










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.3 Bogotá set. 2011
Reflux laryngitis: an Otolaryngologist's perspective
Luis Humberto Jiménez Fandiño, MD (1), Natalia Mantilla Tarazona, MD (2), Javier Andrés Ospina Díaz, MD (3)
(1) Otolaryngologist and Maxillofacial Surgeon. Director of Laryngology and Pathology in the Voice Section of the Otolaryngology Unit at the Hospital Universitario San Ignacio, Pontificia Universidad Javeriana. Bogotá, Colombia jimenez-luis@javeriana.edu.co.
(2) Otolaryngologist. Pontificia Universidad Javeriana. Bogotá, Colombia.
(3) Otolaryngologist. Pontificia Universidad Javeriana. Bogotá, Colombia
Translated by T.A. Zuur and The Language Workshop
Received: 29-03-11 Accepted: 02-08-11
Abstract
Reflux laryngitis is recognized as an extra-digestive manifestation of gastroesophageal reflux. It has become one of the most frequent reasons patients consult with otolaryngologists. In this review we present the otolaryngologist's point of view on this disease, and discuss the continuing controversy about its pathophysiology, diagnosis and treatment.
Key words
Laryngitis, gastroesophageal reflux disease (GERD), laryngopharyngeal reflux.
INTRODUCTION
Reflux laryngitis, also known as laryngopharyngeal reflux (LPR), is one of the extra-digestive manifestations of gastroesophageal reflux disease (GERD) that is produced by the retrograde flow of the gastric contents (acid, pepsin) or duodenal contents (biliary salts, pancreatic enzymes) toward the larynx and the pharynx (1). Although GERD and LPR are considered to be part of a spectrum within one disease with a multifactorial etiology, they differ in their symptoms, clinical manifestations and responses to treatment.
Gastric content reflux can affect organs and systems in the vicinity of the digestive system as proven by descriptions of a B association between reflux tide and various inflammatory pathologies of the head and neck. These include chronic rhinosinusitis, allergic rhinitis, recurrent tonsillitis, hypertrophy of the tonsils and adenoids, obstructive sleep apnea-hypopnea syndrome (OSAHS), asthma, bronchiecstasis, pneumonia, chronic cough, dysphagia, laryngomalacia, pharyngitis, tracheitis, and subglotic stenosis (2-5). There have even been findings of high levels of pepsin in the middle ear and the adenoids of patients with otitis media with effusion (OME). It is believed that the pepsin reaches the middle ear in gastric content that ascends through the nasopharynx and the eustachian tube. This establishes an important association between OME's pathogenesis and chronic otitis media (6-8).
Although data about the relation of gastric reflux and extra-digestive laryngeal manifestations has been published in the literature of otolaryngology for at least four decades (9), it was first named LPR by Koufman at the beginning of the 1990's (10). Since then this entity has been diagnosed more and more frequently by otolaryngologists, to the point that it is over-diagnosed. From 1990 to 2001in the United States, the number of visits to doctors, especially to otolaryngologists, for diseases related to gastroesophageal reflux increased 306%. Prescription of pump proton inhibitors (PPI) increased 14 times (11).
In this article we will review current concepts of LPR, present controversies about the reality of its existence and its diagnosis and treatment, and discuss the otolaryngologist's role in the handling of these patients.
EPIDEMIOLOGY AND PHYSIOPATHOLOGY
The erratic form of presentation of this disease combined with the current absence of a highly sensitive and specific diagnostic method for diagnosing GERD and LPR makes it impossible to determine the real impact and association of these pathologies.
For otolaryngologists, LPR and GERD play an increasingly important role. The evidence shows a significant increase in diagnoses and treatment of reflux related diseases (11). In the United States the direct cost of antireflux treatment (especially PPIs) is esteemed at more than 14 trillion dollars per year. This does not include the costs of medical appointments, diagnostic tests or indirect costs related to effects on labor productivity and quality of life (12).
Some studies show that up to 10% of the patients who go to an otolaryngologist present symptoms related to LPR and that approximately 50% of patients with dysphonia have signs of underlying reflux disease (10,11).
Currently, we do not have sufficient evidence about the relation between GERD and LPR. This is partly due to the fact that patients with LPR who have otolaryngological symptoms do not present common symptoms related to GERD such as epigastralgia and regurgitation (13). In addition, patients who have the most important symptoms of GERD are not usually tested for extra-digestive manifestations. For these reasons it is believed that the prevalence of LPR in the population of patients with GERD has been underestimated (14).
A study in which 1,383 patients with GERD were interviewed determined that LPR increases as the severity of reflux increases (14) while another study has demonstrated that 24% of patients with reflux esophagitis had LPR (15). A third study included patients with chronic laryngitis that were divided into one group with GERD and one without GERD. After both groups had been treated with PPIs it was found that laryngeal symptoms and signs of laryngitis significantly improved only in the group with GERD (16).
LPR is a disease which has multi-factorial etiology in which determinant factors intervene. These factors include the functioning of the esophageal sphincters (lower esophageal sphincter in GERD and upper esophageal sphincter in LPR), tissue sensitivity and exposure time to gastric content (1, 17).
The larynx is at high risk from contact with the contents of the esophagus due to its near proximity to the digestive system. This is why it is logical to think that any reflux which passes above the upper esophageal sphincter can also affect the larynx. Even so, another mechanism has been described through which reflux produces laryngeal lesions without the necessity of direct contact with the larynx. It is the production of a vagal reflex produced by the acidification of the distal esophagus which produces coughing, throat clearing and laryngospasms (13,18).
EFFECTS ON THE LARYNX
The epithelium of the vocal folds is squamous, cylindrical and stratified. Connections by complexes of apical unions create a barrier mechanism against external and internal attacking agents including LPR (19).
In order to evaluate these barrier mechanisms of the epithelium, we have used transepithelial electrical resistance (TER) as an epithelial marker in the larynx and esophagus. TER measures the capacity of the tissue to act as a barrier by restricting the movement of solutes and solvents through the paracellular or transcellular route. Experimental studies have found that exposure of healthy vocal folds to acid and pepsin diminishes TER, thereby increasing the permeability of the epithelium and making it more susceptible to injury (19).
Other studies have demonstrated increased paracellular spaces in patients with LPR (20) and a noticeable diminution of E-Cadherin (transmembrane surface molecules that play a very important role in adhesion) in 37% of patients with LPR (21,22).
In addition, it has been found that patients with LPR have intracellular depletion of carbonic anhydrase III in the presence of pepsin. Carbonic anhydrase III is produced to stabilize cellular pH when the cell comes in contact with acid. It does so by generating a bicarbonate barrier. Diminution of carbonic anhydrase III results in a decrease in the protective response of the laryngeal tissue which is believed to play a very important role in alteration of the intercellular barrier associated with down-regulation of E-cadherin (22). It has also been found that that the Sep70 epithelial stress protein in squamous tissue, which provides epithelial protection, is also diminished in these patients (23).
A study by Aviv et al. has shown that another mechanism that seems to influence alterations in protection of the larynx is decreased sensitivity of the glottis caused by exposure to gastric content. This study found that LPR patients had decreased laryngeal adductory reflexes in response to administration of air pulses (24).
It is important to note that experimental clinical studies and animal studies have demonstrated that the larynx is more susceptible to injury from exposure to gastric contents than is the esophageal tissue. One study has demonstrated that only 3 episodes of LPR per week, with pH less than four, are required to produce changes in the laryngeal tissue while at least 50 episodes per week of GERD are required to produce some degree of injury in the esophagus (22,25).
In summary, all of these alterations in the cellular barrier and protective mechanisms of the larynx cause diminished epithelial resistance and increased susceptibility to future exposures to gastric content.
These epithelial alterations are believed to produce structural alterations in the larynx making reflux laryngitis, with or without granuloma formation, the main clinical manifestation of LPR. LPR has also been identified as the main cause of various other laryngeal pathologies including laryngeal stenosis, laryngeal nodules, polypoid degeneration, laryngomalacia, laryngospasm and paradoxical movement of vocal folds (1,26,27,28,29).
Reflux is also believed to be a factor which negatively affects healing of vocal folds, adversely affecting the results of laryngeal surgery. Two experimental studies on rabbits suggest that acid and pepsin significantly affect the healing of vocal folds (30) and that the healing of subglottic tissue is adversely affected by moderately acidic conditions (31).
Another study of 112 patients with LPR who underwent laryngeal surgery to treat Reinke's edema, vocal polyps or nodules was conducted by Kantas et al. Two groups were randomly selected: one received PPIs prior to and following surgery, the other group did not receive PPIs. The study found that LPR negatively affected re-epithelization and increased the recurrence of laryngeal injuries (32).
SYMPTOMS AND CLINICAL MANIFESTATIONS OF LARYNGOPHARINGEAL REFLUX
An excellent clinical history is indispensable for identification of this pathology. The patient should be asked about common reflux symptoms and symptoms related to head and neck pathologies, although it should be kept in mind the absence of these symptoms does not rule out this disease.
It is important to note that patients with LPR do not usually present classic clinical GERD manifestations as it has been demonstrated that many LPR patients do not have associated esophagitis or epigastralgia. Several studies have determined that LPR patients have an incidence of epigastralgia of less than 40% and an incidence of esophagitis of less than 25% (1,10,33,34).
Among the clinical manifestations of LPR are found a great variety of signs and symptoms of otolaryngeal diseases including dysphonia (71%), dry coughing (51%), throat clearing (42%), globus pharyngis (47%) and hypopharyngeal secretions. We also find dysphagia (35%), sensations of post-nasal drip (PND), bitter saliva, odynophagia and laryngeal spasms. In some cases coughing can become chronic with incapacitating coughing fits which wake the patient during the night (35).
As we can see, dysphonia is one of the main symptoms of LPR which is found in up to 50% of patients with voice alterations and/or laryngeal pathologies (36). Nevertheless, in children the clinical manifestations of this disease can be different from those in adults. Children can present recurrent episodes of tonsillitis, laryngitis and tracheitis, which occur as a consequence of abnormal exposition to acid in the upper respiratory tract. In these cases the presence of an acid pH generates inflammation which favors changes in the bacterial flora and recurrent infectious processes (37).
REFLUX SYMPTOMS INDEX
Indexes found in the literature can help us quantify reflux symptoms. Among them is the RSI (Reflux Symptoms Index). This is a chart with nine questions which aim to determine the severity of the symptoms related to LPR. This patient must fill out this questionnaire at the time of diagnosis and after treatment. Answers to questions are rankings from 0 to 5. Zero indicates "no problem", and five indicates "very troublesome." Since some degree of reflux is found in normal patients, an RSI greater than 13 is considered to be abnormal (38) (Table 1).
Table 1. Reflux Symptoms Index (RSI).
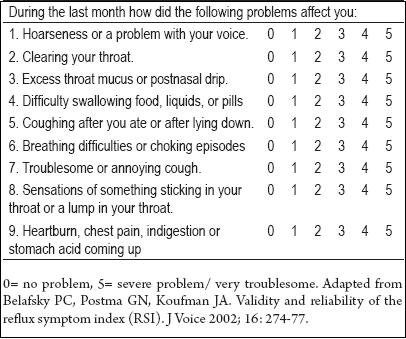
A study conducted by Belafsky et al. to validate the RSI scale evaluated 25 patients with LPR. Each patient's pH was monitored every 24 hours. Prior to beginning treatment, each patient completed the RSI twice: at the time of the first consultation and 8 days after. The patient answered the RSI questionnaire again after 6 months of treatment including twice daily doses of PPIs and other anti-reflux measures. The study found high reproducibility of pretreatment RSI results: 19.9 for the first RSI and 20.9 for the second (p <0.001).
The study included a control group of 25 additional patients of the same ages and genders as the LPR group who were found by using a database of patients who showed no evidence of LPR. The average pre-treatment RSI score for patients with LPR was significantly higher than that of controls (21.2 versus 11.6 p < 0.001). After six months of treatment the LPR groups average score dropped to 12.8, statistically similar to that of the asymptomatic group. Control group patients received no treatment since they were asymptomatic (38).
DIAGNOSIS
The basis for diagnosing this pathology is a combination of chronic or intermittent symptoms correlated with positive findings in the larynx. A complete clinical history with an exhaustive otolaryngological physical examination is necessary for identification of this disease. The physical examination must consider changes in the oral mucosa, hyperemia of the posterior pharyngeal wall, and lingual tonsils, whether or not patient's tongue is white, and laryngeal changes seen with indirect laryngoscopy (37).
The diagnostic algorithm that we currently use is to first identify symptoms suggestive of gastric reflux with extra-digestive manifestations, and then identify whether or not there are structural changes in the larynx or neighboring tissues. To make this identification we use a flexible Fiber Nasolaryngoscope, flexible Tele-laryngoscope and/or a laryngeal videostroboscope. The laryngeal videostroboscopy is a test that uses a strobe light which is synchronized closely to the frequency of vibration of the vocal folds. This allows us to appreciate what appear to be movements in slow motion of the process of vibration of the vocal folds. This examination is especially useful for identifying the alterations in the vibration pattern of the folds that produce laryngeal lesions.
Videolaryngoscopy and the laryngeal stroboscopy findings suggest LPR included pseudosulcus, thick secretions in the glottis, (Figure 1), irregular free edges, erythema and interarytenoid mucosal edema (Figure 2), posterior injuries such as ulcers and granuloma (65-74%) (Figure 3A and 3B), glottal and subglottic stenoses, and paradoxical movement of vocal folds (39,40). 90% of patients with LPR are found to have pseudosulcus and these patients are 2.5 more likely to have positive pH measurements (70% sensitivity, 77% specificity).

Figure 1. Telelaryngoscopy image of a patient with LPR symptoms showing increased and thickened secretions in the glottis with a heightened vascular pattern.

Figure 2. Telelaryngoscopy image of a patient with LPR symptoms showing noticeable edema of the free edge of the vocal folds with heightened vascular pattern as well as interarytenoid mucosa edema and erythema.
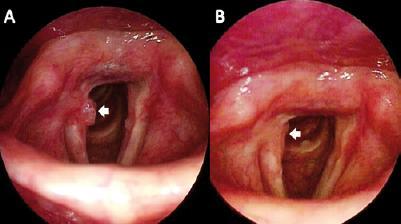
Figure 3. A Telelaryngoscopy image of a patient with LPR symptoms showing a granulomatous lesion in the posterior quarter of the free edge of the right vocal fold over the vocal process of the arytenoids. B Telelaryngoscopy image of the same patient 3 months after beginning PPI treatment and anti reflux control measures. Image shows that the granulomatous lesion in the posterior larynx has completely disappeared.
A study which interviewed 2,000 otolaryngologists revealed that the clinical signs most commonly used to diagnose reflux laryngitis are laryngeal erythema and edema (41). Nevertheless, these signs are not very specific, and it has been determined that many healthy adults can have these types of laryngeal alterations without association with any LPR symptoms (42).
An additional problem for diagnostic exactitude is the variability of diagnoses of extra-digestive reflux manifestations from one observer to another, and for one observer from one patient and/or one occasion to another. A study in which otolaryngologists evaluated laryngoscopy images of 120 patients showed low diagnostic reproducibility (43).
We refer patients who present additional digestive symptoms to gastroenterology for an upper digestive tract endoscopy. Nevertheless, some authors recommend performing an upper digestive tract endoscopy for all patients with manifestations of extra-digestive reflux to rule out important anatomical defects such as hiatal incompetence and hiatal hernia that may be related to the disease. Upper digestive tract endoscopies can also identify other lesions including esophagitis, esophageal stenosis, Barrett's esophagus, gastric mucosal injuries and tumors (37). LPR symptoms have also been shown to be more prevalent than typical GERD symptoms among patients with esophageal adenocarcinomas. These factors support the use of upper digestive tract endoscopy for the evaluation of these patients (44).
In addition to upper digestive tract endoscopies a battery of other diagnostic examinations can be used for selected cases in order to determine esophageal function, response to treatment and need for additional treatment. Among these is measurement of esophageal pH, esophageal gammagraphy, contrast x-rays of the upper digestive tract, manometry and esophageal impedanciometry.
Although the 24-hour esophageal pH test with an intragastric sensor is increasingly being used as a diagnostic tool for determining GERD and LPR, it cannot be considered the "gold standard" for diagnosing an extra-digestive syndrome because it does not reveal abnormal proximal events in a high percentage of patients with extra-digestive symptoms and typical signs. Nevertheless, it is useful for evaluating these patients' responses to treatment (45).
Due to the low specificity of laryngoscopy and the low sensitivity of the 24-hour esophageal pH test for determination of LPR, the therapeutic test has appeared as a diagnostic method which is now accepted in clinical practice. Currently, performance of a therapeutic test is recommended when the physician has clinical suspicion that a patient has LPR and when there is a positive finding for LPR from laryngoscopy (46). Therapeutic tests are not recommended for patients with gastrointestinal bleeding, anemia, abdominal pain and weight loss whose causes have not been completely studied since it is possible such patients have complex pathologies such as neoplasias (37).
CLASSIFICATION OF REFLUX FINDINGS
A subjective scale has been developed to quantify the severity of inflammatory changes in the larynx by identifying endoscopic findings related to LPR. This scale was created because LPR diagnoses based on patients' symptoms and on 24 hours pH measurements are very vague (47).
These subjective findings for patients with LPR are classified using the "Reflux Finding Score" (RFS) developed by Belafsky et al.(Table 2). The RFS gives a score related to laryngoscopic findings. The maximum score is 26; a score of 7 or greater is considered to indicate that LPR is highly likely. This scale has been standardized so that otolaryngologists can perform better diagnoses, document the severity of symptoms and evaluate the effectiveness of treatment (48).
Table 2. "Reflux Finding Score" (RFS).
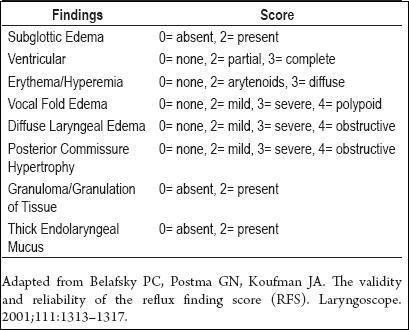
Of the findings mentioned in Table 2, erythema, arytenoid hyperemia and vocal fold edema respond to medical treatment for reflux (49). Other studies confirm that vocal fold edema and erythema and the inter-arytenoid space are sensitive markers for LPR (50).
A study of the validity of the RFS compared a group of 40 patients who had cases of LPR confirmed by pH measurements before treatment, and who were then tested at two, four and six months following treatment, with a control group of 40 patients with healthy larynxes. The study found that the average RFS for healthy patients was 5.2 whereas the average RFS for patients with LPR was 11.5. On the basis of this study the authors consider that this index is reproducible, reliable and appropriate for documenting the effectiveness of treatment of LPR patients. They conclude that it is a useful tool for describing changes in laryngeal tissues caused by this disease (50).
TREATMENT
Current recommendations try to limit indiscriminate empirical use of anti reflux medications for treatment of patients with dysphonia, especially when patients have no GERD symptoms or laryngeal disorders caused by reflux. This is because of the known adverse effects of these drugs and lack of evidence that they benefit patients with dysphonia. Medical management must be directed at controlling inflammatory changes of the larynx when it is documented through laryngoscopic findings of erythema, edema, redundant tissue, irregularities in the interarytenoid, arytenoid, or posterior laryngeal mucosa or findings of irregularities in the vocal folds (51).
In patients with clinical symptoms of reflux disease with extra digestive manifestations, the first step in treatment consists of diet modifications and anti-reflux measures. Diet modifications include weight loss when necessary, and avoidance of exaggerated consumption of alcoholic beverages, coffee, chocolate, menthol, citrus fruit, citrus juices, condiments and spicy food. Anti-reflux measures include raising the head of the bed, left lateral decubitus position at bedtime, avoidance of naps after eating, avoidance of sleep until at least three hours after the last meal of the day, avoidance of abdominal exercises after eating, and avoidance of the use corsets, belts and tight clothing. Research done by Stewart et al. showed that changes in lifestyle for 2 months, with or without medical management with PPIs, considerably improves chronic laryngeal symptoms (52).
As previously mentioned, many recent guidelines for management of manifestations of extra digestive reflux, including the most recent official guidelines of the Asociación Colombiana de Otorrinolaringología (ACORL - Colombian Association of Otolaryngology), recommend performance of a therapeutic test with PPI for patients with symptoms suggestive of laryngopharyngeal reflux (LPR) and who have laryngoscopy findings which are positive for LPR (53, 54). The idea of this test is to determine the influence of reflux on the patient's symptoms. The test consists of PPI dose twice a day, once at least 30 minutes before breakfast, and again at least 30 minutes before dinner. The treatment must be followed for 2 to 3 months without changes in the same dosages until the patient is evaluated again. It has been determined that patients with laryngopharyngeal reflux require a more aggressive and prolonged treatment than do patients with gastroesophageal reflux (1). With medical management lasting 2 or 3 months, most patients' symptoms improve significantly; however laryngeal changes require at least 6 months before they are resolved (39).
If the patient responds adequately to treatment during the test, treatment with progressively decreasing does should be maintained for 6 additional months. If the patient's symptoms persist, two clinical situations are possible. The patient may simply haves an inadequate response to the treatment, but the possibility also exists that the cause of the symptoms is not reflux (37). In the case, PPI dosage can be doubled, the PPI can be changed, or Ranitidine or associate alginates can be added to the treatment. In the second case, the study of the patient must be completed with 24 hour pH measurement with an intragastric sensor without suspending the medication to evaluate whether PPIs are effectively suppressing acid secretion, and the patient must be examined by a gastroenterologist.
Alginates are currently used as an option for GERD treatment and are beginning to be used for laryngopharyngeal reflux (LPR). These alginates create a physical barrier to gastric content and protect the esophageal mucosa from acid reflux. McGlashan et al. studied 49 LPR patients who were divided into a group which was provided with a suspension of alginate and a group which was given placebos. A statistically significant decrease of symptoms was found among the patients who received alginates (12).
Today there are also other tools available for evaluation of the presence of non acid reflux as a cause of the symptoms, esophageal motility and gastric emptying. These include esophageal manometry, esophageal impedance, adding prokinetics when emptying disorders are suspected and the possibility of anti reflux surgery.
Not all patients whose medical management has failed are candidates for surgical management. The best candidates are those who react properly to anti-secretory therapy. Candidates for surgery should have anatomical defects such as large hiatal hernias affecting the motility of the normal upper gastrointestinal tract which need to be corrected. Candidates also include those patients whose reflux persists in the hypopharynx despite maximum doses of PPIs, those who have abundant reflux material, and those with duodenum-gastric reflux or reflux complications (37,54).
CONCLUSIONS
Reflux laryngitis or laryngopharyngeal reflux is one of the extra-digestive manifestations of gastroesophageal reflux. It has become one of the most frequent reasons that patients consult otolaryngologists. However, it has been over-diagnosed by attribution of reflux to several clinical manifestations that are not always related.
LPR is considered to be a different clinical entity than GERD because it presents different symptoms, clinical manifestations and treatment objectives. Although several studies have demonstrated that reflux is associated with the development of different laryngeal pathologies, the controversy about their pathophysiology, diagnosis and treatment persists.
The otolaryngologist must recognize extra-digestive manifestations of reflux for which patients initially consult, and consequently must have the capacity to identify this disease and to lead in its diagnosis and treatment together with the gastroenterologist.
REFERENCES
1. Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the Committee on Speech, Voice, and Swallowing Disorders of the American Academy of OtolaryngologyHead Neck Surgery. Otolaryngol Head Neck Surg 2002; 127: 32-35.
2. Payne RJ, Kost KM, Frenkiel S, Zeitouni AG, Sejean G, Sweet RC, Naor N, Hernández L, Kimoff RJ. Laryngeal inflammation assessed using the reflux finding score in obstructive sleep apnea. Otolaryngol Head Neck Surg 2006; 134(5): 836-42.
3. Pasic TR, Palazzi-Churas KL, Connor NP, Cohen SB, Leverson GE. Association of extraesophageal reflux disease and sinonasal symptoms: prevalence and impact on quality of life. Laryngoscope 2007; 117(12): 2218-28.
4. Parsons JP, Mastronarde JG. Gastroesophageal reflux disease and asthma. Curr Opin Pulm Med 2010; 16(1): 60-3.
5. DelGaudio JM, Naseri I, Wise JC. Proximal pharyngeal reflux correlates with increasing severity of lingual tonsil hypertrophy. Otolaryngol Head Neck Surg 2008; 138(4): 473-8.
6. Sone M, Yamamuro Y, Hayashi H, Niwa Y, Nakashima T. Otitis media in adults as a symptom of gastroesophageal reflux. Otolaryngol Head Neck Surg 2007; 136(1): 19-22.
7. Crapko M, Kerschner JE, Syring M, Johnston N. Role of extra-esophageal reflux in chronic otitis media with effusion. Laryngoscope 2007; 117(8): 1419-23.
8. Al-Saab F, Manoukian JJ, Al-Sabah B, Almot S, Nguyen LH, Tewfik TL, Daniel SJ, Schloss MD, Hamid QA. Linking laryngopharyngeal reflux to otitis media with effusion: pepsinogen study of adenoid tissue and middle ear fluid. J Otolaryngol Head Neck Surg 2008; 37(4): 565-71
9. Gupta R, Sataloff RT. Laryngopharyngeal reflux: current concepts and questions. Curr Opin Otolaryngol Head Neck Surg 2009; 17(3): 143-8.
10. Koufman JA. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope 1991; 101(4 Pt 2 Suppl 53): 1-78. Review.
11. Altman KW, Stephens RM, Lyttle SC, Weiss KB. Changing impact of gastroesophageal reflux in medical and otolaryngology practice. Laryngoscope 2005; 115: 1145-1153.
12. Merati AL. Reflux and cough. Otolaryngol Clin North Am 2010; 43(1): 97-110.
13. Poelmans J, Feenstra L, Demedts I, et al. The yield of upper gastrointestinal endoscopy in patients with suspected reflux-related chronic ear, nose and throat symptoms. Am J Gastroenterol 2004; 99: 1419-1426.
14. Groome M, Cotton JP, Borland M, McLeod S, Johnston DA, Dillon JF. Prevalence of laryngopharyngeal reflux in a population with gastroesophageal reflux. Laryngoscope 2007; 117(8): 1424-8.
15. Lai YC, Wang PC, Lin JC. Laryngopharyngeal reflux in patients with reflux esophagitis. World J Gastroenterol 2008; 14: 4523-4528.
16. Qua CS, Wong CH, Gopala K, Goh KL. Gastro-oesophageal reflux disease in chronic laryngitis: prevalence and response to acid-suppressive therapy. Aliment Pharmacol Ther 2007; 25: 287-295.
17. Cohen SM, Garrett CG. Hoarseness: is it really laryngopharyngeal reflux? Laryngoscope 2008; 118(2): 363-6.
18. Shaker R, Dodds WJ, Ren J, et al. Esophagoglottal closure reflex: a mechanism of airway protection. Gastroenterology 1992; 102(3): 857-61.
19. Erickson E, Sivasankar M. Simulated reflux decreases vocal fold epithelial barrier resistance. Laryngoscope 2010; 120(8): 1569-75.
20. Franchi A, Brogelli B, Massi D, Santucci M, De Campora E, Gallo O. Dilation of intercellular spaces is associated with laryngopharyngeal reflux: an ultrastructural morphometric analysis of laryngeal epithelium. Eur Arch Otorhinolaryngol 2007; 264: 907-911.
21. Johnston N, Bulmer D, Gill GA, et al. Cell biology of laryngeal epithelial defenses in health and disease: further studies. Ann Otol Rhinol Laryngol 2003; 112: 481-491.
22. Gill G, Johnston N, Buda A, et al. Laryngeal epithelial defenses against laryngopharyngeal reflux: investigations of E-cadherin, carbonic anhydrase isoenzyme III, and pepsin. Ann Otol Rhinol Laryngol 2005; 114: 913-921.
23. Johnston N, Dettmar PW, Lively MO, Postma GN, Belafsky PC, Birchall M, Koufman JA. Effect of pepsin on laryngeal stress protein (Sep70, Sep53, and Hsp70) response: role in laryngopharyngeal reflux disease. Ann Otol Rhinol Laryngol 2006; 115(1): 47-58.
24. Aviv JE, Liu H, Parides M, et al. Laryngopharyngeal sensory deficits in patients with laryngopharyngeal reflux and dysphagia. Ann Otol Rhinol Laryngol 2000; 109: 1000- 1006.
25. Ylitalo R, Lindestad P, Ramel S. Symptoms, laryngeal findings, and 24-hour pH monitoring in patients with suspected gastroesophago-pharyngeal reflux. Laryngoscope 2001; 111: 1735-41.
26. Maronian NC, Azadeh H, Waugh P, Hillel A. Association of laryngopharyngeal reflux disease and subglottic stenosis. Ann Otol Rhinol Laryngol 2001; 110(7 Pt 1): 606-12.
27. Kuhn J, Toohill RJ, Ulualp SO, et al. Pharyngeal acid reflux events in patients with vocal cord nodules. Laryngoscope 1998; 108: 1146-9.
28. Manning SC, Inglis AF, Mouzakes J, et al. Laryngeal anatomic differences in pediatric patients with severe laryngomalacia. Arch Otolaryngol Head Neck Surg 2005; 131: 340-343.
29. Maschka DA, Bauman NM, McCray Jr PB, et al. A classification scheme for paradoxical vocal cord motion. Laryngoscope 1997; 107: 1429-1435.
30. Roh JL, Yoon YH. Effect of acid and pepsin on glottic wound healing: a simulated reflux model. Arch Otolaryngol Head Neck Surg 2006; 132(9): 995-1000.
31. Roh JL, Lee YW, Park HT. Effect of acid, pepsin, and bile acid on the stenotic progression of traumatized subglottis. Am J Gastroenterol 2006; 101(6): 1186-92.
32. Kantas I, Balatsouras DG, Kamargianis N, et al. The influence of laryngopharyngeal reflux in the healing of laryngeal trauma. Eur Arch Otorhinolaryngol 2009; 266: 253-259.
33. Wiener GJ, Koufman JA, Wu WC, et al. Chronic hoarseness secondary to gastroesophageal reflux disease: documentation with 24-h ambulatory pH monitoring. Am J Gastroenterol 1989; 84: 1503-8.
34. Belafsky PC, Postma GN, Koufman JA. Transnasal esophagoscopy (TNE). Otolaryngol Head Neck Surg 2001; 125: 588-9.
35. Koufman JA, Amin MR, Panetti M. The prevalence of reflux in 113 consecutive patients with laryngeal and voice disorders. Otolaryngol Head Neck Surg 2000; 123: 385-388.
36. Belafsky PC, Postma GN, Koufman JA. Laryngopharyngeal reflux symptoms improve before changes in physical findings. Laryngoscope 2001; 111: 979-981.
37. Campos G, Enfermedad por reflujo gástrico con manifestaciones extradigestivas, Manual de Otorrinolaringología, cabeza y cuello, 2007.
38. Belafsky PC, Postma GN, Koufman JA. Validity and reliability of the reflux sympton index (RSI). J Voice 2002; 16: 274-77.
39. Belasky PC, Postma GN, Koufman JA, Laryngopharyngeal reflux symptoms improve before changes in physical findings. Laryngoscope 2001; 111: 979-81.
40. Vaezi MF, Gastroesophageal Reflux Disease and the Larynx, J Clin Gastroenterol 2003; 36(3): 198-203.
41. Ahmed TF, Khandwala F, Abelson TI, et al. Chronic laryngitis associated with gastroesophageal reflux: prospective assessment of differences in practice patterns between gastroenterologists and ENT physicians. Am J Gastroenterol 2006, 101: 470- 478.
42. Hicks DM, Ours TM, Abelson TI, et al. The prevalence of hypopharynx findings associated with gastroesophageal reflux in normal volunteers. J Voice 2002; 16: 564- 579.
43. As Branski RC, Bhattacharyya N, Shapiro J. The reliability of the assessment of endoscopic laryngeal findings associated with laryngopharyngeal reflux disease. Laryngoscope 2002; 112: 1019-1024.
44. Reavis KM, Morris CD, Gopal DV, Hunter JG, Jobe BA. Laryngopharyngeal reflux symptoms better predict the presence of esophageal adenocarcinoma than typical gastroesophageal reflux symptoms. Ann Surg 2004; 239(6): 849-56.
45. Vaezi MF, Gastroesophageal Reflux Disease and the Larynx, J Clin Gastroenterol 2003; 36(3): 198-203.
46. Vaezi MF. Laryngeal manifestations of gastroesophageal reflux disease. Curr Gastroenterol Rep 2008; 10(3): 271-7.
47. Peter C. Belafsky, MD, PhD. Abnormal Endoscopic Pharyngeal and Laryngeal Findings Attributable to Reflux. Am J Med 2003; 115(3A): 90S-96S.
48. Joiniau S, Bradshaw A, Esterman A, et al. Reflux and laringitis; a systematic review. Otolaryngol Head and Neck Surg 2007; 136: 686-692.
49. Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS). Laryngoscope 2001; 111: 1313-1317.
50. Pribuisiene R, Uloza V, Kupcinskas L. Diagnostic sensitivity and specificity of laryngoscopic sings and reflux laringitis. Medicina 2006; 44: 280-287.
51. Schwartz SR, Cohen SM, Dailey SH, Rosenfeld RM, et al. Clinical practice guideline: hoarseness (dysphonia). Otolaryngol Head Neck Surg 2009; 141(3 Suppl 2): S1-S31.
52. Steward DL, Wilson KM, Kelly DH, et al. Proton pump inhibitor therapy for chronic laryngo-pharyngitis: a randomized placebo-control trial. Otolaryngol Head Neck Surg 2004; 131: 342-350.
53. Guías oficiales de la ACORL para las enfermedades más prevalentes en otorrinolanrigología. Laringitis crónica por reflujo. 2007.
54. Bove, M., Rosen C. Diagnosis and management of laryngopharyngeal reflux. Current opinion in Otolaryngology & Hean Necks Surgery 2006; 14: 116-123.
1. Koufman JA, Aviv JE, Casiano RR, Shaw GY. Laryngopharyngeal reflux: position statement of the Committee on Speech, Voice, and Swallowing Disorders of the American Academy of Otolaryngology–Head Neck Surgery. Otolaryngol Head Neck Surg 2002; 127: 32-35. [ Links ]
2. Payne RJ, Kost KM, Frenkiel S, Zeitouni AG, Sejean G, Sweet RC, Naor N, Hernández L, Kimoff RJ. Laryngeal inflammation assessed using the reflux finding score in obstructive sleep apnea. Otolaryngol Head Neck Surg 2006; 134(5): 836-42. [ Links ]
3. Pasic TR, Palazzi-Churas KL, Connor NP, Cohen SB, Leverson GE. Association of extraesophageal reflux disease and sinonasal symptoms: prevalence and impact on quality of life. Laryngoscope 2007; 117(12): 2218-28. [ Links ]
4. Parsons JP, Mastronarde JG. Gastroesophageal reflux disease and asthma. Curr Opin Pulm Med 2010; 16(1): 60-3. [ Links ]
5. DelGaudio JM, Naseri I, Wise JC. Proximal pharyngeal reflux correlates with increasing severity of lingual tonsil hypertrophy. Otolaryngol Head Neck Surg 2008; 138(4): 473-8. [ Links ]
6. Sone M, Yamamuro Y, Hayashi H, Niwa Y, Nakashima T. Otitis media in adults as a symptom of gastroesophageal reflux. Otolaryngol Head Neck Surg 2007; 136(1): 19-22. [ Links ]
7. Crapko M, Kerschner JE, Syring M, Johnston N. Role of extra-esophageal reflux in chronic otitis media with effusion. Laryngoscope 2007; 117(8): 1419-23. [ Links ]
8. Al-Saab F, Manoukian JJ, Al-Sabah B, Almot S, Nguyen LH, Tewfik TL, Daniel SJ, Schloss MD, Hamid QA. Linking laryngopharyngeal reflux to otitis media with effusion: pepsinogen study of adenoid tissue and middle ear fluid. J Otolaryngol Head Neck Surg 2008; 37(4): 565-71. [ Links ]
9. Gupta R, Sataloff RT. Laryngopharyngeal reflux: current concepts and questions. Curr Opin Otolaryngol Head Neck Surg 2009; 17(3): 143-8. [ Links ]
10. Koufman JA. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): a clinical investigation of 225 patients using ambulatory 24-hour pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope 1991; 101(4 Pt 2 Suppl 53): 1-78. Review. [ Links ]
11. Altman KW, Stephens RM, Lyttle SC, Weiss KB. Changing impact of gastroesophageal reflux in medical and otolaryngology practice. Laryngoscope 2005; 115: 1145-1153. [ Links ]
12. Merati AL. Reflux and cough. Otolaryngol Clin North Am 2010; 43(1): 97-110. [ Links ]
13. Poelmans J, Feenstra L, Demedts I, et al. The yield of upper gastrointestinal endoscopy in patients with suspected reflux-related chronic ear, nose and throat symptoms. Am J Gastroenterol 2004; 99: 1419-1426. [ Links ]
14. Groome M, Cotton JP, Borland M, McLeod S, Johnston DA, Dillon JF. Prevalence of laryngopharyngeal reflux in a population with gastroesophageal reflux. Laryngoscope 2007; 117(8): 1424-8. [ Links ]
15. Lai YC, Wang PC, Lin JC. Laryngopharyngeal reflux in patients with reflux esophagitis. World J Gastroenterol 2008; 14: 4523-4528. [ Links ]
16. Qua CS, Wong CH, Gopala K, Goh KL. Gastro-oesophageal reflux disease in chronic laryngitis: prevalence and response to acid-suppressive therapy. Aliment Pharmacol Ther 2007; 25: 287-295. [ Links ]
17. Cohen SM, Garrett CG. Hoarseness: is it really laryngopharyngeal reflux? Laryngoscope 2008; 118(2): 363-6. [ Links ]
18. Shaker R, Dodds WJ, Ren J, et al. Esophagoglottal closure reflex: a mechanism of airway protection. Gastroenterology 1992; 102(3): 857-61. [ Links ]
19. Erickson E, Sivasankar M. Simulated reflux decreases vocal fold epithelial barrier resistance. Laryngoscope 2010; 120(8): 1569-75. [ Links ]
20. Franchi A, Brogelli B, Massi D, Santucci M, De Campora E, Gallo O. Dilation of intercellular spaces is associated with laryngopharyngeal reflux: an ultrastructural morphometric analysis of laryngeal epithelium. Eur Arch Otorhinolaryngol 2007; 264: 907-911. [ Links ]
21. Johnston N, Bulmer D, Gill GA, et al. Cell biology of laryngeal epithelial defenses in health and disease: further studies. Ann Otol Rhinol Laryngol 2003; 112: 481-491. [ Links ]
22. Gill G, Johnston N, Buda A, et al. Laryngeal epithelial defenses against laryngopharyngeal reflux: investigations of E-cadherin, carbonic anhydrase isoenzyme III, and pepsin. Ann Otol Rhinol Laryngol 2005; 114: 913-921. [ Links ]
23. Johnston N, Dettmar PW, Lively MO, Postma GN, Belafsky PC, Birchall M, Koufman JA. Effect of pepsin on laryngeal stress protein (Sep70, Sep53, and Hsp70) response: role in laryngopharyngeal reflux disease. Ann Otol Rhinol Laryngol 2006; 115(1): 47-58. [ Links ]
24. Aviv JE, Liu H, Parides M, et al. Laryngopharyngeal sensory deficits in patients with laryngopharyngeal reflux and dysphagia. Ann Otol Rhinol Laryngol 2000; 109: 1000- 1006. [ Links ]
25. Ylitalo R, Lindestad P, Ramel S. Symptoms, laryngeal findings, and 24-hour pH monitoring in patients with suspected gastroesophago-pharyngeal reflux. Laryngoscope 2001; 111: 1735-41. [ Links ]
26. Maronian NC, Azadeh H, Waugh P, Hillel A. Association of laryngopharyngeal reflux disease and subglottic stenosis. Ann Otol Rhinol Laryngol 2001; 110(7 Pt 1): 606-12. [ Links ]
27. Kuhn J, Toohill RJ, Ulualp SO, et al. Pharyngeal acid reflux events in patients with vocal cord nodules. Laryngoscope 1998; 108: 1146-9. [ Links ]
28. Manning SC, Inglis AF, Mouzakes J, et al. Laryngeal anatomic differences in pediatric patients with severe laryngomalacia. Arch Otolaryngol Head Neck Surg 2005; 131: 340-343. [ Links ]
29. Maschka DA, Bauman NM, McCray Jr PB, et al. A classification scheme for paradoxical vocal cord motion. Laryngoscope 1997; 107: 1429-1435. [ Links ]
30. Roh JL, Yoon YH. Effect of acid and pepsin on glottic wound healing: a simulated reflux model. Arch Otolaryngol Head Neck Surg 2006; 132(9): 995-1000. [ Links ]
31. Roh JL, Lee YW, Park HT. Effect of acid, pepsin, and bile acid on the stenotic progression of traumatized subglottis. Am J Gastroenterol 2006; 101(6): 1186-92. [ Links ]
32. Kantas I, Balatsouras DG, Kamargianis N, et al. The influence of laryngopharyngeal reflux in the healing of laryngeal trauma. Eur Arch Otorhinolaryngol 2009; 266: 253-259. [ Links ]
33. Wiener GJ, Koufman JA, Wu WC, et al. Chronic hoarseness secondary to gastroesophageal reflux disease: documentation with 24-h ambulatory pH monitoring. Am J Gastroenterol 1989; 84: 1503-8. [ Links ]
34. Belafsky PC, Postma GN, Koufman JA. Transnasal esophagoscopy (TNE). Otolaryngol Head Neck Surg 2001; 125: 588-9. [ Links ]
35. Koufman JA, Amin MR, Panetti M. The prevalence of reflux in 113 consecutive patients with laryngeal and voice disorders. Otolaryngol Head Neck Surg 2000; 123: 385-388. [ Links ]
36. Belafsky PC, Postma GN, Koufman JA. Laryngopharyngeal reflux symptoms improve before changes in physical findings. Laryngoscope 2001; 111: 979-981. [ Links ]
37. Campos G, Enfermedad por reflujo gástrico con manifestaciones extradigestivas, Manual de Otorrinolaringología, cabeza y cuello, 2007. [ Links ]
38. Belafsky PC, Postma GN, Koufman JA. Validity and reliability of the reflux sympton index (RSI). J Voice 2002; 16: 274-77. [ Links ]
39. Belasky PC, Postma GN, Koufman JA, Laryngopharyngeal reflux symptoms improve before changes in physical findings. Laryngoscope 2001; 111: 979-81. [ Links ]
40. Vaezi MF, Gastroesophageal Reflux Disease and the Larynx, J Clin Gastroenterol 2003; 36(3): 198-203. [ Links ]
41. Ahmed TF, Khandwala F, Abelson TI, et al. Chronic laryngitis associated with gastroesophageal reflux: prospective assessment of differences in practice patterns between gastroenterologists and ENT physicians. Am J Gastroenterol 2006, 101: 470- 478. [ Links ]
42. Hicks DM, Ours TM, Abelson TI, et al. The prevalence of hypopharynx findings associated with gastroesophageal reflux in normal volunteers. J Voice 2002; 16: 564- 579. [ Links ]
43. As Branski RC, Bhattacharyya N, Shapiro J. The reliability of the assessment of endoscopic laryngeal findings associated with laryngopharyngeal reflux disease. Laryngoscope 2002; 112: 1019-1024. [ Links ]
44. Reavis KM, Morris CD, Gopal DV, Hunter JG, Jobe BA. Laryngopharyngeal reflux symptoms better predict the presence of esophageal adenocarcinoma than typical gastroesophageal reflux symptoms. Ann Surg 2004; 239(6): 849-56. [ Links ]
45. Vaezi MF, Gastroesophageal Reflux Disease and the Larynx, J Clin Gastroenterol 2003; 36(3): 198-203. [ Links ]
46. Vaezi MF. Laryngeal manifestations of gastroesophageal reflux disease. Curr Gastroenterol Rep 2008; 10(3): 271-7. [ Links ]
47. Peter C. Belafsky, MD, PhD. Abnormal Endoscopic Pharyngeal and Laryngeal Findings Attributable to Reflux. Am J Med 2003; 115(3A): 90S-96S. [ Links ]
48. Joiniau S, Bradshaw A, Esterman A, et al. Reflux and laringitis; a systematic review. Otolaryngol Head and Neck Surg 2007; 136: 686-692. [ Links ]
49. Belafsky PC, Postma GN, Koufman JA. The validity and reliability of the reflux finding score (RFS). Laryngoscope 2001; 111: 1313-1317. [ Links ]
50. Pribuisiene R, Uloza V, Kupcinskas L. Diagnostic sensitivity and specificity of laryngoscopic sings and reflux laringitis. Medicina 2006; 44: 280-287. [ Links ]
51. Schwartz SR, Cohen SM, Dailey SH, Rosenfeld RM, et al. Clinical practice guideline: hoarseness (dysphonia). Otolaryngol Head Neck Surg 2009; 141(3 Suppl 2): S1-S31. [ Links ]
52. Steward DL, Wilson KM, Kelly DH, et al. Proton pump inhibitor therapy for chronic laryngo-pharyngitis: a randomized placebo-control trial. Otolaryngol Head Neck Surg 2004; 131: 342-350. [ Links ]
53. Guías oficiales de la ACORL para las enfermedades más prevalentes en otorrinolanrigología. Laringitis crónica por reflujo. 2007. [ Links ]
54. Bove, M., Rosen C. Diagnosis and management of laryngopharyngeal reflux. Current opinion in Otolaryngology & Hean Necks Surgery 2006; 14: 116-123. [ Links ]

