










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.3 Bogotá Sept. 2011
Quality management of Inflammatory Bowel Disease
Fabián Juliao Baños, MD (1)
(1) Section Chief of Gastroenterology and Digestive Endoscopy. Inflammatory Bowel Disease Consultation Coordinator at the Hospital Pablo Tobon Uribe in Medellin, Colombia. Professor at the Pontificia Universidad de Antioquia and Universidad Bolivariana in Medellín, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 13-04-11 Accepted: 02-08-11
Abstract
The management of patients with both types of inflammatory bowel disease (IBD), Ulcerative Colitis and Crohn's Disease, varies in medical centers around the world. Recognition of this variability in patient management is the initial step in improving the quality of care of IBD patients. The need for improvement is reflected in the overuse, underuse or misuse of medical services currently available. Having the appropriate knowledge, well adjusted to medical recommendations based on clinical evidence is important if we are to give our patients the best care. This review will provide recommendations regarding IBD patient treatment quality, as well as for prevention of complications associated with the disease and established medical treatment.
Keywords
Inflammatory bowel disease, ulcerative colitis, Crohn's disease, quality of care.
INTRODUCTION
Basing patient care quality on accepted international standards is the main mechanism by which we can provide a level of adequate health care to the population. In 1990 the Institute of Medicine in the USA defined quality health as, "The quality of care in which health services increase the possibility of desired outcomes in patients, which are consistent with current medical knowledge."
A random population study of 12 U.S. cities which surveyed 6,712 adults asked about quality management and found that only 54.9% of individuals receive recommended care. The proportion of acute care was 53.5%, 56.1% for chronic conditions and 52.2% for preventive care (1). A similar study of the same group which surveyed 1,536 children in the same cities found that 46.5% of them receive the recommended care. The proportion of acute care was 67.6%, 53.4% for chronic conditions and 40.7% for preventive actions (2).
It is therefore important to have the appropriate knowledge adjusted to established medical recommendations to give our patients the best care. We see this in our daily practice where overuse, underuse or wrong use of the medical resources we have at our disposal is seen. Recognition of the variability of patient management is the initial step for improving quality of care.
There is great variability in the management of patients with inflammatory bowel disease (IBD) around the world. A study of 64 patients attending consultation for a second opinion at the Women's Hospital in Boston assessed adherence to established guidelines. It found that 64% were receiving suboptimal doses of aminosalicylates (5-ASA). 75% with ulcerative distal colitis did not receive topical 5-ASA and 77% of patients had received steroids for more than 3 months. No attempt had been made to treat 59% of patients with alternatives to steroids such as other immunosuppresors or biological therapy with antibodies against tumor necrosis factor (anti-TNF). 82% of patients using azathioprine had sub-therapeutic doses while 78% of patients received steroid treatment inadequate for prevention of metabolic bone disease. 33% of patients with indications for monitoring colorectal cancer or dysplasia did not undergo colonoscopies (3). Another study in China found that only 54.4% of patients with distal colitis received topical 5-ASA, 27.8% of patients with severe IBD were not treated with steroids and only 19.6% of patients with indications for thiopurines received them. 57% of them were given suboptimal doses (48).
A survey of 186 members of the American Gastroenterological Association about management of Crohn's disease found a high rate of prescription of 5-ASA although little evidence exists for its clinical use. It was especially prescribed by physicians who were not experts in the management of IBD (49).
Vaccinations against preventable disease are important, especially for immunosuppressed patients with IBD. A recent study found that only 45% of these patients received tetanus vaccinations in the previous 10 years, only 28% had annual influenza vaccinations, only 9% were vaccinated against pneumonia, and only 33% of at risk patients had hepatitis B immunization (4).
QUALITY IN TREATMENT OF IBD
Initial treatment of patients with mild to moderate ulcerative colitis is based on 5-ASA derivatives. The presentation to be used depends on the extent of the disease. For patients with ulcerative proctitis, the recommendation is to use 1g/day treatment with 5-ASA suppositories. Liquid or foam enemas are preferable because they are more effective than oral 5-ASA derivatives and topical steroids (5,6). A metaanalysis of patients with active proctitis showed that the average remission rate for treatment with topical 5-ASA derivatives was 67% while the placebo response was 11% (7). For patients with the last 50 cm of the colon compromised by colitis, a combination of topical 5-ASA derivatives with oral 5-ASA is better than administering either separately (8) as patients with extensive colitis do not initially respond to oral 5 -ASA, but do benefit from the addition of topical 5-ASA (9).
Patients with mild to moderate ulcerative colitis that does not respond to treatment with 5-ASA derivatives within 2 weeks should receive oral steroids. The recommended daily dose is 40 mg of oral prednisone. This should be gradually decreased by 5 to10 mg every week after clinical remission has been achieved until the dosage reaches 20 mg/day. At that point daily dosage is should be reduced by 2.5 mg every week until treatment is suspended (10). Similarly, maximum recommended duration of steroid treatment is 12 to 16 weeks. Patients who require more than 1 or 2 courses of steroid treatment a year or who are steroid dependent (those unable to reduce doses of prednisone below 10 mg/day or reduce budesonide doses below 3 mg/day in 3 months who or relapse within 3 months after discontinuation) require steroid sparing strategies such as the use of other immunosuppressants or biological therapy (11).
It is well established that the best way to maintain clinical remission of Crohn's disease is to administer 2.5 mg/kg/day doses of azathioprine. A recent Cochrane review found that the OR of effectiveness with this dosage is 4.1, while for doses of 2.0 mg/kg/day it is 3.0 and for 1.0 mg/kg/day it is 1.2 (12).
Safety of the use of certain medications prior to surgery for patients with Crohn's disease and ulcerative colitis is quite controversial. There is a consensus that prednisone dosage of over 20 mg/day for more than 6 weeks is a risk factor for surgical complications. This drug should be discontinued if possible prior to surgery. If the patient has received steroids for 1 to 3 months, the rate of dosage decrease should be 5 mg per week, but if the treatment had been for 3 to 6 months, the reduction should be 2.5 mg per week. In contrast, thiopurines such as azathioprine appear to be safe in this context (17, 18).
The relation between peri-operative use of anti-TNF therapy and the risk of postoperative complications remains controversial. A recent metaanalysis of 5 studies and 706 patients has shown a higher than normal rate of postoperative complications among patients with who received anti-TNF therapy (OR 1.8). This was especially pronounced for patients with infectious ulcerative colitis (OR 2.24) (19). This has not been demonstrated in patients with Crohn's disease. Furthermore, there is no consensus on the minimum time required between suspension of anti-TNF therapy and surgery. Some say that the time should be a month, but therapeutic concentrations of infliximab have been were detected for up to 8 weeks after infusion (6,20).
Frequently, diagnosis of Crohn's disease in Colombia occurs after an urgent surgical procedure. We know that 60% to 75% of patients with Crohn's disease require surgical treatments at different points of their lives because of complications associated with stricturing or penetrating. It has been estimated that 70% of patients require further surgery after 20 years of follow-up. Surgery is not curative, and symptoms recur in 30% of patients after 3 years, and in 60% after 10 years. In fact, we have found that endoscopically diagnosed recurrence occurs in 70% to 90% of patients within 1 year following surgery. Depending on the severity diagnosed endoscopically, these diagnoses are then correlated with clinical recurrence (38).
Risk factors for surgical recurrence of Crohn's disease include stricturing or penetrating pattern, age at initial surgery (younger patients have greater risks of recurrence), smoking, ileocolonic locations and time elapsed between diagnosis and first surgery. The rates of clinical and endoscopic recurrence in patients with Crohn's disease after first surgery according to different treatments and different studies are as follows: placebo (25% to 77%, 53% to 79%), 5-ASA (24% to 58%, 63% to 66%), budesonide (19% to 32%, 52% to 57%), nitroimidazoles (7% to 8%, 52% to 54%), thiopurines (34% to 50%, 42% to 44% ) and infliximab (0%, 9%) which is the most effective. A management algorithm proposed by Regueiro is shown in Figure 1. This algorithm is important for determination of postsurgical risks facing individual Crohn's disease patients. It indicates endoscopic findings and risk factors to look for to provide the best treatment for our patients (39).
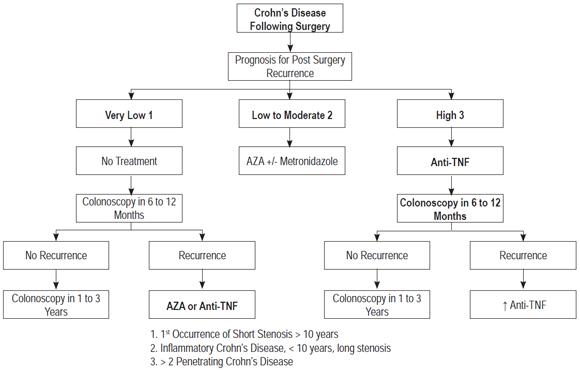
Figure 1. Risk measurement and management of Crohn's disease after surgery. Taken from M. Regueiro Inflamm Bowel Dis 2009; 15:1583-1590.
A recent systematic review found that 67%, of patients with severe ulcerative colitis admitted to the emergency room responded to intravenous steroids (hydrocortisone and methylprednisolone). 29% of them required colectomies. The mortality rate was 1% (40). 6% to 7.9% of them developed toxic megacolon with a mortality rate of around 19%. The mortality rate increased to 41.5% for patients with perforations (41). There are two major dilemmas in management of these individuals' care: how to identify patients at high risk for complications and when to start rescue therapy (Infliximab or cyclosporine) to prevent colectomy. Although there are no comparative studies between these two drugs, infliximab is preferable to cyclosporine for patients previously exposed to azathioprine. The long-term results for patients who have avoided surgery with rescue therapy show that 80% of patients treated with cyclosporin required colectomies after 7 years whereas with infliximab 50% required colectomies 3 years later. Therefore, some authors suggest that these drugs differ from surgery only in the percentage of cases, but this would be elective when it would improve a patient's prognosis (46).
It has been found that patients with more than 12 stools on the second day of treatment have a 55% risk for colectomy whereas those with more than 8 stools on the third day have an 85% risk. One study found that when levels of CRP are over 45 mg/L on the third day and the number of stools is from 3 to 8 per day the risk of colectomy increases to 85%. Other risk factors include albumin <3.0 g/dl, levels of fecal calprotectin > 1922 mg/g, colonic dilatation> 5.5 cm as diagnosed by abdominal x-rays (75% risk of colectomy) and colonoscopic diagnosis of deep ulcers (93% risk of colectomy) (42). Flexible sigmoidoscopy is preferable to total colonoscopy for patients with severe acute ulcerative colitis due to the high risk of perforation. Preferably this procedure should be conducted without colonic preparation, with minimal inflation, and always with biopsies to rule out infection with cytomegalovirus (CMV). This is especially important for patients with prior exposure to steroids or azathioprine (6,46).
In conclusion, we recommend starting "rescue" therapy in patients with severe ulcerative colitis who do not respond to initial treatment with intravenous steroids after 3 to 5 days of treatment. In cases of partial responses on the third day, one might continue steroids for up to 7 days before starting rescue therapy (47). Please note the risk factors mentioned above, and talk with patient and family about future management possibilities using infliximab or cyclosporine. Also, talk to the gastrointestinal surgeon or coloproctologist about the high risk of colectomy in these cases. Sometimes, it is preferable to perform a colectomy in time and not risk the patient's life since there are high risks of mortality associated with complications from severe acute ulcerative colitis.
QUALITY IN THE PREVENTION OF IBD COMPLICATIONS
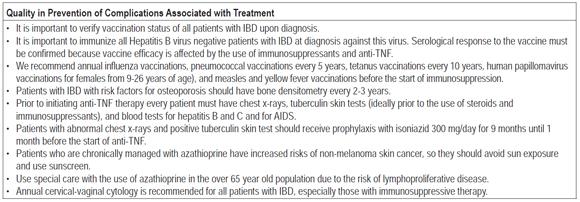
Medical treatment of patients with IBD involves increased use of immunosuppressive drugs which increase risks of infections. Some of these are preventable with the use of vaccinations. Therefore, it is important to check the vaccination status of patients at the time of the initial consultation, ideally at the time of diagnosis. Guidelines for immunization in patients with inflammatory bowel disease (13) recommend annual vaccinations against influenza with inactivated trivalent vaccine, polyvalent pneumococcal vaccine every 5 years (Pneumovax 23), screening of patients at risk for hepatitis B prior to immunosuppression and vaccination with three doses (0, 1 and 6 months), tetanus toxin vaccine every 10 years and quadrivalent human papilloma virus vaccination in 3 doses for women between 9 and 26 years of age. Quadrivalent human papilloma virus vaccination is also recommended for immunosuppressed men in the same age range who have perianal Crohn's disease due to risks of HPV infection and anal cancer. Avoid vaccination with live and attenuated viruses for patients undergoing immunosuppressive therapy. Therefore chickenpox vaccinations in 2 doses are recommended prior to immunosuppression, as is yellow fever vaccine for travelers patients to endemic areas (14,43,50).
Smoking is a risk factor for Crohn's disease. Smokers have higher rates of relapse, hospitalization, and greater need for immunosuppressants and surgery than do nonsmokers. A prospective French study of 59 Crohn's disease patients who stopped smoking showed that they had a 65% lower one year relapse rate than did Crohn's disease patients who continued to smoke (15). Another study by the same French group found that in a follow up of 12 years, the proportion of years with active disease in non-smokers patients with Crohn's disease was significantly lower than that of light smokers (1 to 10 cigarettes/day) and of heavy smokers (more than 10 cigarettes/day) (37% vs. 46% vs. 48%, P <0.001) (16). It appears that smoking has deleterious effect on the clinical course of patients with Crohn's disease, independent of the number of cigarettes consumed per day by the patient, and that the prognosis for people who discontinue smoking is similar to that of nonsmokers.
For screening for colon cancer in patients with IBD we recommend colonoscopic biopsies (2 to 4 samples every 10 cm) for any patient with ulcerative colitis 8 to 10 years after onset of symptoms. Optimally, biopsies should be when the disease is in clinical remission. Thereafter, patients with extensive or left colitis require follow-up biopsies every 1 or 2 years, and annual colonoscopies after 20 years have passed from symptom onset. Patients with primary associated sclerosing cholangitis and patients who have family histories of first-degree colorectal cancer require annual monitoring. Individuals with proctitis or proctosigmoiditis are not at increased risk of colon cancer and require the same assessment as the general population according to their ages. Crohn's disease patients with colonic involvement of at least one third of its length require screening colonoscopies for colorectal cancer 8 to 10 years after onset preferably when the disease is in clinical remission. If it is negative for cancer, it requires follow-up every 1or 2 years, and annual colonoscopies after 20 years have passed from symptom onset (21,22).
One third of patients with IBD have recurrent anemia (hemoglobin <12 g/dl), a finding given little importance by physicians, but which is responsible for many symptoms such as dyspnea, tachycardia, chronic fatigue, nausea, and cognitive impairment all of which impair patient quality of life. The most common cause of anemia is iron deficiency and anemia associated with chronic disease. Other less frequent causes of anemia include vitamin B 12 deficiencies. This is especially the case for Crohn's disease patients with a history of ileal resection or those with ulcerative colitis with ileal pouches. It can also be associated with folic acid deficiency in patients with inadequate food intake. Also, certain medications such as 5-ASA derivatives have been associated with hemolysis, and the myelosuppressive effect of thiopurines such as azathioprine can cause anemia associated with pancytopenia (23).
If possible, maintain Hb levels should be kept over 12 g/dL for female IBD patients and over 13.5g/ dL for male IBD patients. Hemoglobin, hematocrit and ferritin levels of in patients in remission should be monitored every 6 to 12 months. Patients with active IBD cases should be checked every 3 months. In case of macrocytosis or risk factors for vitamin B 12 or folic acid deficiency, they should be measured annually. In patients with anemia and without clinical or laboratory signs of inflammation (CRP, leukocytosis), a ferritin level <30 mg/L and a transferrin saturation below 16% is indicative of iron deficiency anemia. In case of inflammation, the lower limit of ferritin allowed is 100 mg/L. The diagnostic criteria for anemia associated with chronic diseases are ferritin levels > 100 mg/L and transferrin saturation below 16% (24).
In the treatment of anemia in patients with IBD the goal is an increase of 2 g/dL of hemoglobin in 4 weeks. The ideal is to achieve a ferritin level over 100 mg/L and transferrin saturation between 16% and 50%. The simplest treatment is the start of oral iron. However, this is ruled out for patients with Crohn's disease with involvement of small intestine where local Fenton reaction producing free radicals that imply increased inflammation is likely. A dose of 100 mg/day of elemental iron is sufficient, considering that the body can only absorb 10 mg/day. However, the parenteral route is preferred over oral iron for rapid and prolonged response, good tolerance and improvement of quality of life. The total dose of parenteral iron is 1,200 mg intravenously over 4 weeks, 200 mg diluted in 250 ml of saline solution administered twice weekly for 2 weeks. This should be followed by 200 mg weekly for another 2 weeks. This treatment is effective in 65% of patients. Absolute indications for the use of parenteral iron are the presence of severe anemia (Hb <10 g / dL), intolerance (21%) and lack of response to oral iron. Patient preference and severe inflammatory involvement of small intestine must also be considered. Agents such as erythropoietin are indicated in anemia associated with chronic illnesses and when there is no response to parenteral iron (23,24).
The overall prevalence of osteoporosis in patients with IBD is around 15%, but obviously varies according to patients' ages. Patients with this condition have a relative risk of fracture of 1.3 to 1.4 times greater than the general population. This risk is slightly higher for Crohn's disease patients than for those with ulcerative colitis. After 6 months of corticosteroid treatment at doses> 7.5 mg/day, there is a 50% risk of osteoporosis and a 50% risk of fracture. It is suggested bone densitometry should be performed for all patients with IBD with previous fractures or first degree fractures, with previous use of steroids (prednisone> 7.5 mg/day for more than 3 months), postmenopausal women, men over 50 years of age and people with lower than normal body mass indexes to rule out osteoporosis. This should be repeated every 2 to 3 years. General measures for prevention of osteoporosis include adequate daily calcium (1,200 mg) and vitamin D (400-800 IU) intakes, exercise, avoidance of smoking and alcohol, and limitation of prolonged use of steroid medication savers such as azathioprine and anti-TNF. On the other hand it is important to reduce inflammation in patients with IBD to decrease osteoclast activity. When osteoporosis (T score <-2.5) is present bisphosphonate management should be prescribed. For patients who require steroids, use of bisphosphonates should be initiated when their T scores fall below -1.0 (25, 26).
IBD patients have three times higher risk of thromboembolic events than does the general population. Among them there is a predominance of deep vein thrombosis and pulmonary embolism with an estimated incidence of 1% to 6.7%, and these tend to occur at younger ages. This procoagulant state is due to congenital and acquired prothrombotic factors, the latter of which is more important. Among inherited factors, the most common are mutation of Leiden V factor, homozygous mutation C667T in the methylenetetrahydrofolate reductase gene and mutation 20210A in the prothrombin gene. It is advisable to study these disorders in IBD patients with a history of thromboembolic events. Among acquired factors are inflammation, prolonged immobilization, hyperhomocysteinemia (nutritional deficiencies of vitamin B12, vitamin B6 and folic acid), smoking, surgery, central venous catheters, steroid therapy and oral contraceptive use. Prophylaxis with heparin should be performed for venous thrombosis in patients with these risk factors (32, 33, 34).
With the advent of biological therapy, particularly anti-TNF for patients with IBD, a concern about reactivation of latent tuberculosis has arisen. This concern is especially important in third world countries like ours where reactivation could have serious public health repercussions. An FDA report 10 years ago found 70 cases of active tuberculosis in 147,000 patients treated with infliximab. Infections were diagnosed on average 12 weeks after starting treatment with this drug. 56% of these cases were extrapulmonary, while 24% had disseminated or miliary presentations (27). These data were collected prior to the current recommendation of routine screening chest x-rays and tuberculosis testing for all patients prior to initiation of anti-TNF therapy. Recent data show that the incidence of tuberculosis in patients with IBD has declined significantly with the implementation of screening.
All individuals should be informed of tuberculosis risks prior to initiation of anti-TNF treatment, and should sign an informed consent form. Every patient should have chest x-rays. They should also have an intradermal tuberculin test despite its low specificity, the influence of BCG vaccination in its results (first 10 years), and possible false negative results related to anergia associated with steroids and immunosuppressive therapy (up to 83%). Recently an alternative method of diagnosing latent tuberculosis has been developed. It is a QuantiFERON-TB or T-SPOT.TB test that measures production of gamma interferon in T lymphocytes in response to in vitro stimulation with antigens from Mycobacterium tuberculosis not present in the vaccine (BCG). This makes it more specific than the tuberculin test. Furthermore, its result are not altered even in the presence of immunosuppressive therapy. It has been found that in patients with prior application of tuberculin QuantiFERON results can be altered. This can be avoided by applying the latter during the first 15 days after application of the first. Patients with latent tuberculosis (positive tuberculin test with hardening > 5 mm or abnormal chest radiograph) should be treated with isoniazid 300 mg/day for 9 months ending 1 month before the start of the first application of anti-TNF. This has been shown to reduce incidence of tuberculosis by 70%. Anti-TNF should be immediately discontinued in cases of active tuberculosis (28). The British Thoracic Society recommends that tuberculin test or QuantiFERON testing be repeated annually during maintenance of patients in anti-TNF therapy due to the risk of tuberculosis infection "de novo" with this treatment (50).
In addition, there are documented cases of reactivation of chronic hepatitis B infection in patients with anti-TNF. Therefore, application of surface antigen (HBsAg) and anti-core (anti-HBcore) prior to starting anti-TNF is recommended. If the HBsAg is positive, viral load should be sent, e antigen antibody to e antigen (HBeAg and anti-HBe). If the viral load (DNA) is> 20,000 copies and the HBeAg is positive, patients are called active carriers. Anti-TNF should be discontinued and hepatitis B should be treated as active. Patients with <20,000 copies are inactive carriers. For these patients chemoprophylaxis should be initiated with lamivudine 100 mg/day (if less than 12 months due to risk of resistance), 2 weeks before the start of anti-TNF and 3-6 months after discontinuance of anti-TNF with follow-up tests for ALT and viral load every 1 to 3 months during treatment. Patients without previous vaccinations for hepatitis B or with low levels of antibodies against HBsAg should be vaccinated. There is no evidence that treatment with anti-TNF exacerbates the course of hepatitis C infection, however we recommend monitoring ALT and viral loads of these patients. It is also advisable to request proof of human immunodeficiency virus or acquired immune deficiency syndrome (AIDS) prior to initiating anti-TNF (28, 43, 44, 45).
Increased incidence of non-melanoma type skin cancers have been found in patients with IBD compared to the general population (RR 1.64). The persistent use of azathioprine (OR 4.27) and biological therapy (OR 2.18) are risk factors for cancer development. Previous studies have shown that azathioprine increases the photosensitivity of human skin, so patients are advised to avoid sun exposure and use sunscreen daily. Where possible, they should be evaluated by a dermatologist (29,30).
The CESAME study group in France found an incidence of lymphoproliferative disease in patients receiving azathioprine of 0.9/1,000 patients/year. Its incidence was 0.20/1,000 patients/year among those who stopped treatment and 0.26/1,000 patients/year among those who never received azathioprine for management of IBD (p = 0.0054). The relative risk was 5.28 among those receiving thiopurines compared to those not treated with this drug. A more interesting finding is that patients less than 50 years of age had an incidence of 0.37/1,000 patients/year, between 50 and 60 years of age incidence was 2.58/1,000 patients/year and for patients over the age of 65 the incidence was 5.41/1,000 patients/year. All of this indicates the need for caution when considering the use of azathioprine for patients over 65 years old given the risk of lymphoproliferative disease (31).
In recent years there has been an increase in Clostridium difficile, anaerobic gram positive bacteria that damage the tissues by producing toxins A and B in patients with IBD. It leads to a more aggressive and severe course than among IBD patients than it does in people without IBD. The prevalence of this infection in IBD patients in acute crisis ranges from 5% to 18% of cases. It can be diagnosed by ELISA for toxin A and B in stool. In case of a negative result in initial sampling and an uncertain diagnosis, repeating the test increases its sensitivity. Risk factors include previous exposure to antibiotics (only 40% in IBD), the use of immunosuppressants (OR 2.58), previous use of proton pump inhibitors, advanced age, patient comorbidities and person-to-person infection. Clostridium difficile infection increases the time of hospitalization and the risk of colectomy (OR: 6.6). Currently high suspicion of Clostridium difficile infection is recommended for patients with severe IBD activity and presence of risk factors. An ELISA test for toxins A and B in the stool should be performed, and, if Clostridium difficile is diagnosed, early treatment should be started to prevent severe complications such as toxic megacolon and the need for surgery. Measures to isolate infected patients from contact are important, and it should be remembered that alcohol can not destroy the spores of this organism. After contact with the patient or patient's environment, wash with soap and water to sweep off spores (35).
Finally, women with IBD on immunosuppressive therapy and most smokers have a higher rate of abnormal cervical-vaginal cytology (CCV) than does the general population. These abnormalities could be related to increased rates of infection by human papillomavirus (HPV). A study by Sunanda Kane showed that 42.5% of patients with IBD had abnormal CCVs compared to only 7% of controls without IBD. In addition the study found that those undergoing immunosuppressive therapy for more than six months had 50% more abnormal CCVs . All lesions showed high-risk HPV (+) (36). CCV is currently recommended annually for all women with IBD, especially those undergoing immunosuppressive therapy. Women patients between the ages of 9 to 26 should be vaccinated against HPV, ideally before the onset of sexual intercourse. 3 doses of vaccine, one every 2 months should be applied. This protects against types 16 and 18 (responsible for 70% of cervical cancers), and against HPV types 6 and 11 associated with genital warts (37,50).
Inflammatory bowel disease is a non-curable disease, which requires medical management and/or surgical treatment to maintain disease remission and if possible achieve mucosal healing, improve quality of life, minimize complications of the disease and monitor adverse events associated with drugs used. Tables 1, 2 and 3 summarize a series of recommendations that will help us offer quality management for our patients.
Table 1. Summary of quality management recommendations for IBD patients.
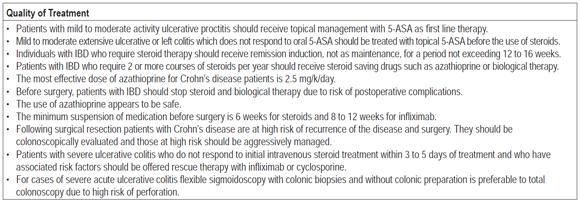
Table 2. Summary of quality management recommendations for patients with IBD
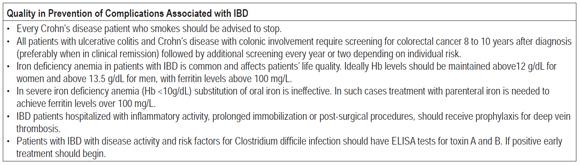
Table 3. Summary of quality management recommendations for IBD patients.
Acknowledgments
Thanks to my wife Lina and my daughters Pauline and Susana for their time.
REFERENCES
1. McGlynn EA, Asch SM, Adams J, et al. The Quality of Health Care Delivered to Adults in the United States. N Engl J Med 2003; 348: 2635-45.
2. Mangione-Smith R, DeCristofaro AH, Setodji CM, et al. The Quality of Ambulatory Care Delivered to Children in the United States. N Engl J Med 2007; 357: 1515-23.
3. Reddy SI, Friedman S, Banks P, et al. Are patients with inflammatory bowel disease receiving optimal care? Am J Gastroenterol 2005; 100: 1357-1361.
4. Melmed GY, Ippoliti AF, Papadakis KA, et al. Patients with Inflammatory Bowel Disease Are at Risk for Vaccine-Preventable Illnesses Am J Gastroenterol 2006; 101: 1834-1840.
5. Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: American college of gastroenterology, practice parameters committee. Am J Gastroenterol 2010; 105: 501-523.
6. Travis SP, Stange EF, Lémann M, et al. European evidence-based consensus on the management of ulcerative colitis: Current management. Journal of Crohn`s and Colitis 2008; 2: 24-62.
7. Marshall JK, Irvine EJ. Rectal aminosalicylate therapy for distal ulcerative colitis: a meta-analysis. Aliment Pharmacol Ther 1995; 9: 293-300.
8. Safdi M, DeMicco M, Sninsky C, et al. A double-blind comparison of oral vs. rectal mesalamine vs. combination therapy in the treatment of distal ulcerative colitis. Am J Gastroenterol 1997; 92: 1867-71.
9. Marteau P, Probert CS, Lindgren S, et al. Combined oral and enema treatment with Pentasa (mesalazine) is superior to oral therapy alone in patients with extensive mild/moderate active ulcerative colitis: a randomised, double blind, placebo controlled study. Gut 2005; 54: 960-5.
10. Lichtenstein GR, Abreu MT, Cohen R, et al. American Gastroenterological Association Institute technical review on corticosteroids, immunomodulators, and infliximab in inflammatory bowel disease. Gastroenterology 2006; 130: 940-987.
11. Panaccione R, Rutgeerts P, Sandborn WJ, et al. Review article: treatment algorithms to maximize remission and minimize corticosteroid dependence in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2008; 28: 674-688.
12. Prefontaine E, Sutherland LR, MacDonald JK, Cepoiu K. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn's disease (Review) Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No: CD000067.
13. Sands BE, Cuffari C, Katz J, et al. Guidelines for Immunizations in Patients with Inflammatory Bowel Disease. Inflamm Bowel Dis 2004; 10: 677-692.
14. Melmed GY. Vaccination Strategies for Patients with Inflammatory Bowel Disease on Immunomodulators and Biologics. Inflamm Bowel Dis 2009; 15: 1410-1416.
15. Cosnes J, Beaugerie L, Carbonnel F, Gendre JP. Smoking Cessation and the Course of Crohn`s Disease: An Intervention Study. Gastroenterology 2001; 120: 1093-1099.
16. Seksik P, Sokol H, Beaugerie L, Cosnes J. Effects of Light Smoking Consumption on the Clinical Course of Crohn's Disease. Inflamm Bowel Dis 2009; 15: 734-741.
17. Aberra FN, Lewis JD, Hass D, et al. Corticosteroids and immunomodulators: postoperative infectious complication risk in inflammatory bowel disease patients. Gastroenterology 2003; 125: 320-6.
18. Ferrante M, Vermiere S, Van Assche G, Rutgeerts P, et al. Corticosteroids but not Infliximab Increase Short-term Postoperative Infectious Complications in Patients with Ulcerative Colitis. Inflamm Bowel Dis 2009; 15: 1062-1070.
19. Yang Z, Wu Q, Wu K, Fan D. Meta-analysis: pre-operative infliximab treatment and short-term post-operative complications in patients with ulcerative colitis. Aliment Pharmacol Ther 2010; 31: 486-492.
20. Dignass A, Van Assche G, Lindsay JO, Lémann M, et al. The second European evidence-based consensus on the diagnosis and management of Crohn´s disease: Current management. Journal of Crohn`s and Colitis 2010; 4: 28-62.
21. Itzkowitz SH, Present DH. Consensus conference: colorectal cancer screening and surveillance in inflammatory bowel disease. Inflamm Bowel Dis 2005; 11: 314-321.
22. Farraye F, Odze R, Eaden J, Itzkowitz S. AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease. Gastroenterology 2010; 138: 746-774.
23. Gasche C, Lomer MC, Cavill I, Weiss G. Iron, anaemia, and inflammatory bowel diseases. Gut 2004; 53: 1190-1197.
24. Gasche C, Berstad A, Befrits R, Dignass A, et al. Guidelines on the Diagnosis and Management of Iron Deficiency and Anemia in Inflammatory Bowel Diseases. Inflamm Bowel Dis 2007; 13: 1545-1553.
25. Lichtenstein GR, Sands BE, Pezianas M. Prevention and Treatment of Osteoporosis in Inflammatory Bowel Disease. Inflamm Bowel Dis 2006; 12: 797-813.
26. Bernstein C, Leslie W, Leboff M. AGA Technical Review on Osteoporosis in Gastrointestinal Diseases. Gastroenterology 2003; 124: 795-841.
27. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. N Engl J Med 2001; 345: 1098-140.
28. Papa A, Mocci G, Bonizzi M, et al. Use of Infliximab in Particular Clinical Settings: Management Based on Current Evidence. Am J Gastroenterol 2009; 104: 1575-1586.
29. Long MD, Herfarth H, Pipkin C, et al. Increased Risk for Non-Melanoma Skin Cancer in Patients With Inflammatory Bowel Disease. Clin Gastroenterology and Hepatology 2010; 8: 268-274.
30. Smith MA, Irving PM, Marinaki AM, Sanderson JD. Review article: malignancy on thiopurine treatment with special reference to inflammatory bowel disease. Aliment Pharmacol Ther 2010; 32: 119-130.
31. Beaugerie L, Brousse N, Bouvier A, Colombel JF, et al. Lynphoproliferative disorders in patients receiving thiopurines for infl ammatory bowel disease: a prospective observational cohort study. Lancet 2009; 374: 1617-25.
32. Papa A, Danese S, Grillo A, Gasbarrini G, Gasbarrini A. Review Article: Inherited Thrombophilia in Inflammatory Bowel Disease. Am J Gastroenterol 2003; 98: 1247-1251.
33. Spina L, Saibeni S, Battaglioli T, et al. Thrombosis in Inflammatory Bowel Diseases: Role of Inherited Thrombophilia. Am J Gastroenterol 2005; 100: 2036-2041.
34. Yoshida H, Granger DN. Inflammatory Bowel Disease: A Paradigm for the Link between Coagulation and Inflammation. Inflamm Bowel Dis 2009; 15: 1245-1255.
35. Ananthakrishnan AN, Issa M, Binion D. Clostridium Difficile and Inflammatory Bowel Disease. Gastroenterol Clin N Am 2009; 38: 711-728.
36. Kane SV, Khatibi B, Reddy D. Use of immunosuppressants results in a higher incidence of abnormal Pap smears in women with inflammatory bowel disease. Am J Gastroenterol 2008; 103: 631-636.
37. Kane S. Abnormal Pap Smears in Inflammatory Bowel Disease. Inflamm Bowel Dis 2008; 14(8): 1158-60.
38. Rutgeerts P, Geboes K, Vantrappen G, et al. Predictability of the postoperative course of Crohn's disease. Gastroenterology 1990; 99: 956-983.
39. Regueiro M. Management and Prevention of Postoperative Crohn's Disease. Inflamm Bowel Dis 2009; 15: 1583-1590.
40. Turner D, Walsh C, Steinhart AH, et al. Response to corticosteroids in severe ulcerative colitis: a systematic review of the literature and a metaregression. Clin Gastroenterol Hepatol 2007; 5(1): 103-10.
41. Gan SI, Beck PL. A New Look at Toxic Megacolon: An Update and Review of Incidence, Etiology, Pathogenesis, and Management. Am J Gastroenterol 2003; 98: 2363-2371.
42. Travis S, Satsangi J, Lemann M. Predicting the need for colectomy in severe ulcerative colitis: a critical appraisal of clinical parameters and currently available biomarkers. Gut 2011; 60: 3-9.
43. Rahier JF, Ben-Horin S, Chowers Y, et al. European evidence-based Consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. J Crohn Colitis 2009; 3: 47-91.
44. Hou JK, Velayos F, Terrault N, Mahadevan U. Viral hepatitis and inflammatory bowel disease. Inflamm Bowel Dis 2010; 16: 925-32.
45. Gisbert JP, Chaparro M, Esteve M. Review article: prevention and management of hepatitis B and C infection in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2011; 33: 619-633.
46. Van Assche G, Vermeire S, Rutgeerts P. Management of acute severe ulcerative colitis. Gut 2011; 60: 130-133.
47. Hart AL, NG SC. Review article: the optimal medical Management of acute severe ulcerative colitis. Aliment Pharmacol Ther 2010; 32: 615-627.
48. Zhu Q, Cao Q, Jian-Min S. Quality of care for patients with inflammatory bowel disease in East China. World J Gastroenterol 2008; 14(4): 612-616.
49. Esralian E, Spiegel BM, Targownik LE, et al. Differences in the management of Crohn's disease among experts and community providers, based on a national survey of sample case vignettes. Aliment Pharmacol Ther 2007; 26, 1005-1018.
50. Moscandrew M, Mahadevan U, Kane S. General Health Maintenance in IBD. Inflamm Bowel Dis 2009; 15: 1399-1409.
1. McGlynn EA, Asch SM, Adams J, et al. The Quality of Health Care Delivered to Adults in the United States. N Engl J Med 2003; 348: 2635-45. [ Links ]
2. Mangione-Smith R, DeCristofaro AH, Setodji CM, et al. The Quality of Ambulatory Care Delivered to Children in the United States. N Engl J Med 2007; 357: 1515-23. [ Links ]
3. Reddy SI, Friedman S, Banks P, et al. Are patients with inflammatory bowel disease receiving optimal care? Am J Gastroenterol 2005; 100: 1357-1361. [ Links ]
4. Melmed GY, Ippoliti AF, Papadakis KA, et al. Patients with Inflammatory Bowel Disease Are at Risk for Vaccine-Preventable Illnesses Am J Gastroenterol 2006; 101: 1834-1840. [ Links ]
5. Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: American college of gastroenterology, practice parameters committee. Am J Gastroenterol 2010; 105: 501-523. [ Links ]
6. Travis SP, Stange EF, Lémann M, et al. European evidence-based consensus on the management of ulcerative colitis: Current management. Journal of Crohn's and Colitis 2008; 2: 24-62. [ Links ]
7. Marshall JK, Irvine EJ. Rectal aminosalicylate therapy for distal ulcerative colitis: a meta-analysis. Aliment Pharmacol Ther 1995; 9: 293-300. [ Links ]
8. Safdi M, DeMicco M, Sninsky C, et al. A double-blind comparison of oral vs. rectal mesalamine vs. combination therapy in the treatment of distal ulcerative colitis. Am J Gastroenterol 1997; 92: 1867-71. [ Links ]
9. Marteau P, Probert CS, Lindgren S, et al. Combined oral and enema treatment with Pentasa (mesalazine) is superior to oral therapy alone in patients with extensive mild/moderate active ulcerative colitis: a randomised, double blind, placebo controlled study. Gut 2005; 54: 960-5. [ Links ]
10. Lichtenstein GR, Abreu MT, Cohen R, et al. American Gastroenterological Association Institute technical review on corticosteroids, immunomodulators, and infliximab in inflammatory bowel disease. Gastroenterology 2006; 130: 940-987. [ Links ]
11. Panaccione R, Rutgeerts P, Sandborn WJ, et al. Review article: treatment algorithms to maximize remission and minimize corticosteroid dependence in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2008; 28: 674-688. [ Links ]
12. Prefontaine E, Sutherland LR, MacDonald JK, Cepoiu K. Azathioprine or 6-mercaptopurine for maintenance of remission in Crohn's disease (Review) Cochrane Database of Systematic Reviews 2009, Issue 1. Art. No: CD000067. [ Links ]
13. Sands BE, Cuffari C, Katz J, et al. Guidelines for Immunizations in Patients with Inflammatory Bowel Disease. Inflamm Bowel Dis 2004; 10: 677-692. [ Links ]
14. Melmed GY. Vaccination Strategies for Patients with Inflammatory Bowel Disease on Immunomodulators and Biologics. Inflamm Bowel Dis 2009; 15: 1410-1416. [ Links ]
15. Cosnes J, Beaugerie L, Carbonnel F, Gendre JP. Smoking Cessation and the Course of Crohn's Disease: An Intervention Study. Gastroenterology 2001; 120: 1093-1099. [ Links ]
16. Seksik P, Sokol H, Beaugerie L, Cosnes J. Effects of Light Smoking Consumption on the Clinical Course of Crohn's Disease. Inflamm Bowel Dis 2009; 15: 734-741. [ Links ]
17. Aberra FN, Lewis JD, Hass D, et al. Corticosteroids and immunomodulators: postoperative infectious complication risk in inflammatory bowel disease patients. Gastroenterology 2003; 125: 320-6. [ Links ]
18. Ferrante M, Vermiere S, Van Assche G, Rutgeerts P, et al. Corticosteroids but not Infliximab Increase Short-term Postoperative Infectious Complications in Patients with Ulcerative Colitis. Inflamm Bowel Dis 2009; 15: 1062-1070. [ Links ]
19. Yang Z, Wu Q, Wu K, Fan D. Meta-analysis: pre-operative infliximab treatment and short-term post-operative complications in patients with ulcerative colitis. Aliment Pharmacol Ther 2010; 31: 486-492. [ Links ]
20. Dignass A, Van Assche G, Lindsay JO, Lémann M, et al. The second European evidence-based consensus on the diagnosis and management of Crohn's disease: Current management. Journal of Crohn's and Colitis 2010; 4: 28-62. [ Links ]
21. Itzkowitz SH, Present DH. Consensus conference: colorectal cancer screening and surveillance in inflammatory bowel disease. Inflamm Bowel Dis 2005; 11: 314-321. [ Links ]
22. Farraye F, Odze R, Eaden J, Itzkowitz S. AGA Technical Review on the Diagnosis and Management of Colorectal Neoplasia in Inflammatory Bowel Disease. Gastroenterology 2010; 138: 746-774. [ Links ]
23. Gasche C, Lomer MC, Cavill I, Weiss G. Iron, anaemia, and inflammatory bowel diseases. Gut 2004; 53: 1190-1197. [ Links ]
24. Gasche C, Berstad A, Befrits R, Dignass A, et al. Guidelines on the Diagnosis and Management of Iron Deficiency and Anemia in Inflammatory Bowel Diseases. Inflamm Bowel Dis 2007; 13: 1545-1553. [ Links ]
25. Lichtenstein GR, Sands BE, Pezianas M. Prevention and Treatment of Osteoporosis in Inflammatory Bowel Disease. Inflamm Bowel Dis 2006; 12: 797-813. [ Links ]
26. Bernstein C, Leslie W, Leboff M. AGA Technical Review on Osteoporosis in Gastrointestinal Diseases. Gastroenterology 2003; 124: 795-841. [ Links ]
27. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. N Engl J Med 2001; 345: 1098-140. [ Links ]
28. Papa A, Mocci G, Bonizzi M, et al. Use of Infliximab in Particular Clinical Settings: Management Based on Current Evidence. Am J Gastroenterol 2009; 104: 1575-1586. [ Links ]
29. Long MD, Herfarth H, Pipkin C, et al. Increased Risk for Non-Melanoma Skin Cancer in Patients With Inflammatory Bowel Disease. Clin Gastroenterology and Hepatology 2010; 8: 268-274. [ Links ]
30. Smith MA, Irving PM, Marinaki AM, Sanderson JD. Review article: malignancy on thiopurine treatment with special reference to inflammatory bowel disease. Aliment Pharmacol Ther 2010; 32: 119-130. [ Links ]
31. Beaugerie L, Brousse N, Bouvier A, Colombel JF, et al. Lynphoproliferative disorders in patients receiving thiopurines for infl ammatory bowel disease: a prospective observational cohort study. Lancet 2009; 374: 1617-25. [ Links ]
32. Papa A, Danese S, Grillo A, Gasbarrini G, Gasbarrini A. Review Article: Inherited Thrombophilia in Inflammatory Bowel Disease. Am J Gastroenterol 2003; 98: 1247-1251. [ Links ]
33. Spina L, Saibeni S, Battaglioli T, et al. Thrombosis in Inflammatory Bowel Diseases: Role of Inherited Thrombophilia. Am J Gastroenterol 2005; 100: 2036-2041. [ Links ]
34. Yoshida H, Granger DN. Inflammatory Bowel Disease: A Paradigm for the Link between Coagulation and Inflammation. Inflamm Bowel Dis 2009; 15: 1245-1255. [ Links ]
35. Ananthakrishnan AN, Issa M, Binion D. Clostridium Difficile and Inflammatory Bowel Disease. Gastroenterol Clin N Am 2009; 38: 711-728. [ Links ]
36. Kane SV, Khatibi B, Reddy D. Use of immunosuppressants results in a higher incidence of abnormal Pap smears in women with inflammatory bowel disease. Am J Gastroenterol 2008; 103: 631-636. [ Links ]
37. Kane S. Abnormal Pap Smears in Inflammatory Bowel Disease. Inflamm Bowel Dis 2008; 14(8): 1158-60. [ Links ]
38. Rutgeerts P, Geboes K, Vantrappen G, et al. Predictability of the postoperative course of Crohn's disease. Gastroenterology 1990; 99: 956-983. [ Links ]
39. Regueiro M. Management and Prevention of Postoperative Crohn's Disease. Inflamm Bowel Dis 2009; 15: 1583-1590. [ Links ]
40. Turner D, Walsh C, Steinhart AH, et al. Response to corticosteroids in severe ulcerative colitis: a systematic review of the literature and a metaregression. Clin Gastroenterol Hepatol 2007; 5(1): 103-10. [ Links ]
41. Gan SI, Beck PL. A New Look at Toxic Megacolon: An Update and Review of Incidence, Etiology, Pathogenesis, and Management. Am J Gastroenterol 2003; 98: 2363-2371. [ Links ]
42. Travis S, Satsangi J, Lemann M. Predicting the need for colectomy in severe ulcerative colitis: a critical appraisal of clinical parameters and currently available biomarkers. Gut 2011; 60: 3-9. [ Links ]
43. Rahier JF, Ben-Horin S, Chowers Y, et al. European evidence-based Consensus on the prevention, diagnosis and management of opportunistic infections in inflammatory bowel disease. J Crohn Colitis 2009; 3: 47-91. [ Links ]
44. Hou JK, Velayos F, Terrault N, Mahadevan U. Viral hepatitis and inflammatory bowel disease. Inflamm Bowel Dis 2010; 16: 925-32. [ Links ]
45. Gisbert JP, Chaparro M, Esteve M. Review article: prevention and management of hepatitis B and C infection in patients with inflammatory bowel disease. Aliment Pharmacol Ther 2011; 33: 619-633. [ Links ]
46. Van Assche G, Vermeire S, Rutgeerts P. Management of acute severe ulcerative colitis. Gut 2011; 60: 130-133. [ Links ]
47. Hart AL, NG SC. Review article: the optimal medical Management of acute severe ulcerative colitis. Aliment Pharmacol Ther 2010; 32: 615-627. [ Links ]
48. Zhu Q, Cao Q, Jian-Min S. Quality of care for patients with inflammatory bowel disease in East China. World J Gastroenterol 2008; 14(4): 612-616. [ Links ]
49. Esralian E, Spiegel BM, Targownik LE, et al. Differences in the management of Crohn's disease among experts and community providers, based on a national survey of sample case vignettes. Aliment Pharmacol Ther 2007; 26, 1005-1018. [ Links ]
50. Moscandrew M, Mahadevan U, Kane S. General Health Maintenance in IBD. Inflamm Bowel Dis 2009; 15: 1399-1409. [ Links ]

