










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.3 Bogotá set. 2011
Case report: Ulcers in the small intestine due to glucosamine and methylsulfonylmethane (MSM) use
Nicolás Zuluaga, MD (1), Luis F. Roldán, MD (1), Mauricio González, MD (1), Raúl Ríos, MD (2), Yezid Farfán, MD (1), Antonio Restrepo, MD (1)
(1) Gastroenterologist at the Instituto Gastroclinico in Medellín, Colombia.
(2) General Practitioner at the Unidad de Fisiología of the Instituto Gastroclinico in Medellín, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 13-09-10 Accepted: 02-08-11
Abstract
We report on the case of a female patient with abdominal pain, iron deficiency anemia who tested positive for fecal occult blood but had no overt gastrointestinal bleeding. Patient had a known history of osteoarthritis and used Glucosamine - MSM. Both upper GI endoscopy and colonoscopy were negative. Capsule endoscopy showed multiple concentric ulcers, several of which were actively bleeding. Patient reported no use of NSAIDs, and there was no evidence of Crohn's disease. Nutritional supplements were stopped. After four weeks abdominal pain improved, patient had anemia and a fecal occult blood test was negative. Symptoms have not recurred.
Key words
Small intestinal ulcers, methylsulfonylmethane, MSM.
The patient is a 66 year old woman who had suffered from twelve months of generalized colicky pain with greatest intensity in the right iliac fossa and upper right quadrant. Defecation resulted in little improvement. Colic was associated with distension, nausea, occasional vomiting, asthenia and adynamia. Patient defected easily 2-3 times per day. Stools were soft, without blood or melenas. Patient suffered no weight loss, but had pain in both knees.
The patient had a history of osteoarthritis which had been managed for a year with glucosamine, chondroitin sulfate and MSM. Patient took no anti-inflammatory medications or acetaminophen after it was noticed they had no positive effect but did generate epigastric discomfort. The patient had undergone a cholecystectomy, a hysterectomy and a cystopexy. She had no allergies or history of transfusions. Patient does not smoke or consume liquor and has no pertinent family history.
Findings from a physical examination of the patients showed HR 80/min, weight 70 kg, and arterial pressure of 120/80. The patient was alert and well oriented. She was pale and experienced pain upon palpation of the right iliac fossa and upper right quadrant but had no masses, enlargements or adenopathies. There were no other positive findings in the physical examination.
The patient's complete blood count showed a hemoglobin count of 9 gr/dl and showed that the patient was both hypochromic and microcytic with 8,000 leukocytes/mm3 and 320,000 platelets/ mm3. Nitrogen compounds and hepatic profile were normal. Fecal matter tested positive for human hemoglobin. Upper endoscopy showed a hiatal hernia and erythematous gastritis in the antrum. A biopsy determined that the patient suffered from chronic inflammation, but that no Helicobacter pylori were present. A total colonoscopy showed diverticulosis in the colon. Distal ileoscopy was normal. Because of occult bleeding capsule enteroscopy was performed. It demonstrated multiple concentric superficial ulcers with clear edges throughout. Some, located within the mucosa, were actively bleeding; otherwise the appearance of the mucosa was normal. Slight cicatricial stenosis was also found. (See Figures 1, 2, 3, 4 and 5)

Figure 1. Concentric Ulcer.

Figure 2. Fibrous scar with slight stenosis.

Figure 3. Ulcer with active bleeding.

Figure 4. Ulcer with signs of active bleeding.

Figure 5. Ulcer with beginning of layered bleeding.
After these studies patient was sent for evaluation by gastroenterologist. Tests for anti-nuclear antibodies (ANAs) antibodies to Saccharomyces cerevisiae (ASCAs) and anti-neutrophil cytoplasmic antibody (ANCAs) were all negative. Tests of patient's erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were normal. In agreement with the patient, glucosamine with MSM was suspended and replaced with 1.5 gr of mesalazine and 1 tablet of ferrous sulfate daily. A check up one month showed complete resolution of patient's symptoms. Hemoglobin level was 12 gr/dl, and a test of fecal matter for occult bleeding was negative. Mesalazine and ferrous sulfate were suspended. An additional check up four months later confirmed complete resolution of patient's symptoms with a hemoglobin level of 13 gr/dl and a test of fecal matter for occult bleeding which again was negative.
DISCUSSION
Currently use of an endoscopic video capsule is recommended as a first line tool for evaluation of the small intestine of patients with occult digestive bleeding (1). This method has identified that the most frequent causes of occult digestive bleeding are vascular lesions, polyps, neoplasias and ulcers (2).
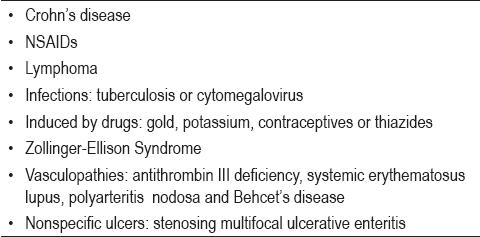
Various entities can cause multiple stenosing ulcers of the small intestine such as those our patient presented (Table 1) (3-5). Of these NSAIDs and Crohn's disease are the most representative.
Table 1. Causes of ulceration with stenosis on the small intestine.
NSAIDs may cause erosions and ulcers of diverse forms, but the main characteristics of these ulcers are that they are concentric and superficial and have clear edges. Similarly, as these ulcers heal the process causes stenoses similar to diaphragms (6). Although diagnosis of NSAID enteropathy has not been standardized, some authors (7) have proposed the following criteria:
1. A history of NSAID use
2. Findings of erosion, ulcer and/or typical stenosis
3. Improvement of clinical findings and/or endoscopic findings upon suspension of NSAIDs
4. Exclusion of inflammatory bowel disease, neoplasia and infectious diseases.
Ulcers appearing in Crohn's disease can be aphthous, longitudinal or stenosing. They appear together with patches of cobblestone mucosa, inflammatory pseudopolyps and are clinically associated with extraintestinal manifestations, fissures or fistulas (8, 9).
There are also reports of two rare and little understood entities which resemble NSAID enteropathy: chronic non-specific ulcers of the small intestine and cryptogenic multifocal ulcerous stenosing enteritis (CMUSE) (3, 4). Patients with these entities have neither histories of NSAID use nor inflammatory or infectious diseases. Chronic non-specific ulcers of the small intestine are characterized by their distal location in the small intestine and by recurrence even after surgery. In cases of CMUSE there are manifold ulcers and stenoses in the small intestine that may respond to treatment with corticoids. Whether these two entities are related, or if they are variants of other diseases, is not known. We also do not yet know the incidence of these conditions here in Colombia.
The patient reported on here had a low clinical probability of Crohn's disease and had no indications of other diseases. Patient had not been prescribed NSAIDs, although it is not possible to rule out surreptitious use. Improvement upon suspension of glucosamine with MSM (which has anti-inflammatory properties) makes this compound the main suspect for the cause of this enteropathy (10).
MSM (Methylsulfonylmethane) is a nutritional supplement that is used to reduce peripheral pain, inflammation and arthritis. It can inhibit the degenerative changes that occur in osteoarthritis. This compound may act through its ability to stabilize cellular membranes, to slow or to stop the response of injured cells, and to sweep away free hydrogen radicals. Its sulfide content can help rectify dietary deficiencies and improve cartilage formation (11, 12). Studies of murine macrophages have demonstrated that MSM inhibits the increase induced by nitric oxide lipopolysaccharides and E2 prostaglandin through the suppression of inducible nitric oxide synthase and COX - 2 expression (13). In spite of these possible beneficial effects there is no clear evidence of its clinical utility (11, 12).
Studies that have evaluated this component do not report its gastrointestinal toxicity, although they do make reference to possible allergic reactions, abdominal discomfort and cutaneous rashes (10-12). Because of its implications, it is vitally important that we learn about this secondary effect. In our institution we are currently studying the association of this compound and other natural supplements with several similar cases.
REFERENCES
1. ASGE Standards of Practice Committee. The role of endoscopy in the management of obscure GI bleeding. Gastrointest Endosc 2010; 72: 471-479.
2. Rockey D. occult and obscure gastrointestinal bleeding: causes and clinical management. Nat Rev Gastroenterol. Hepatol 2010; 7: 265-279.
3. Chen Y, Ma W, Chen J, Cai J. Multiple chronic non-specific ulcer of small intestine characterized by anemia and hypoalbuminemia. World J Gastroenterol 2010; 16: 782-784.
4. Freeman H. Multifocal stenosing ulceration of the small intestine. World J Gastroenterol 2009; 15: 4883-4885.
5. Zeino Z. Adverse effects of drugs on small intestine and colon. Best Pract Res Clin Gastroenterol 2010; 24: 133-141.
6. Higuchi K, Umegaki E, Watanabe T, Yoda Y, Morita E, Murano M. Present status and strategy of NSAIDs-induced small bowel injury. J Gastroenterol 2009; 44: 879-888.
7. Hayashi Y, Yamamoto H, Taguchi H, Sunada K, Miyata T, Yano T, Arashiro M, Sugano K. Nonsteroidal anti-inflammatory drug-induced small-bowel lesions identified by double-balloon endoscopy: endoscopic features of the lesions and endoscopic treatments for diaphragm disease. J Gastroenterol 2009; 44(Suppl XIX): 57-63.
8. Matsumoto T, Iida M, Matsui T, Yao T. Chronic nonspecific multiple ulcers of the small intestine: a proposal of the entity from Japanese gastroenterologists to Western enteroscopists. Gastrointest Endosc 2007; 66: S99-S107.
9. Chang D, Kim J, Choi H, Soo Eun C, Han D, Byeon J, Kim JO. Double balloon endoscopy in small intestinal Crohn's disease and other inflammatory diseases such as cryptogenic multifocal ulcerous stenosing enteritis (CMUSE). Gastrointest Endosc 2007; 66: S96-S98.
10. Anonymous. Methylsulfonylmethane (MSM). Monograph. Altern Med Rev 2003; 8: 438-41.
11. Brien S, Prescott P, Lewith G. Meta-analysis of the Related Nutritional Supplements Dimethyl Sulfoxide and Methylsulfonylmethane in the Treatment of Osteoarthritis of the Knee. Evid Based Complement Alternat Med 2009; 1-10.
12. Brien S, Prescott P, Bashir N, Lewith H, Lewith G. Review Systematic review of the nutritional supplements dimethyl sulfoxide (DMSO) and methylsulfonylmethane (MSM) in the treatment of osteoarthritisOsteoarthritis Cartilage 2008; 16: 1277-88.
13. Kim Y, Kim D, Lim H, Baek D, Shin H. The anti-inflammatory effects of methylsulfonylmethane on lipopolysaccharide-induced inflammatory responses in murine macrophages. Biol Pharm Bull 2009; 32: 651-656.
1. ASGE Standards of Practice Committee. The role of endoscopy in the management of obscure GI bleeding. Gastrointest Endosc 2010; 72: 471-479. [ Links ]
2. Rockey D. occult and obscure gastrointestinal bleeding: causes and clinical management. Nat Rev Gastroenterol. Hepatol 2010; 7: 265-279. [ Links ]
3. Chen Y, Ma W, Chen J, Cai J. Multiple chronic non-specific ulcer of small intestine characterized by anemia and hypoalbuminemia. World J Gastroenterol 2010; 16: 782-784. [ Links ]
4. Freeman H. Multifocal stenosing ulceration of the small intestine. World J Gastroenterol 2009; 15: 4883-4885. [ Links ]
5. Zeino Z. Adverse effects of drugs on small intestine and colon. Best Pract Res Clin Gastroenterol 2010; 24: 133-141. [ Links ]
6. Higuchi K, Umegaki E, Watanabe T, Yoda Y, Morita E, Murano M. Present status and strategy of NSAIDs-induced small bowel injury. J Gastroenterol 2009; 44: 879-888. [ Links ]
7. Hayashi Y, Yamamoto H, Taguchi H, Sunada K, Miyata T, Yano T, Arashiro M, Sugano K. Nonsteroidal anti-inflammatory drug-induced small-bowel lesions identified by double-balloon endoscopy: endoscopic features of the lesions and endoscopic treatments for diaphragm disease. J Gastroenterol 2009; 44(Suppl XIX): 57-63. [ Links ]
8. Matsumoto T, Iida M, Matsui T, Yao T. Chronic nonspecific multiple ulcers of the small intestine: a proposal of the entity from Japanese gastroenterologists to Western enteroscopists. Gastrointest Endosc 2007; 66: S99-S107. [ Links ]
9. Chang D, Kim J, Choi H, Soo Eun C, Han D, Byeon J, Kim JO. Double balloon endoscopy in small intestinal Crohn's disease and other inflammatory diseases such as cryptogenic multifocal ulcerous stenosing enteritis (CMUSE). Gastrointest Endosc 2007; 66: S96-S98. [ Links ]
10. Anonymous. Methylsulfonylmethane (MSM). Monograph. Altern Med Rev 2003; 8: 438-41. [ Links ]
11. Brien S, Prescott P, Lewith G. Meta-analysis of the Related Nutritional Supplements Dimethyl Sulfoxide and Methylsulfonylmethane in the Treatment of Osteoarthritis of the Knee. Evid Based Complement Alternat Med 2009; 1-10. [ Links ]
12. Brien S, Prescott P, Bashir N, Lewith H, Lewith G. Review Systematic review of the nutritional supplements dimethyl sulfoxide (DMSO) and methylsulfonylmethane (MSM) in the treatment of osteoarthritisOsteoarthritis Cartilage 2008; 16: 1277-88. [ Links ]
13. Kim Y, Kim D, Lim H, Baek D, Shin H. The anti-inflammatory effects of methylsulfonylmethane on lipopolysaccharide-induced inflammatory responses in murine macrophages. Biol Pharm Bull 2009; 32: 651-656. [ Links ]

