of potential adverse effects and the necessity to suspend treatment in the event of severe adverse effects (diarrhea, vomiting, allergies, migraines etc.). After treatment ended, patients were again interviewed to complete information on adverse effects and fulfillment of treatment which was measured by counting medication remaining in the patient's "pill box". Verification of eradication was determined in the same way as was the original diagnosis: by means of an endoscopy performed six to eight weeks after treatment ended.
Patients were called by telephone on the fifth and eleventh day of treatment and were asked about adverse effects of treatment. Their responses were recorded on a form. Adverse effects were defined as symptoms which patients had not reported prior to start of treatment
Study design, randomization and sample size calculation
The investigation was designed to be an open randomized prospective study at a level three hospital in Bogota. A computer generated randomization list determined which patients would receive treatment A and which would receive treatment B. Patients were informed of the characteristics of the medicines that would be used to treat their H. Pylori infections. The sample size calculation assumed that the STT had an 85% eradication rate and that the experimental sequential therapy (ST) had a 92% eradication rate. These assumptions were based on average eradication rates in Colombia medium and in the published literature. Cluster Sample Size 1.0 was used to make the sample size calculation. A normal approximation was used with the continuity correction method under the following criteria: Type I error: 5%, Type II error: 10%, 85% eradication rate in control group, 92% eradication rate in experimental group with allocation rate between groups of 2.
The sample size according to the calculations was 75 patients in each group with an additional 10% in each group in anticipation of losses. The treatment groups were defined as follows:
Scheme A was STT for 10 days: 20 mg omeprazole before breakfast, 20 mgs before dinner, 500 mgs clarithromycin after breakfast, 500 mgs after dinner, 1 gram amoxicillin after breakfast and 1 gram after dinner.
Scheme B was ST for 10 days: 20 mg omeprazole before breakfast, 20 mgs before dinner for ten days, 1 gram amoxicillin after breakfast and 1 gram after dinner for the first five days. For the last five days, 500 mg tinidazole after breakfast and 500 mgs after dinner, plus 500 mg clarithromycin after breakfast and 500 mg after dinner, replaced Amoxicillin.
Statistical Analysis
SPSSS 10 was used for statistical calculations. Comparison of qualitative variables was done by means of the chi square test or Fisher's exact test depending upon which was appropriate for the Student's T test distribution. P < 0.05 was considered significant. Efficacy analyses were conducted for both intention to treat (ITT) and protocol (PP).
Results
At the end of the study 165 patients were included: 85 in the STT group and 80 in the ST group. Table 1 shows the patients' characteristics and Figures 1 and 2 shows a diagram of the population studied.
Table 1. Patients’ characteristics and treatment indications.
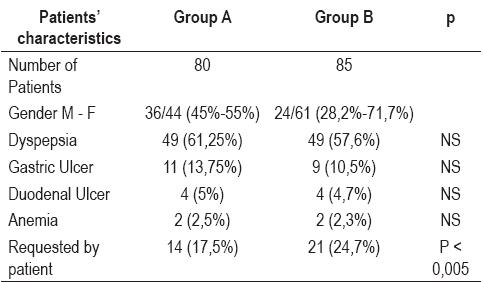
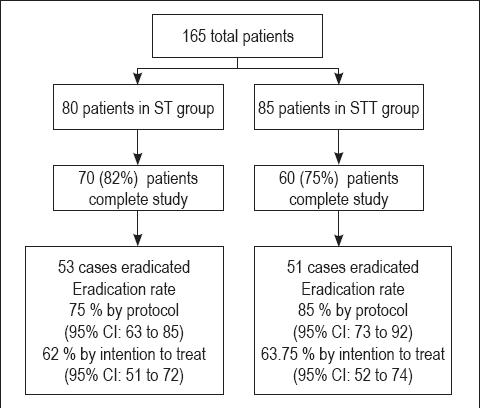
Figure 1. Diagram of population studied.
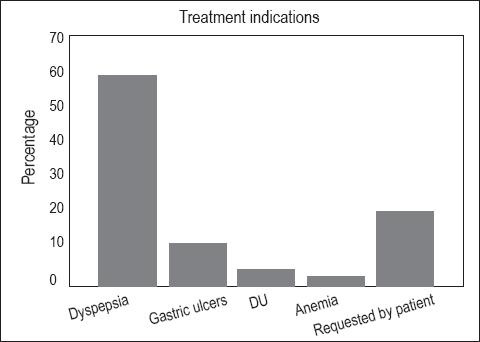
Figure 2. Treatment indications.
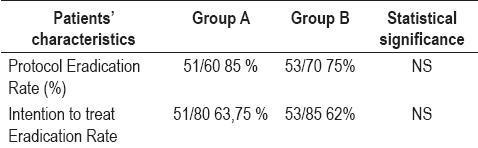
In Group A (STT), 60 out of 80 completed the treatment (75 %). Among these the infection was eradicated in 51 giving an 85% efficacy rate by protocol (95% CI: 73 to 92) and 63.75 % by intention to treat (95% CI: 52 to 74). Patients that did not complete the study dropped out of the study; none of them retired due to adverse effects. In Group B (ST), 70 out of 85 (82 %) completed the treatment. Among these the infection was eradicated in 53 patients giving a 75% efficacy rate by protocol (95% CI: 63 to 85) and 62% by intention to treat (95% CI: 51 to 72).
The eradication rate by protocol among patients from 18 to 40 years of age in Group A was 100% (95% CI: 0.59 to 1.0). Among patients over 40 years of age it was 88.4% (95% CI: 69 to 97). In Group B the eradication rate by protocol among patients from 18 to 40 years of age was 90.9% (95% CI: 58 99), and among patients over 40 years of age it was 68% (95% CI: 46 to 85) (Table 2).
Table 2. Eradication Rate Comparison.
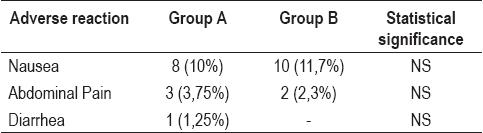
The adverse effects in the two treatment groups are shown in Table 3. None of the losses from the groups were related to adverse effects.
Table 3. Adverse Effects of Treatment.
DISCUSSION
This study discovered that STT has a 64% efficacy rate by intention to treat, which is far below the 90% suggested by experts as a condition for a treatment to be considered a useful first line therapy (32) and also well below the 80% threshold for intention to treat recommended by the last Maastricht consensus (1,33). The eradication rate for STT coincides with international publications which find eradication rates from 67% to 69% with the same STT (14), but our result contrasts with the results of similar studies conducted in our country more than a decade ago. Those results for eradication rates ranged from 87% to 92% (15-17). With such a low success rate, this therapy is in the "unacceptable" ranks according to the recent recommendation published by experts since it is less than 80% (23). Sequential therapy presented no drawbacks in terms of patients' understanding of dosage, contrary to the indications of some authors (2327).
Although our results are consistent with current world developments, it is important to take into account that the medications used in this study were generic (with the exception of clarithromycin which is not covered by the POS system). Even though these medications are internationally accepted as having some similitude with the original medications, we do not know if the bioequivalence and bioavailability studies have been conducted in our country for these generic medications that would determine their comparability to the original drugs. Even though biological plausibility exists, and even though it would explain the decrease in STT efficacy as well as the high rate of resistance (over 15%) to clarithromycin (19, 20), we consider that to be certain about the decreased effectiveness of STT in Colombia, studies using the original medications are necessary. The best option would be a multicentric study.
Recently Dr. Correa's group in Pasto demonstrated an 85% eradication rate with STT by intention to treat (34). Rates of resistance to clarithromycin and metronidazole were not mentioned, although they are probably low since high resistance rates cause STT eradication rates to noticeably decrease. The study also does not mention if original medication was used original (1, 14). Nevertheless, it would not be surprising if there are low rates of resistance to Clarithromycin in Pasto since Álvarez et al. recently found a 3.8% resistance rate to Clarithromycin in central-western Colombia (35). In addition to the high proportion of patients who dropped out of our study, one of the study's weaknesses was that antibiotic resistance was not studied. As a result we are uncertain if the low rate of eradication is due to the use of generic medication or to resistance to Clarithromycin. Even though the acceptable 85% eradication rate by protocol might suggest that the resistance to Clarithromycin is low in the studied population, a more reliable method of verification of eradication such as the urea breath test or fecal antigen test was not used (1). Consequently there could be an underestimation of the real eradication of STT since only histology was used. With the results of the present study we can conclude that, at the minimum, STT with medication used in the POS system is not efficient. Also, this study found that ST eradication efficacy was less than that found internationally. Data collected in 22 clinical trials including 2,388 patients demonstrated an average 91.3% eradication rate by intention to treat (95% CI:.90.2 to 92.5) and a 93.7% average eradication rate by protocol (95% CI: 92.7 to 94.7%), In comparison our study found a 62% eradication rate by intention to treat (95% CI: 51 to 72) and a 75% eradication rate by protocol (95% CI: 63 to 85). The rates found in our study were also lower than those found in Spain of 84% by intention to treat and 90% by protocol (26). As mentioned above for STT, since medication used in ST is also "generic", it is still necessary to evaluate the behavior of these therapies using the original medications. Such a study should also to take into account the increasing levels of resistance to clarithromycin and metronidazole here in Colombia (20).
Since results for intention to treat for both STT and ST were similar in our study, the national scientific community which treats patients infected with H. Pylori and the health care authorities of Colombia should consider this infection to be a priority. Wider research regarding eradication therapies for this infection should be undertaken now. This is especially so because in the "real life scenario" using POS medications and results by intention to treat, no effective first line therapies are now available. Consequently it is necessary to begin concomitant therapies or triple therapies with levofloxacin. In other countries these treatments have been shown to have superior efficacies to the treatments examined in this study (14, 36). There were no statistically significant differences in relation to adverse effects between the two groups.
In conclusion, the current study found low rates of success with both STT and ST using generic medications in a population in Bogota. We consider it necessary to conduct similar studies using original medications and to conduct research regarding resistance to antimicrobials in this population, as is currently recommended (20).
Conflicts of interest
None.
REFERENCES
1. Malfertheiner P, Megraud F, O´Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut 2007; 56: 772-81.
2. McNamara D, El-Omar E. Helicobacter pylori infection and the pathogenesis of gastric cancer: A paradigm for host-bacterial interactions. Dig Liv Dis 2008; 40: 504-9.
3. Otero W, Gómez M, Castro D. Carcinogénesis gástrica. Rev Col Gastroenterol 2009; 24: 314-329.
4. Muhsen K, Cohen D. Helicobacter pylori infection and iron stores: a systematic review and meta-analysis. Helicobacter 2008; 13: 323-40.
5. Stasi R, Satparwari A, Segal JB, Osborn J, Evangelista ML, Cooper N, et al. Effects of eradication Helicobacter pylori infection in patients with immune thrombocytopenic purpura: a systematic review. Blood 2009; 113: 1231-40.
6. Zhang YY, Xia HHX, Zhuang ZH, Zhong J. Review article: "true" reinfection of Helicobacter pylori after successful eradication-worldwide annual rates, risk factors and clinical implications. Aliment Pharmacol Ther 2008; 29: 145-160.
7. Huang JQ, Hunt RH. The evolving epidemiology of Helicobacter pylori infection and gastric cancer. Can J Gastroenterol 2003; 17 Suppl B: 18B-20B.
8. Suebaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002; 347: 1175-86.
9. Howden CW, Hunt RH. Guidelines for the management of Helicobacter pylori. Ad Hoc Committee on practice parameters of the American College of Gastroenterology. Am J Gastroenterol 1998; 93: 2330-8.
10. Lam SK, Talley NJ. Report of the 1997 Asia Pacific Consensus Conference on the management of Helicobacter pylori infection. J Gastroenterol Hepatol 1998; 13: 1-12.
11. Bytzer P, O´Morain C. Treatment of Helicobacter pylori Helicobacter 2005; 10 (Suppl 1): 40-46.
12. Wolle K, Malfertheiner P. Treatment of Helicobacter pylori. Best Pract Res Clin Gastroenterol 2007; 21: 315-24.
13. Chey WD, Wong BCY. American College of Gastroenterology Guideline on the Management of Helicobacter pylori Infection. Am J Gastroenterol 2007; 102:1808-25.
14. Otero W, Trespalacios AA, Otero E. Tratamiento de Helicobacter pylori. Un importante reto en gastroenterología. Rev Col Gastroenterol 2009; 24: 279-292.
15. Gutiérrez O, Otero W, Páez O, Roldán L, Lima E, Reyes R y col. Terapia triple con lansoprazol, amoxicilina y claritromicina durante 10 días (LAC-10) erradica Helicobacter pylori. Rev Colomb Gastroenterol 2001; 16: 132-135.
16. Otero W, Gutiérrez O, Quintero F, Orozco C, Ibáñez M. Eficacia de pantoprazol con claritromicina y amoxicilina para la erradicación de Helicobacter pylori en pacientes con úlcera duodenal o dispepsia no ulcerosa. Rev Col gastroenterol 2000; 15: 247-51.
17. Sierra F, Otero W, Gutiérrez O, Molano B. One week Full-dose Triple Therapy: New Standard for H. Pylori Treatment in Latin America. Gastroenterology 1996; 110: A258.
18. Henao S, Otero W, Martínez J, Ángel LA. Resistencia primaria de Helicobacter pylori a metronidazol en Colombia. Rev Col Gastroenterol 2009; 24: 10-15.
19. Henao SC, Quiroga A, Martínez JD, Otero W. Resistencia primaria a claritromicina en aislamientos de Helicobacter pylori. Rev Col Gastroenterol 2009; 24: 110-115.
20. Trespalacios AA, Otero W, Mercado Marcela. Resistencia de Helicobacter pylori a claritromicina, amoxicilina y metronidazol en pacientes colombianos. Rev Col Gastroenterol 2010; 25: 31-8.
21. Zullo A, Rinaldi V, Winn S, et al. A New highly effective short-term therapy schedule for Helicobacter pylori eradication. Aliment Pharmacol Ther 2000; 14: 715-8.
22. Jafri NS, Hornung CA, Howden CA. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naïve to treatment. Ann Intern Med 2008; 148: 1-10.
23. Graham DY, Lu H, Yamaoka Y. A report card to grade Helicobacter pylori therapy. Helicobacter 2007; 12: 275-8.
24. Vaira D, Zulo A, Vakil N, Gatta L, Ricci C, Perna F, et al. Sequential therapy versus standard triple drug therapy for Helicobacter pylori eradication. Ann Intern Med 2007; 146: 556-63.
25. Zullo A, Vaira D, Vakil N, High eradication rates of Helicobacter pylori with a new sequential treatment. Aliment Pharmacol Ther 2003; 17: 719-26.
26. De Francesco V, Zullo A, Margiotta M, Sequential treatment for Helicobacter pylori does not share the risk factors of triple therapy failure. Aliment Pharmacol Ther 2004; 19: 407-14.
27. Sanchez-Delgado J, Calvet X, Bujanda L, Gisbert J, Titó L, Castro M, Ten Day sequential treatment for Helicobacter pylori eradication in clinical practice. Am J gastroenterol 2008; 103: 1-4.
28. Park S, Chun HJ, Kim ES, Patk SC, Jung ES, Lee SD, et al. The 19-day sequential therapy for Helicobacter pylori eradication in Korea: Less effective tan expected. AGA 2009, Gastroenterology Suppl 1: Abstract M1053.
29. Moher D, Schulz KF, Altman DG. The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomized trials. Lancet 2001; 357: 1191-4.
30. Jack J, Talley NJ, Camillero M, at al. Functional gastroduodenal disorders. Gastroenterology 2005; 130:1466-79.
31. Dixon MF, Genta RM, Yardley JH, et al. Classification and grading of gastritis. The updated Sydney system. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996; 20: 1161-81.
32. Hopkins RJ. In search to the Holy Grail of Helicobacter pylori remedies. Helicobacter 2001; 6: 81-3.
33. Current European concepts in the management of Helicobacter pylori infection. The Maastricht Consensus Report. European Helicobacter pylori Study Group. Gut 1997; 41: 8-13.
34. Fischbach LA, Bravo LE, Zarama GR, Bravo JC, Ojha PR, Priest EL, et al. A randomized clinical trial to determine the efficacy of regimens containing clarithromycin, Metronidazole, and Amoxicillin among histological subgroups for Helicobacter pylori eradication in a developing country. Helicobacter 2009; 14: 100-8.
35. Álvarez A, Moncayo JL, Santacruz JL, Santacoloma M, Corredor LF, Reinosa E. Antimicrobial susceptibility and mutations involved in clarithromycin resistance in Helicobacter pylori isolates from patients in the western central region of Colombia. Antimicr Ag Chemoter 2009; 53: 4022-4.
35. Gisbert JP. "Rescue regimens after Helicobacter pylori treatment failure. World J Gastroenterol 2008; 14: 5385-5402.
1. Malfertheiner P, Megraud F, O'Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut 2007; 56: 772-81. [ Links ]
2. McNamara D, El-Omar E. Helicobacter pylori infection and the pathogenesis of gastric cancer: A paradigm for host-bacterial interactions. Dig Liv Dis 2008; 40: 504-9. [ Links ]
3. Otero W, Gómez M, Castro D. Carcinogénesis gástrica. Rev Col Gastroenterol 2009; 24: 314-329. [ Links ]
4. Muhsen K, Cohen D. Helicobacter pylori infection and iron stores: a systematic review and meta-analysis. Helicobacter 2008; 13: 323-40. [ Links ]
5. Stasi R, Satparwari A, Segal JB, Osborn J, Evangelista ML, Cooper N, et al. Effects of eradication Helicobacter pylori infection in patients with immune thrombocytopenic purpura: a systematic review. Blood 2009; 113: 1231-40. [ Links ]
6. Zhang YY, Xia HHX, Zhuang ZH, Zhong J. Review article: "true" reinfection of Helicobacter pylori after successful eradication-worldwide annual rates, risk factors and clinical implications. Aliment Pharmacol Ther 2008; 29: 145-160. [ Links ]
7. Huang JQ, Hunt RH. The evolving epidemiology of Helicobacter pylori infection and gastric cancer. Can J Gastroenterol 2003; 17 Suppl B: 18B-20B. [ Links ]
8. Suebaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002; 347: 1175-86. [ Links ]
9. Howden CW, Hunt RH. Guidelines for the management of Helicobacter pylori. Ad Hoc Committee on practice parameters of the American College of Gastroenterology. Am J Gastroenterol 1998; 93: 2330-8. [ Links ]
10. Lam SK, Talley NJ. Report of the 1997 Asia Pacific Consensus Conference on the management of Helicobacter pylori infection. J Gastroenterol Hepatol 1998; 13: 1-12. [ Links ]
11. Bytzer P, O'Morain C. Treatment of Helicobacter pylori Helicobacter 2005; 10 (Suppl 1): 40-46. [ Links ]
12. Wolle K, Malfertheiner P. Treatment of Helicobacter pylori. Best Pract Res Clin Gastroenterol 2007; 21: 315-24. [ Links ]
13. Chey WD, Wong BCY. American College of Gastroenterology Guideline on the Management of Helicobacter pylori Infection. Am J Gastroenterol 2007; 102:1808-25. [ Links ]
14. Otero W, Trespalacios AA, Otero E. Tratamiento de Helicobacter pylori. Un importante reto en gastroenterología. Rev Col Gastroenterol 2009; 24: 279-292. [ Links ]
15. Gutiérrez O, Otero W, Páez O, Roldán L, Lima E, Reyes R y col. Terapia triple con lansoprazol, amoxicilina y claritromicina durante 10 días (LAC-10) erradica Helicobacter pylori. Rev Colomb Gastroenterol 2001; 16: 132-135. [ Links ]
16. Otero W, Gutiérrez O, Quintero F, Orozco C, Ibáñez M. Eficacia de pantoprazol con claritromicina y amoxicilina para la erradicación de Helicobacter pylori en pacientes con úlcera duodenal o dispepsia no ulcerosa. Rev Col gastroenterol 2000; 15: 247-51. [ Links ]
17. Sierra F, Otero W, Gutiérrez O, Molano B. One week Full-dose Triple Therapy: New Standard for H. pylori Treatment in Latin America. Gastroenterology 1996; 110: A258. [ Links ]
18. Henao S, Otero W, Martínez J, Ángel LA. Resistencia primaria de Helicobacter pylori a metronidazol en Colombia. Rev Col Gastroenterol 2009; 24: 10-15. [ Links ]
19. Henao SC, Quiroga A, Martínez JD, Otero W. Resistencia primaria a claritromicina en aislamientos de Helicobacter pylori. Rev Col Gastroenterol 2009; 24: 110-115. [ Links ]
20. Trespalacios AA, Otero W, Mercado Marcela. Resistencia de Helicobacter pylori a claritromicina, amoxicilina y metronidazol en pacientes colombianos. Rev Col Gastroenterol 2010; 25: 31-8. [ Links ]
21. Zullo A, Rinaldi V, Winn S, et al. A New highly effective short-term therapy schedule for Helicobacter pylori eradication. Aliment Pharmacol Ther 2000; 14: 715-8. [ Links ]
22. Jafri NS, Hornung CA, Howden CA. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naïve to treatment. Ann Intern Med 2008; 148: 1-10. [ Links ]
23. Graham DY, Lu H, Yamaoka Y. A report card to grade Helicobacter pylori therapy. Helicobacter 2007; 12: 275-8. [ Links ]
24. Vaira D, Zulo A, Vakil N, Gatta L, Ricci C, Perna F, et al. Sequential therapy versus standard triple drug therapy for Helicobacter pylori eradication. Ann Intern Med 2007; 146: 556-63. [ Links ]
25. Zullo A, Vaira D, Vakil N, High eradication rates of Helicobacter pylori with a new sequential treatment. Aliment Pharmacol Ther 2003; 17: 719-26. [ Links ]
26. De Francesco V, Zullo A, Margiotta M, Sequential treatment for Helicobacter pylori does not share the risk factors of triple therapy failure. Aliment Pharmacol Ther 2004; 19: 407-14. [ Links ]
27. Sanchez-Delgado J, Calvet X, Bujanda L, Gisbert J, Titó L, Castro M, Ten Day sequential treatment for Helicobacter pylori eradication in clinical practice. Am J gastroenterol 2008; 103: 1-4. [ Links ]
28. Park S, Chun HJ, Kim ES, Patk SC, Jung ES, Lee SD, et al. The 19-day sequential therapy for Helicobacter pylori eradication in Korea: Less effective tan expected. AGA 2009, Gastroenterology Suppl 1: Abstract M1053. [ Links ]
29. Moher D, Schulz KF, Altman DG. The CONSORT statement: Revised recommendations for improving the quality of reports of parallel-group randomized trials. Lancet 2001; 357: 1191-4. [ Links ]
30. Jack J, Talley NJ, Camillero M, at al. Functional gastroduodenal disorders. Gastroenterology 2005; 130:1466-79. [ Links ]
31. Dixon MF, Genta RM, Yardley JH, et al. Classification and grading of gastritis. The updated Sydney system. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996; 20: 1161-81. [ Links ]
32. Hopkins RJ. In search to the Holy Grail of Helicobacter pylori remedies. Helicobacter 2001; 6: 81-3. [ Links ]
33. Current European concepts in the management of Helicobacter pylori infection. The Maastricht Consensus Report. European Helicobacter pylori Study Group. Gut 1997; 41: 8-13. [ Links ]
34. Fischbach LA, Bravo LE, Zarama GR, Bravo JC, Ojha PR, Priest EL, et al. A randomized clinical trial to determine the efficacy of regimens containing clarithromycin, Metronidazole, and Amoxicillin among histological subgroups for Helicobacter pylori eradication in a developing country. Helicobacter 2009; 14: 100-8. [ Links ]
35. Álvarez A, Moncayo JL, Santacruz JL, Santacoloma M, Corredor LF, Reinosa E. Antimicrobial susceptibility and mutations involved in clarithromycin resistance in Helicobacter pylori isolates from patients in the western central region of Colombia. Antimicr Ag Chemoter 2009; 53: 4022-4. [ Links ]
36. Gisbert JP. "Rescue regimens after Helicobacter pylori treatment failure. World J Gastroenterol 2008; 14: 5385-5402. [ Links ]

