










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.3 Bogotá Sept. 2011
Case report: Cecal ameboma as a complication of intestinal amebiasis
Héctor Adolfo Polanía Lizcano (1), Ronald Cabrera Díaz (2)
(1) Professor at the Universidad Surcolombiana-Neiva, Colombia.
(2) General Surgery Resident at the Universidad Surcolombiana. Neiva, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 25-03-11 Accepted: 02-08-11
Abstract
We report the case of a patient with cecum ameboma, an uncommon intestinal manifestation of amebiasis. Patient underwent surgery after an initial diagnosis of a perforated cecal neoplasm of an appendiceal adhesion mass. Histology confirmed the presence of trophozoites of E. Histolytica in an area of ulceration and necrosis of the cecum wall. While initially the ameboma was treated medically, clinical manifestations led to surgery with good evolution.
Key words
Ameboma, cecum, amebiasis.
INTRODUCTION
Amebiasis is one of the most frequent parasitosis worldwide, but its incidence is higher in developing and third world countries in which general levels of health are lower and where water potable water is not always available. Infections caused by E. histolytica are the second most common type of parasitosis in the world (Malaria is the first.), accounting for between 40,000 and 100,000 deaths annually (1, 2). The E. histolytica entamoeba invades the host tissue in trophozoite form and destroys the tissue by secreting proteins and capturing red blood cells. This leads to its most frequent clinical presentation of amebiasis (amebic dysentery or amebic colitis), but it can also appear in uncommon forms such as necrotic colitis, toxic megacolon, ulceration, perianal fistulas apart from ameboma (3, 4). For this case report we performed a systematic search of the literature from Latin America, Colombia, and elsewhere in the world and found very few reported cases. Most of the published information about this type of complication comes from Third World countries.
CLINICAL CASE PRESENTATION
A 53 year old female patient came to the urgent care clinic at the University Hospital of Neiva in Huila, Colombia. For five days she had suffered from epigastric pain and pain in the periumbilical region that radiated to the right iliac fossa and then became generalized abdominal pain. The patient also presented hyporexia and fever from an unknown cause. The patient had a clinical history of Type 2 diabetes mellitus and poorly controlled arterial hypertension. During the physical examination the patient's heart rate was 100 per minute and her arterial blood pressure was 140/80mmHg. Physical examination of the abdomen showed pain and the sensation of a mass in the right iliac fossa which led to a first approximate diagnosis approach of appendicitis complicated by a mass of appendiceal adhesions or a possible tumor of a perforated cecum. A complete blood count showed a leukocyte level of 18,900, neutrophils at 89%, lymphocytes at 4.8%, a platelet level of 24,1000, hemoglobin at 6.7gr/dl, PCR 28, creatinine at 1.48mg/dl, and ureic nitrogen at 24 mg/dl. We decided to transfuse 2 units of packed red blood cells per hour. Treatment began with 200mgs IV ciprofloxacin every 12 hours and 500 mgs IV metronidazole every 8 hours. A CAT scan showed the presence of a soft tissue injury located on the cecal wall. It reduced the intestinal diameter and was probably related to a neoplastic process (Figure 1).

Figure 1. Computerized axial tomography with contrast showing lesion in the cecal wall with dense soft tissue diminishing the diameter of the colon.
24 hours after admittance, the intensity of the patient's pain increased and was combined with involuntary abdominal defense. As this was compatible with acute abdomen requiring surgical treatment the patient underwent an exploratory laparotomy which found 500 cc of yellow liquid in 4 quadrants with a 15cm x 15cm hard mass in the cecum adhering to the right broad ligament of the uterus. A right radical hemicolectomy with a terminal lateral ileoileostomy using mechanical sutures was performed. During surgery we began to suspect that the patient suffered from cecal ameboma. Post-operative treatment continued with antibiotics. The oral route was reinitiated three days after surgery. Seven days after surgery the patient could tolerate eating soft foods and was discharged from the hospital. A review of the acid-Schiff (PAS) stain from pathology revealed severe amoebic colitis with ulceration and necrosis plus benign lymphoid hyperplasia, but there were no signs of malignancy (Figure 2).
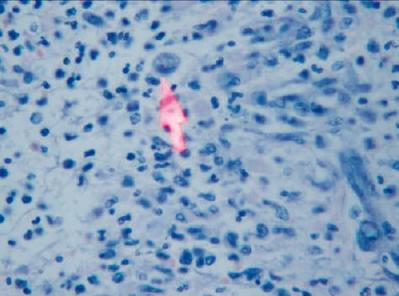
Figure 2. This microscopic view of the cecal wall after staining with hematoxylin-eosin dye shows severe inflammation and the presence of trophozoites compatible with severe amoebic colitis.
LITERATURE REVIEW
E. histolytica infections which cause amebiasis begin with ingestion of water contaminated with fecal matter containing cysts of the ameba (1). Trophozoites of the ameba are released into the lumen of the gastrointestinal tract where they rapidly clone themselves. This expanded trophozoite population later forms new cysts which perpetuate the cycle when they are excreted in the infected individuals feces (1,2,3). The infection can be located in any part of the intestine, but are most likely to be found in the cecum and the ascending colon (4, 5). Gastrointestinal presentations of E. histolytica infections range from asymptomatic (carrier) to colitis and the formation of abscesses and intestinal perforations. Amebiasis is common in developing countries in which up to 10% of the populations may be infected, but it is uncommon in developed countries. In 1991 The World Journal of Surgery published an article by Dr. Humberto Aristizabal on fulminating amoebic colitis in Colombia (6).
Since this infection's clinical manifestations are not specific, it is necessary to consider uncommon clinical presentations to make a correct diagnosis (7). It has been reported that 55% of all patients who present extracolonic amebiasis also present ulcers in the region of the ileocecal valve. These ulcers can be precursors to masses Generally this is due to repeated episodes of untreated or partially treated amebic colitis (8,9). Amebomas at the intestinal level are mostly located in the cecum and the ascending colon and can simulate colon carcinomas (10). Sometimes they appear as a mass with granulated tissue caused by a local infection of amoebas. Since this could be confused with a neoplastic lesion, it is epidemiologically important to consider this entity as a possibility in patients who present ileocecal masses in zones where E. histolytica infections are endemic (11,12). The diagnostic approach of ileocecal masses includes ruling out other infectious and noninfectious causes. Consequently, blood tests for entamoebas are required.
The bias of these tests is high since the serum levels of entamoebas may be elevated up to 1 year after the infection begins and because these tests do not distinguish between E histolytica infections and E dispar infections. Nevertheless, blood tests continue to be the test of choice in countries where infection is not prevalent (13).
Symptoms leading to differential diagnoses of amebomas include all ileocecal masses ranging from tubercolomas, lymphomas, appendicitis, and adenocarcinomas to those associated with Crohn's disease and infections by atypical fungi on to blood vessel malformations and diverticulitis (14). It has been calculated that 1.5% of all amebiasis infections result in the colonic masses called amebomas (15,16).
Considering that the majority of these lesions are discovered incidental to laparotomies, it is necessary to stress that this entity should be medically treated with tissue imidazole and luminal agents for 15 to 21 days (17, 18). It is vitally important to take a good clinical history and have a good diagnostic approach for suitable interpretation of endoscopic and radiologic images (19).
CONCLUSSIONS
Amebiasis and its complications continue to be a public health problem in our developing countries. The differential diagnosis of masses located in the right colon, (cecum and ascending colon) must include the possibility of amebomas, the diagnosis of which requires an early colonoscopy, histopathologic studies and blood tests to check for the presence of intestinal amebiasis. These measures can lead to early diagnosis and to suitable treatment.
REFERENCES
1. Stanley SL Jr. Amoebiasis. Lancet 2003; 361: 1025-34.
2. Huston CD. Intestinal Protozoa. En: Feldman, Sleisenger & Fordtran's Gastrointestinal and Liver Diseases, 8ª ed, Elsevier editors, Philadelphia, Pensylvania 2006. p. 2414-2435.
3. Cox FE. History of human parasitic diseases. Infect Dis Clin North Am 2004; 18: 171-88.
4. Martínez-Palomo A, Espinosa-Castellano M. Amebiasis and other protozoan infections. En: Cohen & Powderly. Infectious Diseases, 2nd ed., Philadelphia, Pensylvania, Elsevier editors 2004. p. 1567-71.
5. Sharma M, Vohra H, Bhasin D. Enhanced pro-inflammatory chemokine/cytokine response triggered by pathogenic Entamoeba histolytica: basis of invasive disease. Parasitology 2005; 131: 783-96.
6. Aristizábal H. Fulminant amebic colitis. Wld J Surg 1991; 15: 216-221.
7. Sharma D, Patel LK, Vaidya VV. Amoeboma of ascending colon with multiple amoebic liver abscesses. J Assoc Physicians India 2001; 49: 579-580.
8. L Rouas, M Amrani, A Reguragui, L Gamra, MA Belababbas. Diagnostic problems associated with intestinal amoeboma: case report. Med Trop 2004; 64: 176-178.
9. Rico HMA, Rodea RH. Ameboma de colon ascendente, reporte de caso. Cir Gen 2006; 28 suppl 1: S112.
10. DC Ng, SY Kwok, Y Cheng, CC Chung, MK Li. Colonic amoebic abscess mimicking carcinoma of the colon. Hong Kong Med J 2006; 12: 71-73.
11. Majeed SK, Ghazanfar A, Ashraf J. Cecal amoeboma simulating malignant neoplasia, ileocecal tuberculosis and Crohn's disease. J Coll Physicians Surg Pak 2003; 13: 116-7.
12. Guzman Valdivia Gomez G, Chavelas Lluck M, Medina González E. Unsuspected tumor of the colon. Rev Gastroenterol Mex 1996; 61: 362-3.
13. Radovanovic ZL, Katic VV, Nagorni AV, Zivkovic VV, Stankovic TD, Trenkic MS. Clinical diagnostic problems associated with cecal ameboma: case report and review of the literature. Pathol Res Pract 2007; 203: 823-5.
14. Simsek H, Elsurer R, Sokmensuer C, Balaban HY, Tatar G. Ameboma mimicking carcinoma of the cecum: case report. Gastrointest Endosc 2004; 59: 453-454.
15. Hardin RE, Ferzli GS, Zenilman ME, Gadangi PK, Bowne WB. Invasive amebiasis and ameboma formation presenting as a rectal mass: An uncommon case of malignant masquerade at a western medical center. World J Gastroenterol 2007; 13: 5659-60.
16. M Matsura, H Nakase, T Fujimori, Y Tsuda, T Chiba. Cecal ameboma. Gastrointest Endosc 2005; 62: 442-443.
17. Rodea-Rosas H, Athíe Gutiérrez C, Durán Padilla M, Montalvo-Jave Eduardo, Guizae-Bermúdez C. El comportamiento del ameboma en las últimas cuatro décadas. Experiencia en el Hospital General de México, OD. Rev Cir Gen 2008; 30: 70-73.
18. S Misra, V Misra, M Dwivedi. Ileocecal masses in patients with amebic liver abscess: etiology and management, World J. Gastroenterol 2006; 12: 1933-1936.
19. Ooi BS, Seow-Choen F. Endoscopic view of rectal amebiasis mimicking a carcinoma. Tech Coloproctol 2003; 7: 51-53.
1. Stanley SL Jr. Amoebiasis. Lancet 2003; 361: 1025-34. [ Links ]
2. Huston CD. Intestinal Protozoa. En: Feldman, Sleisenger & Fordtran's Gastrointestinal and Liver Diseases, 8a ed, Elsevier editors, Philadelphia, Pensylvania 2006. p. 2414-2435. [ Links ]
3. Cox FE. History of human parasitic diseases. Infect Dis Clin North Am 2004; 18: 171-88. [ Links ]
4. Martínez-Palomo A, Espinosa-Castellano M. Amebiasis and other protozoan infections. En: Cohen & Powderly. Infectious Diseases, 2nd ed., Philadelphia, Pensylvania, Elsevier editors 2004. p. 1567-71. [ Links ]
5. Sharma M, Vohra H, Bhasin D. Enhanced pro-inflammatory chemokine/cytokine response triggered by pathogenic Entamoeba histolytica: basis of invasive disease. Parasitology 2005; 131: 783-96. [ Links ]
6. Aristizábal H. Fulminant amebic colitis. Wld J Surg 1991; 15: 216-221. [ Links ]
7. Sharma D, Patel LK, Vaidya VV. Amoeboma of ascending colon with multiple amoebic liver abscesses. J Assoc Physicians India 2001; 49: 579-580. [ Links ]
8. L Rouas, M Amrani, A Reguragui, L Gamra, MA Belababbas. Diagnostic problems associated with intestinal amoeboma: case report. Med Trop 2004; 64: 176-178. [ Links ]
9. Rico HMA, Rodea RH. Ameboma de colon ascendente, reporte de caso. Cir Gen 2006; 28 suppl 1: S112. [ Links ]
10. DC Ng, SY Kwok, Y Cheng, CC Chung, MK Li. Colonic amoebic abscess mimicking carcinoma of the colon. Hong Kong Med J 2006; 12: 71-73. [ Links ]
11. Majeed SK, Ghazanfar A, Ashraf J. Cecal amoeboma simulating malignant neoplasia, ileocecal tuberculosis and Crohn's disease. J Coll Physicians Surg Pak 2003; 13: 116-7. [ Links ]
12. Guzman Valdivia Gomez G, Chavelas Lluck M, Medina González E. Unsuspected tumor of the colon. Rev Gastroenterol Mex 1996; 61: 362-3. [ Links ]
13. Radovanovic ZL, Katic VV, Nagorni AV, Zivkovic VV, Stankovic TD, Trenkic MS. Clinical diagnostic problems associated with cecal ameboma: case report and review of the literature. Pathol Res Pract 2007; 203: 823-5. [ Links ]
14. Simsek H, Elsurer R, Sokmensuer C, Balaban HY, Tatar G. Ameboma mimicking carcinoma of the cecum: case report. Gastrointest Endosc 2004; 59: 453-454. [ Links ]
15. Hardin RE, Ferzli GS, Zenilman ME, Gadangi PK, Bowne WB. Invasive amebiasis and ameboma formation presenting as a rectal mass: An uncommon case of malignant masquerade at a western medical center. World J Gastroenterol 2007; 13: 5659-60. [ Links ]
16. M Matsura, H Nakase, T Fujimori, Y Tsuda, T Chiba. Cecal ameboma. Gastrointest Endosc 2005; 62: 442-443. [ Links ]
17. Rodea-Rosas H, Athíe Gutiérrez C, Durán Padilla M, Montalvo-Jave Eduardo, Guizae-Bermúdez C. El comportamiento del ameboma en las últimas cuatro décadas. Experiencia en el Hospital General de México, OD. Rev Cir Gen 2008; 30: 70-73. [ Links ]
18. S Misra, V Misra, M Dwivedi. Ileocecal masses in patients with amebic liver abscess: etiology and management, World J. Gastroenterol 2006; 12: 1933-1936. [ Links ]
19. Ooi BS, Seow-Choen F. Endoscopic view of rectal amebiasis mimicking a carcinoma. Tech Coloproctol 2003; 7: 51-53. [ Links ]

