










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.3 Bogotá Sept. 2011
Most frequently asked questions about pregnancy and hepatitis B
Carmen Yanette Suárez Quintero, MD (1)
(1) Gastroenterologist and Hepatologist at the Hospital Universitario de San Ignacio in Bogotá, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 30-08-11 Accepted: 15-09-11
Abstract
Currently there are an estimated 350 million people in the world who have chronic hepatitis B infections. In areas where the disease is endemic such as Asia, Sub-Saharan Africa and the Amazon region, the infection is most often acquired in the prenatal period or in early childhood. This is in turn related to the high prevalence of Hepatitis B e-Antigen (HBeAg) (40% to 50%) found among women of reproductive age (1-4).
Key words
Pregnancy, hepatitis B, transmission
Prevention of vertical transmission of HBV infections is very important because infection at an early age has a high probability of becoming chronic and because severe complications such as cirrhosis and liver cancer are also likely to appear very early. Unfortunately HBV testing, assessment and monitoring before and during pregnancy is not done in many areas. This is due partly to lack of resources, but also to the difficulty accessing health care services in some remote areas and to simple lack of knowledge about the disease.
Below I discuss a typical case report of a pregnant woman who is infected with HBV.
A 26 year old patient had her first pregnancy check-up in her fourth month of pregnancy. The patients HBsAg (HBV surface antigen) test value was reported as 358. For this reason the doctor requested that her husband also be given the HBsAg test to understand the evolutionary state of the infection. In addition HBeAg (HBV e antigen) and viral load tests were requested. The husband had been vaccinated against HBV and tested negative. The patient was diagnosed as having chronic HBV without cirrhosis or portal hypertension. Her transaminase level was less than 2 times the normal level, she was positive for HBeAg, and had a viral load of 350,000 IU/ml. The doctor informed the patient of the diagnosis, and she in turn asked the following questions:
1. How is the HBV transmitted to the child and what is the probability that this could happen?
Transmission can occur in utero or at birth. In utero transmission is very rare except in the context of acute HBV in the third trimester of pregnancy and when HBV is present in the placenta (especially in hairy endothelial capillary cells). Thus, most of the time transmission occurs during delivery. Nevertheless, cesarean sections do not prevent mother to child transmission (5-7). HBeAg positive mothers have a risk of transmitting the virus ranging from 70% to 90% at 6 months plus a 90% probability that the baby will be chronically infected. Mothers who are HBeAg negative have risks of transmission ranging from 10% to 40 %, with a probability of 40% to 70% of the baby being chronically infected. Viral load greater than 8 to 10 copies during pregnancy is another risk factor, not only for maternal-fetal transmission, but also for poor response to vaccine, intrauterine infection and HBV mutation (8, 9).
2. Can anything be done to prevent HBV transmission to the child?
Yes. Treatment includes administration of 100 IU HIBg (HBV immune globulin) and HBV vaccine to the child in the first 12 hours after birth followed by boosters at 4 weeks and 6 months of age. The infection may persist in five to ten percent of children of mothers who are HBeAg (+) and in one to three percent of children of mothers who are HBeAg (-). Nevertheless, between one and two percent of children who are treated may not develop immunity later (10).
3. Should an expecting mother who has a HBV infection use any antiviral drugs or take any other treatment during pregnancy?
Because viremia levels are a major factor in determination of the possibility of immunoprophylaxis in the newborn as well as in potential, prenatal treatment is extremely important for pregnant women with high viral load greater than 8 to 10 copies. Treatment with antiviral drugs beginning at 34 weeks of pregnancy has been shown to achieve a sufficient reduction of viral loads which is important in case of an early delivery.
There are 6 antiviral drugs approved for the treatment of chronic hepatitis B: Adefovir dipidoxil (category C of drug safety in pregnancy), interferon (category C), entecavir (category C), lamivudine (category C), tenofovir (category B), and telbivudine (category B). Of these lamivudine has been best studied and also has been studied for treatment of HIV. Safe lamivudine dosage has been determined to be 150 mg every 12 hours (11-13).
4. Are there any adverse effects from the use of antiviral drugs during pregnancy?
There are reports of lactic acidosis and hepatic steatosis in pregnant women receiving these analogs, so it is important to monitor liver enzymes and serum electrolytes when a patient receives this type of medication during pregnancy (12).
5. What kind of follow-up treatment should be done after delivery?
As mentioned, the vaccine and HIBg should be given. After completing the vaccine series, anti-HBs and HBsAg should be administered between 9 and 18 months of age. Children with negative HBsAg and anti-HBsAg greater than 10 mIU / mL will be protected and should not require future medical treatment. However, children with lower levels of anti-HBsAg will not be adequately protected and should be revaccinated with another three dose series and retested one or two months after the final dose. Children who test HBsAg positive should be considered infected and should be treated as such (14).
6. Can chronic HBV by itself have any impact on delivery?
There is evidence chronic HBV increases morbidity rates for conditions such as fetal distress, preterm labor and meconium peritonitis among mothers and newborns. There have also been observations of increased incidences of gestational diabetes, pre-partum hemorrhaging and preterm labor among mothers with chronic Hepatitis B (15, 16).
7. What is the impact of chronic HBV on pregnancy?
Pregnancy is well tolerated by healthy women although there is an increase in the production of hormones with immunosuppressive effects such as corticosteroids, estrogens and progesterone. On the other hand it has also been observed that one third of women have decreased viral load levels with HBeAg seroconversion occurring among 17% of these women one or two months after delivery (17, 18).
8. Should breast feeding by women with chronic HBV be prohibited?
In the 1970s and 1980s various groups reported HBV transmission from breast milk, but in 1975 Beasley and colleagues compared breast milk with formula milk. They reported 53% of the children of mothers with HBsAg who received breast milk tested positive for HBsAg, but that 60% of the children of mothers with HBsAg who received prepared formulas also tested positive. They concluded that HBV had not been transmitted by breast milk to children who had tested positive for HBsAg (19).
CONCLUSIONS
Although not all physiopathological mechanisms involved in the transmission of HBV from mother to child are exactly known, we now know much more than a few years ago. This forces us to study each particular case in order to provide the best advice for each situation so that each mother's labor can be successful and so that the presence of HBV can be prevented in the child. Finally, following suggestions found in the literature, we propose what could be the algorithm for management of HBV infection during pregnancy (figure 1).
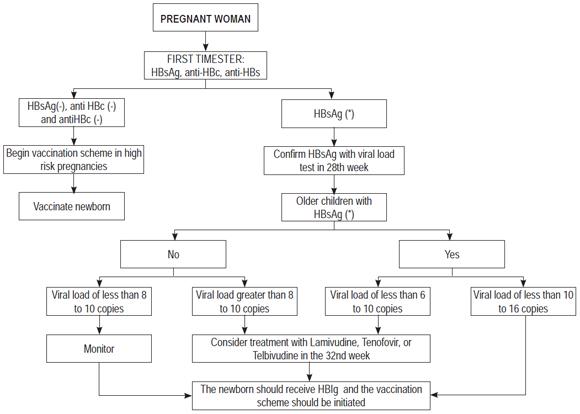
Figure 1. Flow chart for managing HBV infections in pregnant women and newborns.
REFERENCES
1. Lok AS. Chronic hepatitis B. N Engl J Med 2002; 346(22): 1682-3.
2. Yao JL. Perinatal transmission of hepatitis B virus infection and vaccination in China. Gut 1996; 38: s37-38.
3. Euler G. Hepatitis B surface antigen prevalence among pregnant women in urban areas: implications for testing, reporting and preventing perinatal transmission. Pediatrics 2003; 111: 1192-97.
4. Gupta I. Immunogenicity and safety of two schedules of hepatitis B vaccination during pregnancy. J Obstet Gynaecol Res 2003; 29(2): 84-6.
5. Okada K. Antigen and anti-e in the serum of asymptomatic carrier mothers as indicators of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med 1976; 294(14): 746-49.
6. Guntupalli SR. Hepatic diseases and pregnancy: an overview of diagnosis and management. Crit Care Med 2005; 33(10): S332-9.
7. Xu DZ. Risk factors and mechanism of transplacental transmission of hepatitis B virus. J Med Virol 2002; 67(1): 20-6.
8. Su G. Efficacy and safety of lamivudine treatment or chronic hepatitis B in pregnancy. World Gastroentrol 2004; 10(6): 910-12.
9. Tang JR. Hepatitis B surface antigenemia at birth: a long term follow-up study. J Pediatr 1998; 133(3): 374-7.
10. Tran TT. Management of the pregnant hepatitis B patient. Curr Hepat Rep 2008; 2: 43-48.
11. Van Zonneveld M. Lamivudine treatment during pregnancy to prevent perinatal transmission of hepatitis B virus infection. J Viral Gepat 2003; 10(40); 294-7.
12. Peters MG. Special populations with hepatitis B infection. Hepatology 2009; 49(5 suppl): S146.
13. Lok AS. Management of hepatitis B: summary of a clinical research workshop. Hepatology 2007; 45(4): 1056-75.
14. Mast EE. A comprehensive immunization strategy to eliminat3e transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices: infants, children and adolescents. MMWR Recom Rep 2005; 54: 1-31.
15. Tse KY. The impact of maternal HBsAg carrier status on pregnancy outcomes: a case-control study.J Hepatol 2005; 43(5): 771-5.
16. Wong S. Hepatitis B Carrier and perinatal outcome in singleton pregnancy. Am J perinatol 1999; 16(9): 485-8.
17. Lin HH. Postpartum subsidence of hepatitis b viral replication in HBeAg-positive carrier mothers. J Med Virol 1989; 29(1): 1-6.
18. Almog Y. Oestrogen suppresses hepatitis b virus expression in male athymic mice transplanted with HBV. Antiviral Res 1992; 19(4): 285-93.
19. Beasley RP. Evidence against breastfeeding as a mechanism for vertical transmission of hepatitis B. Lancet 1975; 2: 740-1.
1. Lok AS. Chronic hepatitis B. N Engl J Med 2002; 346(22): 1682-3. [ Links ]
2. Yao JL. Perinatal transmission of hepatitis B virus infection and vaccination in China. Gut 1996; 38: s37-38. [ Links ]
3. Euler G. Hepatitis B surface antigen prevalence among pregnant women in urban areas: implications for testing, reporting and preventing perinatal transmission. Pediatrics 2003; 111: 1192-97. [ Links ]
4. Gupta I. Immunogenicity and safety of two schedules of hepatitis B vaccination during pregnancy. J Obstet Gynaecol Res 2003; 29(2): 84-6. [ Links ]
5. Okada K. Antigen and anti-e in the serum of asymptomatic carrier mothers as indicators of positive and negative transmission of hepatitis B virus to their infants. N Engl J Med 1976; 294(14): 746-49. [ Links ]
6. Guntupalli SR. Hepatic diseases and pregnancy: an overview of diagnosis and management. Crit Care Med 2005; 33(10): S332-9. [ Links ]
7. Xu DZ. Risk factors and mechanism of transplacental transmission of hepatitis B virus. J Med Virol 2002; 67(1): 20-6. [ Links ]
8. Su G. Efficacy and safety of lamivudine treatment or chronic hepatitis B in pregnancy. World Gastroentrol 2004; 10(6): 910-12. [ Links ]
9. Tang JR. Hepatitis B surface antigenemia at birth: a long term follow-up study. J Pediatr 1998; 133(3): 374-7. [ Links ]
10. Tran TT. Management of the pregnant hepatitis B patient. Curr Hepat Rep 2008; 2: 43-48. [ Links ]
11. Van Zonneveld M. Lamivudine treatment during pregnancy to prevent perinatal transmission of hepatitis B virus infection. J Viral Gepat 2003; 10(40; 294-7. [ Links ]
12. Peters MG. Special populations with hepatitis B infection. Hepatology 2009; 49(5 suppl): S146. [ Links ]
13. Lok AS. Management of hepatitis B: summary of a clinical research workshop. Hepatology 2007; 45(4): 1056-75. [ Links ]
14. Mast EE. A comprehensive immunization strategy to eliminat3e transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices: infants, children and adolescents. MMWR Recom Rep 2005; 54: 1-31. [ Links ]
15. Tse KY. The impact of maternal HBsAg carrier status on pregnancy outcomes: a case-control study.J Hepatol 2005; 43(5): 771-5. [ Links ]
16. Wong S. Hepatitis B Carrier and perinatal outcome in singleton pregnancy. Am J perinatol 1999; 16(9): 485-8. [ Links ]
17. Lin HH. Postpartum subsidence of hepatitis b viral replication in HBeAg-positive carrier mothers. J Med Virol 1989; 29(1): 1-6. [ Links ]
18. Almog Y. Oestrogen suppresses hepatitis b virus expression in male athymic mice transplanted with HBV. Antiviral Res 1992; 19(4): 285-93. [ Links ]
19. Beasley RP. Evidence against breastfeeding as a mechanism for vertical transmission of hepatitis B. Lancet 1975; 2: 740-1. [ Links ]

