










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957versão On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.4 Bogotá out./dez. 2011
Proposed recommendations and guidelines for diagnosis of Hirschsprungs disease in mucosal and submucosal biopsies from the rectum
Lina Eugenia Jaramillo Barberi, MD. (1)
(1) Associate Professor at the Universidad Nacional de Colombia, Pathologist at the Fundación Hospital de La Misericordia in Bogotá, Colombia. millito59@hotmail.com
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 02-11-11 Accepted: 22-11-11
Abstract
Although constipation is common in children, most children have no structural disease, and only a small percentage of them have an organic cause for diseases such as intestinal dysganglionosis. Of these the most common is Hirschsprungs disease (HD), a disorder of the enteric nervous systems development characterized by the absence of ganglion cells in the distal colon that causes functional obstruction. A diagnosis is established by rectal biopsy which requires surgery.
In Colombia there are no clear guidelines for the study of these patients. This results in late diagnoses of almost half of the children with HD after one year of age. This article proposes recommendations and management guidelines for both the surgeon and the pathologist in an attempt to facilitate the study of patients with symptoms of constipation and suspected aganglionosis.
Key words
Constipation, rectal biopsies, intestinal dysganglionosis, ganglion cells, aganglionosis, Hirschsprungs disease.
INTRODUCTION
Chronic constipation is frequent among children; it is estimated that 8% suffer from chronic constipation at some point in their lives. Approximately 3% to 5% of pediatric consultations and 10% to 15% of gastroenterological consultations are due to chronic constipation (1). Most patients present functional constipation that can be managed by pediatricians. Patients with severe constipation must be checked for organic causes such as anatomical malformations, or endocrine, neurological, or metabolic disorders (2). Children that have suffered from constipation since the neonatal period, or whose constipation is unresponsive to treatment and persists with chronic symptoms, must be tested for enteric neuropathy and must have rectal biopsies taken.
Hirschsprungs disease (HD) is a disorder of the enteric nervous systems development characterized by the absence of ganglion cells in the distal colon that causes functional obstruction. Once a diagnosis is confirmed, basic treatment consists of the removal of the aganglionic segment and an anastomosis between the well innervated intestine and the distal rectum.
A clear understanding of the enteric nervous systems histology is necessary for diagnosis of this entity. There are three nervous plexuses: Auerbachs plexus, also known as the myenteric plexus, is located between the two layers of the muscularis propria, Henles plexus is located above the circular layer of the muscularis propria, and Meissners plexus, the most superficial, is located below the muscularis propria.
A biopsy of the mucosa and submucosa usually evaluates Meissners plexus but, when deep enough, can even sometimes include Henles plexus. A normal plexus is composed of neurons (ganglion cells) and supporting cells (glia). The characteristic histological finding of HD is a total absence of ganglion cells and an increase in structural density of the plexuses. Glial cells are replaced by Schwann cells, hypertrophy is present, and nerves look similar to peripheral nerves (3).
Diagnosis of HD continues to be a problem in this country because a large proportion of pathologists are uncomfortable doing this study because of the difficulty of evaluating material submitted by the surgeon. This is due to the absence of any guidelines to guarantee good performance of the biopsy. This report details some recommendations based on my experience of over 20 years in a pediatric hospital that has become a referral institution for this type of study.
From 2005 to 2009 we conducted 272 studies of children suspected of having HD: 106 were patients in our institution, and 166 were referrals for diagnosis or a second opinion. Most biopsies were from the mucosa and submucosa. The average level of biopsies per patient was 3.13 (2.3 to 5). During this period 56 patients were diagnosed with HD, equivalent to 20.58% (4). This is a high incidence compared to those reported in the literature (5). The most likely explanation for this is that our referral institution receives more cases than are in the general population. There were 44 boys and 12 girls with a ratio of 3.66: 1 which is similar to that described in the literature (5).
Publications of studies in industrialized countries report that more than two thirds of HD patients are diagnosed during the neonatal period and almost 95% before one year of age (5, 6). In our cases we found that, of the 56 patients diagnosed with HD, 44.64% were older than one year, 33.92% were between 1 and 11 months, and only 14.28% were neonates (7). The remaining 7.16% had no reference age listed. This reflects a problem in our diagnostic opportunity which is probably a mix of factors such as lack of consensus on the management of constipation by doctors, lack of criteria for rectal biopsies, and misleading or inaccurate reports obtained from the histopathological studies.
Our high volume of extra-institutional cases (61.03%) highlights a lack of confidence on the part of pediatric surgeons and general pathologists to undertake the study of patients with constipation. This in turn raises the need to develop a protocol for management of rectal biopsy material which would ensure proper orientation and emphasize the obligation of conducting broad and standardized series of pathology reports. For these reasons the objective of this review is to share my experience and make recommendations to facilitate the diagnosis of Hirschsprungs disease.
STEP BY STEP
One of the biggest responsibilities that we have when we conduct studies of rectal biopsies taken because of constipation is to guarantee that the material has been removed, cut, handled and fixed in the correct ways so that the probability of making a correct diagnosis is increased. To this end, there are tasks which are the responsibility of the surgeon, and others which are the responsibility of the pathologist.
The surgeon should obtain an adequate number of rectal biopsies which should all be of adequate size and depth. The surgeon should place them in a 10% formaldehyde solution. We recommend taking biopsies at three or more levels. Each biopsy should be properly marked to indicate at how many centimeters from the pectinate line it was taken.
The pathologist should
Orient and cut the specimens, and then request that the technician test a series of between 50 and 100 cuts stained with hematoxylin and eosin.
Evaluate the histological material and decide whether or not it is adequate. If its is not, the pathologist should report this.
The pathologist should clearly understand the classic signs of HD.
The pathologist should perform a differential diagnosis when appropriate.
None of the hospitals in this country use the histochemical staining technique for the acetylcholine esterase enzyme (AChE) as a marker for nerve fibers of the lamina propria and muscularis mucosa, even though this is considered by many to be the most important diagnostic tool for HD (8). Many institutions use only routine techniques, although increasing numbers of laboratories have access to the use of immunohistochemical markers that can occasionally be very useful even though in most cases they are not essential for diagnosis.
The key to the success of the study is to begin as soon as the sample is taken. In our institution we do not have suction biopsy equipment, so the material is obtained by transrectal biopsy conducted in operating rooms under general anesthesia. The patient is placed in a prone position, the rectum is dilated with a rectal speculum to expose its anterior wall, the biopsy level is chosen, a suture is stitched just below the mucosa, submucosa is pulled up, and the fragment is cut with scissors (Figure 1). The number of levels from which biopsies were taken varies in different schools. A little over a year ago, the surgeons in our institution by consensus to take biopsies from levels 3 and 5 levels at distances of 1,2,3,4 and 5 cm from the pectinate line. The biopsy size generally ranges from 0.3 to 0.5 cm which is sufficient if the sample is carefully handled. Our pathology service recommends that the surgeon avoid areas of the mucosa which look like they contain micronodules, as these samples are generally lymphoid aggregates occupying the submucosa and displacing Meissners plexus.
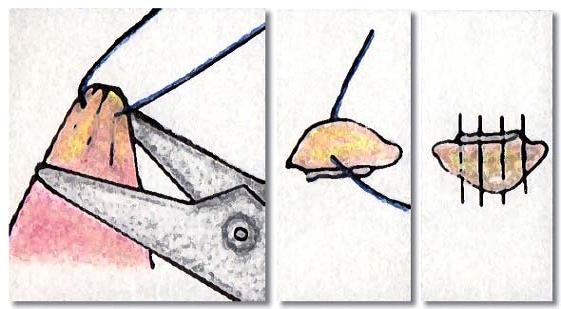
Figure 1. Taking the biopsy, identification and orientation of sample for cross sections.
Unlike routine biopsies in which the pathologists duties are limited to counting the fragments received, measuring them, and putting them into the processing cassettes, testing of biopsies taken for diagnosis of HD should be guided by a specialist. For these cases the layer necessary for diagnosis is the submucosa, so that guaranteeing that this tissue is well represented is vital. I recommend placing the fragment on a piece of paper with the mucosa side down. Then, stretch the tissue carefully so as not to crush it, and make as many parallel cuts as possible along the minor axis with distance between each cut of approximately 0.10 cm (Figure 2 and 3). The purpose of this procedure is to avoid to the extent possible oblique inclusions which contain very little of the submucosa, and to avoid samples of only the "head" which in which the observable tissue is either rectal mucosa or muscularis mucosa (Figure 4).

Figure 2. 0.5 cm endorectal biopsy including mucosa and submucosa.

Figure 3. Anterior view of specimen after cross sections.
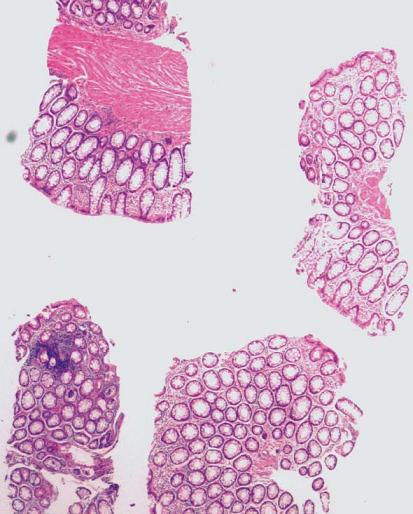
Figure 4. Material unsuitable for study of innervation because there is no submucosa to evaluate.
In our service technicians have already been shown Figures 2 and 3 and have been taught that for these samples, unlike other gastrointestinal tract biopsies, the key part to study is the submucosa. Given that the technician has already received guidance on the type of samples to be tested, we send the material order "For Innervation." This means cutting each block into two or three layers with an average of 12 to 15 slices cut from each of these layers (Figure 5). This result is between 60 and 120 slides per biopsy. It is important to order the series from the start to ensure that tissue is not wasted in mounting and remounting the slices. In most cases this is sufficient to diagnose or rule out aganglionosis. At the same time, usually is a small remnant of tissue in the block which can be used to add to the series in problematic cases or which can be tested with supplementary immunohistochemistry.

Figure 5. Perform examination of each level of transrectal biopsy sent for study.
It is important that a pathologist who is not an expert in HD to have clear concepts about the classic indications of this disease. You can not confuse, "I see no ganglion cells," with, "There are no ganglion cells." Since this is a disease the diagnosis of which is based on the absence of an element of histology, it is essential that the pathologist is sure that, both in terms of technology and knowledge, everything is consistent with aganglionosis. In general terms classical HD, i.e. short segment HD which occurs in 75% to 80% of cases, involves the distal sigmoid colon and rectum and is characterized histologically by nerve filaments which are large, thick, and compact. Nerve filaments are generally larger than 40 microns in diameter, and there are definitely no ganglion cells in these cases. If the filaments are few, small or lax, and do not look like neurons, it is valid to question the diagnosis and to suspect other diseases (3, 9). It is important to remember that long segment aganglionosis, especially total colonic aganglionosis, contrary to usual there can be decreased or nearly absent plexus. In these cases, as in almost all pathological studies, history and correlation are essential to guide the pathologist.
It is also vitally important to determine when a biopsy is insufficient or inadequate for diagnosis. Anatomically, the lower level of sampling is should be one or ideally 2 cms above the pectinate line. Biopsies which are very low or close to the anal sphincter may not have ganglion cells even when the patient does not have aganglionosis. When ganglion cells are not observed in a biopsy and there are islands of squamous epithelium or sphincter muscle fibers, it is the unequivocal signature that the sample was obtained from below the pectinate line. This should always be reported as a sample which is inadequate for diagnosis. If in doubt about the sampling site, I recommend making a note to remind the clinician and avoid misinterpretations. From the histological point of view a rectal biopsy is considered appropriate when the amounts of mucosa and muscularis mucosa together are equivalent in thickness to the amount of submucosa (Figure 6) (10). If the amount of submucosa in the sample is good, but it contains a lymphoid follicle, this must also be considered unsuitable for making a HD diagnosis (Figure 7). For any type of sample received, the pathologist should look judiciously at all cuts. Sometimes neurons can be identified in the periphery of the follicle, or immersed in the muscularis mucosa, in which cases aganglionosis can certainly be ruled out even when biopsies seemed inappropriate for the study (Figure 8).
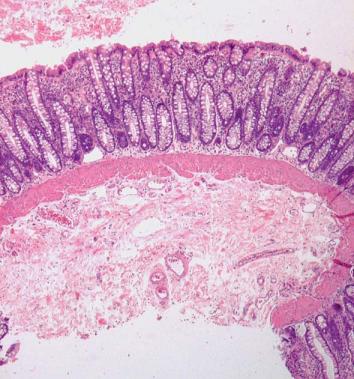
Figure 6. Adequate biopsy for study of innervation: the submucosal thickness is equivalent to the sum of the mucosa and muscularis mucosa (H&E 40X).
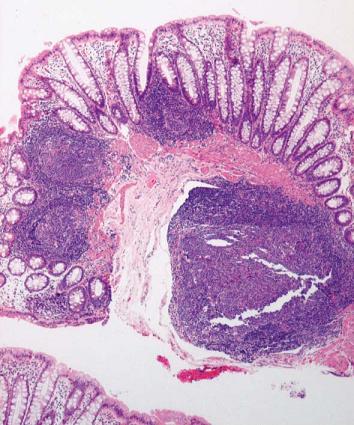
Figure 7. Material unsuitable for study of innervation: the submucosa is largely occupied by a very small lymphoid follicle tissue being evaluated (H&E 40X).
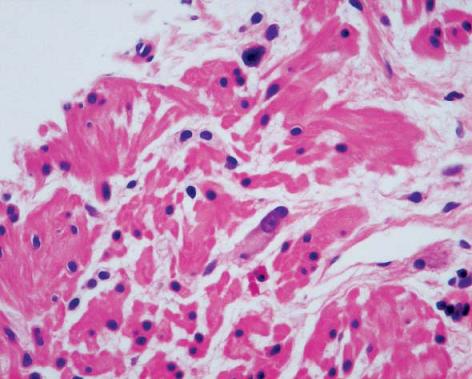
Figure 8. Ganglion cells observed in the middle of the muscularis mucosa ruling out diagnosis of Hirschsprung’s Disease (H & E 400X).
The easiest diagnosis to establish in biopsies of rectal mucosa-submucosa is that normal innervation is present. In fact, this is the most often seen case, and it can be confirmed with a review of just a few levels.
On the other hand, sometimes it is important to perform differential diagnoses. Mucosa-submucosa biopsies are not adequate to rule out entities such as myopathies or hypoganglionosis, but they do allow us to confirm diagnoses of immature plexuses and to cause us to suspect intestinal neuronal dysplasia (IND) (6, 7). This entity has generated much discussion. While some pathologists consider that it exists, others accept it only as a secondary disorder associated with intestinal motility problems such as HD. The most recent criteria determined that establishing a diagnosis of IND requires examination of at least 25 submucosal ganglions among which at least 20% must be giants having more than 8 ganglion cells in a cross-section. Taking biopsies 8 to 10 cm above the pectinate line is recommended. The criteria also specify that this diagnosis should never be made in children under 1 year of age (6). Within our institution, endo-rectal biopsies are almost never done at levels as high as 10 cm above the pectinate line. Therefore, when we find indications of "hyperganglionosis" in the submucosa of a patient who is over 1 year old, we refer the finding and suggest that it be correlated with clinical examination and radiology to rule out the possibility of IND. If it is appropriate, the surgeon then maps endorectal biopsies to obtain 5 at the same level in order to have the minimum number needed to confirm or rule out dysplasia.
Sometimes what we see is a very immature innervation pattern of ganglion cells similar to that seen in premature infants. These patterns are aggregated into rosette structures with minimal neuropils. Their morphology is different from that of mature neuron cells: they are smaller and bluish-gray, have darker nuclei, are eccentric, their nucleoli are not that prominent, and their cytoplasm is less elongated (11, 12). It is important to learn to recognize these cells and interpret them correctly in order to avoid misdiagnoses of aganglionosis (Figure 9).
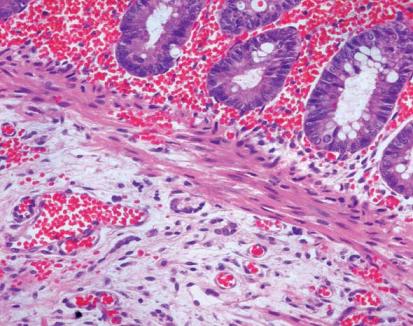
Figure 9. Immature ganglion cells arranged in rosette structures. Note that they have small eccentric nuclei and elongated gray-blue cytoplasm (H&E 200X).
When a series of slides from a good quality biopsy does not show ganglion cells, I do not recommend specific immunostaining studies for bcl-2 or NSE immunoreactive ganglion cells or for Schwann cells (Synaptophysin or S100) because the images are difficult to interpret (Figure 10). My opinion is that if in 60 to 120 levels no neurons were identified; it is unlikely that in two or three levels checked with immunohistochemistry we will be lucky enough to find clear and unequivocal evidence not seen in the series. When the issue is whether the cells observed are immature neurons or not, I believe that immunohistochemistry may help clarify the diagnosis. I recommend using conventional markers for neurons such as those already mentioned: bcl-2 or NSE immunoreactive ganglion cells.
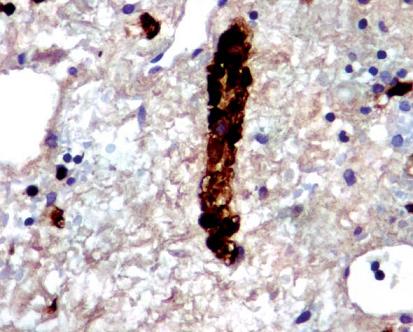
Figure 10. Immunohistochemistry with S100, marking equivocal and difficult to interpret (S100 400X).
Within the wide range of commercially available markers, I especially recommend calretinin, a calcium-binding protein involved in the signaling pathway that plays an important role in the organization and operation of the central nervous system (13). This marker is considered to be an alternative to the acetylcholinesterase technique (5, 8). It gives a positive pattern in patients who do not have the disease while it is negative or very weakly positive in cases of aganglionosis (Figures 11 and 12). In normal patients it is positive in the muscularis mucosa, in the lamina propria and in the submucosal plexus where it stains the Schwann cells and Bly highlights the nuclei of neurons. In cases of aganglionosis there may be discrete calretinin positivity in nerve fibers, but negativity in the muscularis mucosa, in the lamina propria and, of course, in the nuclei. Again, in these cases as in almost all pathology studies, immunohistochemistry should be interpreted in conjunction with hematoxylin and possible false positives or negatives taken into account.
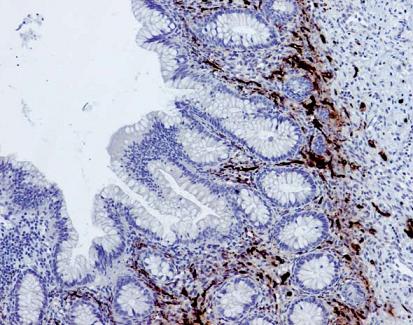
Figure 11. Calretinin immunohistochemistry in patients with normal innervation, marking positive lamina propria of the mucosa and Meissners muscular plexus (Calretinin 100X).
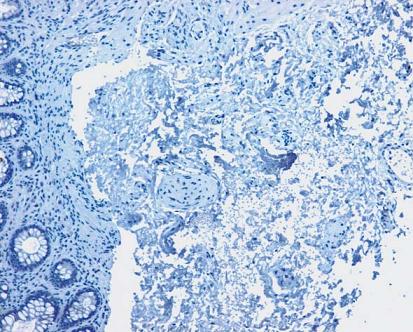
Figure 12. Calretinin immunohistochemistry in patients with Aganglionosis. Negative in the lamina propria of the mucosa and Meissners muscular plexus (Calretinin 100X).
CONCLUSIONS
Classically HD is histologically characterized by large, thick nerve fibers which are generally greater than 40 microns in diameter. They are compact and definitely have no ganglion cells. Observation of the histological picture in a series of 100 cuts on average is sufficiently specific to establish a diagnosis.
The presence of a few small, lax nerve fibers in the absence of ganglion cells must be evaluated with caution: it is prudent to suspect other diseases. It is important to remember that this image may correspond to rare types such as long-segment aganglionosis or total colon aganglionosis. In these cases, contrary to the usual, there may be decreased or near absence of plexuses.
The morphology of immature ganglion cells is different than that of mature cells. Immature cells have rosette structures only a minimum amount of neuropils. Learning how to recognize this is vital in order to avoid incorrect interpretations and misdiagnoses of aganglionosis.
Immunohistochemistry with conventional markers such as NSE and BCL2 neurons is useful when there is a serious doubt about whether the cells observed are immature neurons since positive results from these tests will confirm the diagnosis.
If the laboratory has access to calretinin, this is a simple and reliable method to help establish a diagnosis of HD. It is considered to be an alternative to the acetylcholinesterase technique. It results in a positive pattern in patients without the disease, but is negative or very weakly positive in cases of aganglionosis.
My final recommendation is that we must not forget our responsibilities as pathologists when confirm or rule out a diagnosis of HD. Mortality rates from untreated aganglionic megacolon among children are as high as 80%. Mortality rates among patients treated surgically are generally very low, although there are many complications. These include stenosis or leakage from the anastomosis, intestinal obstructions, pelvic abscesses or lesions, incontinence, and enterocolitis. It is a grave mistake not to diagnose the disease, but the picture is not better when a false diagnosis of HD is made since the patient will not only be subject to the risk of surgery, but his or her real condition will not be treated while there may be a number of complications from the intervention that could even cause death.
REFERENCES
1. Masi P, Miele E, Staiano A. Pediatric anorectal disorders. Gastroenterol Clin North Am 2008; 37: 709-730.
2. Khan AR, Vujanic GM, Huddart S. The constipated child: how likely is Hirschsprungs disease? Pediatr Surg Int 2003; 19: 439-442.
3. Montedonico S. Constipación crónica y desordenes de los plexos entéricos. Rev Med Clin Condes 2009; 20: 805-806.
4. López T. JC, Jaramillo B, LE. Papel o utilidad de la biopsia rectal en el estudio del paciente pediátrico con estreñimiento. Experiencia de cinco años en un centro de referencia colombiano 2011. Pendiente publicación.
5. De Lorijn F, Reitsma JB, Voskuijl WP, Aronson DC, Ten FJ Kate, Smets AM, Taminiau JA, Benninga M. Diagnosis of Hirschsprungs Disease: A Prospective, Comparative Accuracy Study of Common Tests. J Pediatr 2005; 146: 787-92.
6. Meier-Ruge W. Bruder E, Kapur RP. Intestinal Neuronal Dysplasia Type B: One Giant Ganglion is Not Good Enough. Pediatric and Developmental Pathology 2006; 9: 444-452.
7. Feichter S., Meier-Ruge WA, Bruderb E. The histopathology of gastrointestinal motility disorders in children. Seminars in Pediatric Surgery 2009; 18: 206-211.
8. Wakely PE Jr, McAdams AJ. Acetylcholinesterase histochemistry and the diagnosis of Hirschsprungs disease: a 3 1/2-year experience. Pediatr Pathol 1984; 2(1): 35-46.
9. Puri. Variant Hirschsprung´s Disease. Journal of Pediatric Surgery 1997; 32(2): 149-157.
10. Qualman SJ, Jaffe R, Bove KE. Monforte-Muñoz H. Diagnosis of Hirschsprung Disease Using the Rectal Biopsy: Multi-institutional Survey. Pediatric and Developmental Pathology, 1999; 2: 588-596.
11. Ariel I, Vinograd I, Lernau OZ et al. Rectal mucosal biopsy in Aganglionosis and allied conditions. Hum Pathol 1983; 14: 991-995.
12. Venugopal S, Mancer K, Shandling B. The validity of rectal biopsy in relation to morphology and distribution of ganglion cells. J Pediatric Surg 1981; 16: 433-437.
13. Guinard-Samuel V, Bonnard A, De Lagausie P, et al. Calretinin immunohistochemistry: a simple and efficient tool to diagnose Hirschsprung disease. Modern Pathology 2009; 22: 1379-1384.
1. Masi P, Miele E, Staiano A. Pediatric anorectal disorders. Gastroenterol Clin North Am 2008; 37: 709-730. [ Links ]
2. Khan AR, Vujanic GM, Huddart S. The constipated child: how likely is Hirschsprungs disease? Pediatr Surg Int 2003; 19: 439-442. [ Links ]
3. Montedonico S. Constipación crónica y desordenes de los plexos entéricos. Rev Med Clin Condes 2009; 20: 805-806. [ Links ]
4. López T. JC, Jaramillo B, LE. Papel o utilidad de la biopsia rectal en el estudio del paciente pediátrico con estreñimiento. Experiencia de cinco años en un centro de referencia colombiano 2011. Pendiente publicación. [ Links ]
5. De Lorijn F, Reitsma JB, Voskuijl WP, Aronson DC, Ten FJ Kate, Smets AM, Taminiau JA, Benninga M. Diagnosis of Hirschsprungs Disease: A Prospective, Comparative Accuracy Study of Common Tests. J Pediatr 2005; 146: 787-92. [ Links ]
6. Meier-Ruge W. Bruder E, Kapur RP. Intestinal Neuronal Dysplasia Type B: One Giant Ganglion is Not Good Enough. Pediatric and Developmental Pathology 2006; 9: 444-452. [ Links ]
7. Feichter S., Meier-Ruge WA, Bruderb E. The histopathology of gastrointestinal motility disorders in children. Seminars in Pediatric Surgery 2009; 18: 206-211. [ Links ]
8. Wakely PE Jr, McAdams AJ. Acetylcholinesterase histochemistry and the diagnosis of Hirschsprungs disease: a 3 1/2-year experience. Pediatr Pathol 1984; 2(1): 35-46. [ Links ]
9. Puri. Variant Hirschsprung´s Disease. Journal of Pediatric Surgery 1997; 32(2): 149-157. [ Links ]
10. Qualman SJ, Jaffe R, Bove KE. Monforte-Muñoz H. Diagnosis of Hirschsprung Disease Using the Rectal Biopsy: Multi-institutional Survey. Pediatric and Developmental Pathology, 1999; 2: 588-596. [ Links ]
11. Ariel I, Vinograd I, Lernau OZ et al. Rectal mucosal biopsy in Aganglionosis and allied conditions. Hum Pathol 1983; 14: 991-995. [ Links ]
12. Venugopal S, Mancer K, Shandling B. The validity of rectal biopsy in relation to morphology and distribution of ganglion cells. J Pediatric Surg 1981; 16: 433-437. [ Links ]
13. Guinard-Samuel V, Bonnard A, De Lagausie P, et al. Calretinin immunohistochemistry: a simple and efficient tool to diagnose Hirschsprung disease. Modern Pathology 2009; 22: 1379-1384. [ Links ]

