










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev Col Gastroenterol v.26 n.4 Bogotá oct./dic. 2011
Aggressive angiomyxoma in men: Clinical case report and literature review
Juan Fernando Medina R., MD (1), Javier A. Carrera S. MD (2), Heinz O. Ibáñez, MD (2), Carlos E. Martínez J., MD (2)
(1) Coloproctology Fellow at the Universidad Militar" Nueva Granada" Hospital Militar Central in Bogotá, Colombia.
(2) Coloproctologists in the Coloproctology Program of the Universidad Militar"Nueva Granada" and in the Coloproctology Service of Hospital Militar Central in Bogotá, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 10-02-11 Accepted: 11-10-11
Abstract
We report a case of a male patient with an aggressive angiomyxoma located in the presacral space which was diagnosed and clinically treated at the Hospital Militar Central in Bogotá, Colombia. Kraskes posterior approach was used to completely excise the lesion with minimal functional and aesthetic impact on the patient. Aggressive angiomyxomas are extremely rare. They are most commonly found in pelvic locations in women. They are even more exotic in men, with very few cases reported in the literature. Management requires complete removal of the lesion and the clinical and imaging follow-up given their high rate of recurrence.
Key words
Aggressive angiomyxoma, presacral tumor, Kraskes approach.
INTRODUCTION
Aggressive angiomyxoma (AA) is a rare pelvic soft-tissue tumor often found in the perineum which originates from myocardial fibroblasts. It is locally aggressive and metastasizes quickly and easily. First described in 1983 by Steeper and Rosai in the soft tissues of the pelvis and perineum of premenopausal women, these tumors appear to be benign in cytology, composed of spindle and star cells embedded in a myxoid matrix containing medium caliber vessels. Nevertheless, despite their cytologically harmless appearance, they are infiltrating tumors with high risks of recurrence (1, 3, 5-7).
Because they are rare, their incidence has not been clearly established (1), but about 190 cases have been described in the medical literature to date. Of these approximately 150 have been reported in premenopausal women from 30 to 40 years of age and 40 cases have been reported in men (4, 5, 7, 12). Of these cases only about 70 have had been located in the pelvis or in retroperitoneal locations (3). It has been established that fewer than 150 of the cases were reported in the English language literature between 1983 and 2004 (2). In 2007 fifteen additional cases in were described men in the English and five more in Spanish-language literature (1). Incidence and reports of the disease have been increasing each year (12).
The entity occurs at least 7 times more often among women as it does among men. It has been reported in male and female children as young as 2 years old (2, 3, 5). It is most frequently found in the scrotum, perineum, groin, pelvis and spermatic cord (1). In women it is most commonly found in the perineum and pelvic organs including the bladder and uterus (3).
CASE REPORT
A 58 year old male patient came to the Hospital Militar Central in Bogotá, Colombia because of a single episode of inflamed lower rectal bleeding which had stopped without treatment. This incident followed 2 years of slow growth of a mass at right gluteus level adjacent to the posterior midline. The initial physical examination confirmed the presence of a soft 8 x 5 cm mass with ill-defined edges in the right central gluteus.
A distal rectal examination showed a firm mass attached to the right side of the distal rectum without infiltration. A total colonoscopy found nothing else of note and ruled out other lesions as explanations of the single episode of self-limiting rectal bleeding.
An abdominal-pelvic MRI showed the presence of an 8.8 x 5.5 cm tumor with well-defined edges located in the pelvis. This established the diagnosis of a presacral tumor (Figure 1).

Figure 1. Recognition of presacral lesion by MRI.
Given the location and the definition of the lesions its edges shown in images, surgical management using an approach that would reach the tumor while maintaining the sphincter integrity was needed. Consequently, Kraskes technique was selected (Figures 2 and 3).
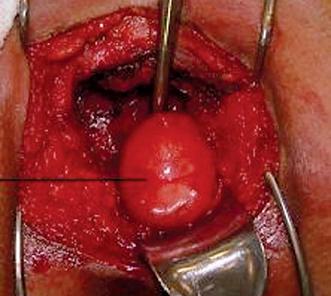
Figure 2. Presentation of the presacral tumor after performing digital dissection of retrorectal space.
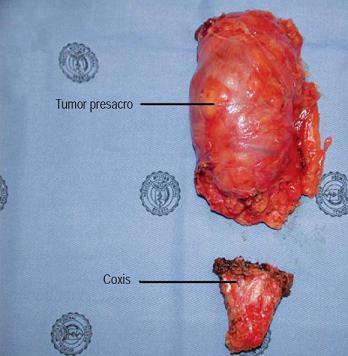
Figure 3. Presacral lesion after extraction.
The official pathology report showed:
Macroscopic examination:
- Soft 11.5 x 7 x 4 inch mass weighing 188 grams with superficial vascular congestion and parenchymal appearance. Mucoid and whirling after cutting
Microscopy:
- Mesenchymal tumor composed of spindle cells and stellate cells in myxoid stroma with abundant blood vessels. Mitosis was not observed.
Immunohistochemistry:
- Positive for actin, vimentin and desmin
- Negative for estrogens and progestin
- Negative for Ki67 and S100
- Positive in vessels for CD 34
Pathological diagnosis of retrorectal mass:
- Mesenchymal tumor compatible with aggressive angiomyxoma.
Currently the patient has completed 8 months without disease and remains under clinical monitoring by the Coloproctology and Oncology services of the hospital. Monitoring includes periodic MRI imaging which has ruled out tumor recurrence to date. Cosmetic results are satisfactory as a consequence of the approach selected, and there are no alterations in anorectal continence.
DISCUSSION
Aggressive angiomyxoma was first described in 1983 by Steeper and Rosai as a locally infiltrative benign mesenchymal neoplasm. They described it as having a predilection for the soft tissues of the pelvis and perineum of young women and of being aggressive in the sense of having high frequencies of local recurrence even after adequate initial treatment (1-7, 9). About 2 years later Begin published his experience with 9 patients which included the first report of this entity among men (5).
This is a relatively rare tumor that most surgeons will not find in their careers (8), and the fact that the case presented here is that of a male patient reinforces its unusual nature (10).
PATHOGENESIS
Although currently aggressive angiomyxomas causes, incidence and pathogenesis are unknown (1-3), some articles have considered that origin in isolated mesenchymal cells is a possibility (3, 5). From the standpoint of histogenesis as shown through electron microscopy, tissue cultures and immunohistochemical and ultrastructural analysis, these lesions originate in fibroblasts or myofibroblasts in the area of the perineum and/or pelvis. This is the best accepted hypothesis for their origins (1, 3, 6, 10). Given the most common ages at presentation, a hormonal cause has also been proposed for aggressive angiomyxomas pathogenesis. Nevertheless, the wide reported age range of patients and onset in males theoretically limits the possibility of a hormone dependent cause (3, 4, 7, 10).
HISTOLOGY
Microscopically, these tumors have low to moderate cellularity. Their mesenchymal neoplastic cells are hyperchromatic with dense homogeneous chromatin. There are occasional nucleoli and very little mitosis occurs. In addition they tend to have fusiform or stellate morphology with relatively scarce eosinophilic cytoplasm in a myxoid base. Blood vessels are medium size and large with a variety of secondary changes including medial hypertrophy and fibrointimal proliferation scattered throughout the tumor forming a thick hyalinized wall. Although evidence of infiltration can be seen by the entrapment of fat, muscle and/or medium-sized nerve bundles, the proliferative vascular pattern seen in most soft tissue tumors has not been reported in angiomyxoma (4-6, 9, 10).
CYTOGENETIC ANALYSIS
Cytogenetic analysis of the 7 female cases reported at that time showed karyotype abnormalities associated with a translocation in the 12q14-15 region and even the loss of an X chromosome. This translocation produces an aberrant expression of the HMGA2 (aka HMGIC) gene. This gene is an architectural transcription factor that is primarily expressed during embryogenesis and is a member of the High Mobility (High Mobility Group-HMG) of proteins. Although this finding initially suggested the use of the HMGA2 gene as a marker for this malignancy, the idea was rejected because the translocation is often shared by other mesenchymal tumors such as uterine leiomyomas, lipomas, pulmonary hamartomas, liposarcomas, and hemangiopericytomas. Currently this translocation is considered to be the most common chromosomal abnormality associated with the emergence of human mesenchymal neoplasms, and thus HMGA2 cannot be used as a specific marker for aggressive angiomyxoma. Nevertheless, it has been suggested that it can be used for evaluation of margins and in the detection of small foci of residual tumor excisions or recurrences. Until we have more information these chromosomal findings are not uniform in any way, but rather mere curiosities (1-3, 10, 11, 14, 17-19).
IMMUNOHISTOCHEMISTRY
Although there are no known markers specific to aggressive angiomyxoma (10, 11), immunohistochemical study can establish that tumor cells are positive for vimentin and desmin (100%), variably positivity for smooth muscle specific actin (94%), for estrogen receptors (93%) and for progesterone receptors (90%) and for CD34. These cells test negative for S100 protein, chromogranin, Ki-67 and factor VIII (1, 3-6, 10, 11, 13).
Male patients may test positive for estrogen and progesterone receptors (11). In differential diagnosis among angiomyxoma, myxoid liposarcoma and myxoma for these patients, patients with angiomyxoma should test positive for vimentin and negative for S-100 protein (14).
MACROSCOPIC EXAMINATION
Macroscopically, tumors are usually firm or gelatinous with diameters of 10 cm or more. They are whitish with pink or red outer surfaces and gray colored cross sections resulting from myxoid stroma that is rich in collagen fibers. Their content is mucoid or watery, encapsulation is either poor or absent content, and their architecture is with relatively sharp margins in some areas and adherence or infiltration of fat, fibrous tissue and/or muscle in other areas. Some cases have been reported with diffusely infiltrative margins. During examination exceptional cases have presented hemorrhaging or necrosing tissue, while other cases are encapsulated and well circumscribed (3-7, 10).
Angiomyxomas heterogeneous appearance does not allow for macroscopic tissue diagnosis, so histopathologic examination is almost always necessary to establish the diagnosis (6).
DIFFERENTIAL DIAGNOSIS
Given their propensity for local recurrence, differential diagnoses should be done for multiple benign myxoid lesions, even though clinical, microscopic and immunohistochemical characteristics are shared by several types of tumors. It is important to differentiate angiomyxoma from angiomyofibroblastoma of the vulva which shares histogenic features with it. In fact, this suggests the possibility that these two lesions are related and possibly derived from a primitive mesenchymal cell normally found in the female genital tract which has the capacity of myofibroblastic differentiation. Nevertheless, angiomyxoma, unlike angiomyofibroblastoma, tests positive for factor VIII and negative for smooth muscle actin (3, 4, 7).
In addition to angiomyofibroblastoma, other myxoid tumors are lipomas, intramuscular types myxomas, juxta-articular myxoid leiomyoma, pelvic fibromatosis, low-grade malignant myxoid sarcoma (myxoid liposarcoma) and low-grade malignant myxoid fibrous histiocytoma (myxofibrosarcoma) (3-5, 7, 10, 12).
CLINICAL PRESENTATION
Aggressive angiomyxoma occurs much more frequently among women than in men, among whom it is rare. Its underlying mechanisms are still under study (2). To date only 40 cases among men have been published (4, 10, 13).
The female to male ratio is approximately 6.6:1.8 (2, 5, 6, 10) with some reports putting it as high as 15:2 (4, 7). While its age distribution has a wide range, it occurs most frequently between ages 18 and 63 with peak incidence during the reproductive years from the second to fourth decades of life. A patient of 2 years old is the youngest reported in the literature to date (2, 5-7, 10). These tumors usually occur at later ages among men, between the third and fifth decade of life with an average age of 46 years (2, 11, 15).
Typically angiomyxoma is a slow growing locally infiltrative lesion, but it is not invasive or capped (10, 13). Its size varies from 1 cm to 60 cm, but is commonly larger than 10 cm. It presents symptoms related to compression of adjacent organs since there is no direct invasion (6, 7, 10, 13).
In general, these lesions occur in the pelvis, perineum and inguinal region (96.77%) among both men and women. To date few cases have been described in sites other than these areas (2, 4, 7, 10). Physical examination often underestimates the total extent of angiomyxoma except for cases of small vaginal or vulvar lesions (6). Extension from the perineum into the pelvis is common and often unnoticed clinically (9).
Among men, sites which are frequently involved include the scrotum (38%), the spermatic cord (33%), the perineum region (13%) and the groin. There are also reports of cases in the retrovesical region, prostate and epididymis (5, 7, 10, 11, 13). Among women sites which are frequently involved include the vulva, the vagina, the groin, the buttocks and the peritoneum, but it has also been described in the oral cavity, the uterus, the cervix, the bladder and the pararenal space (4, 7, 10). Since tumors are usually large, contiguous involvement of several sites is common (5).
This uncommon neoplasm presents no typical universal symptoms but rather presents a wide variety of clinical signs (2). Among female patients it usually presents as a long lasting mass accompanied by perineal, labial or pelvic pains similar to pulsating pressures. Patients experience dyspareunia and a sensation of mass in the pelvis or abdomen which increases when heavy objects are lifted (5, 6).
Consequently, most cases are diagnosed incidentally, even though preoperative recognition is often quite difficult because of the rarity of the condition. Mistaken diagnoses are made in approximately 82% of cases (2, 3, 6, 7). In these cases aggressive angiomyxoma is often confused with Bartholins cysts, vulvar abscesses, vaginal cysts, lipomas, vaginal prolapse, pelvic floor hernias (sphincter muscles of the anus), vaginal masses or polyps, liposarcomas, fibrosarcomas, botryoid sarcomas, vulgar masses and inguinal hernias (1, 2, 6, 7, 10). In other cases the diagnosis of angiomyxoma is only made by the pathologist after resection of a misdiagnosed pelvic mass (6).
Although its features are benign, two cases with distant metastasis in women for whom aggressive angiomyxoma was fatal have been described. The evolution of the disease in one of these patients took 10 years from diagnosis while in the other it took 27 years. This suggests that clinical follow-up should be done for all cases (1, 2, 4, 7, 10).
The rate of local recurrence is very high, varying between 36% and 83% of cases. Most are diagnosed in the first two to three years after initial surgery with average recurrence time between 9 and 14 months following surgery (2, 4-7, 9, 11, 12, 14). Nevertheless, there have been reports of recurrences occurring up to 17 years after initial surgery. The earliest reported recurrence happened just two months after initial surgery (6, 10, 12).
This high recurrence rate has been attributed to incomplete surgical excision since residual tumors are the main determinant of recurrence (2, 9, 10). Among men, there seems to be less local recurrence (approximately 20% of cases compared to 50% among women). This is probably because complete resection is easier in the paratesticular region of men than in the pelvis and perineum of women (1). Other reports estimate that this lesion recurs in approximately 9% of male cases. There have been no reports of metastasis among men to date (13).
Two factors may contribute to the high rate of local recurrence. First, the tumor may not have been diagnosed prior to initial surgery, and the extent of the tumor may not be perceived. Second, the strategic location of the tumor around the urethra, vagina, anal sphincter and rectum with extensions above and below the pelvic diaphragm makes complete resection difficult and does not allow either an exclusively abdominal or an exclusively perineal approach. For these reasons, most recurrences are related to inadequate resection and the presence of residual tumor (9).
However, there are series of cases which have reported no differences in rates of recurrence among patients with negative surgical margins and those with positive margins. This has created some controversy over whether surgical margins are associated with recurrence, but the results of these reports have not been possible to reproduce (2, 16).
Given these characteristics, the diagnosis must be made according to clinical suspicion supported by CAT scan or MRI. A biopsy is mandatory to confirm the diagnosis as final recognition is based on histopathologic and immunohistochemical studies and because confirmation is necessary to avoid potentially disfiguring procedures (2-4, 6).
IMAGING
Imaging tests such as pelvic and rectal ultrasound, computed axial tomography (CAT scans) and magnetic resonance imaging (MRI) provide useful clues for diagnosis of this disease (2, 6). Intravenous pyelograms, marrow scintigraphy, barium enemas and pelvic angiography have also been used to assess the extent of the lesion before surgery (6).
Ultrasound may show a well-defined hypoechoic mass with thin multiple internal echogenic septa with frankly cystic appearance (2, 9, 10). Angiography usually reveals a hypervascular mass occasionally accompanied by feeder vessels (9, 13).
CAT scans show tumors with well defined margins and lower attenuation than muscles while MRIs characteristically show high signal intensity. Both of these radiological features are secondary to the loose myxoid matrix and high water content of these lesions (2, 6, 9, 10). Another important characteristic is that these lesions form masses that displace rather than infiltrate adjacent structures (3, 9).
MRIs are preferable to CAT scans because of their better tissue characterization and lack of ionizing radiation. Consequently MRIs are the method of choice for monitoring and controlling possible recurrences (2, 3, 6, 7, 9, 10, 12).
The use of CAT scans or MRIs is essential for definition of tumor size especially since size is usually not clinically apparent in cases where there are extensions from the perineum into the pelvis. These cases are very common, and often unexpected. Both studies can accurately determine the extent (invasive edge) and the relationship to adjacent organs of the tumor and whether or not the tumor passes through the pelvic diaphragm. This is key to determining the choice of surgical approach (either perineal, abdominal, or both) in order not to leave residual tumor (2, 6, 9).
SURGERY
Surgery is undoubtedly the most important radical method for treating this disease. Complete resection is considered to be the treatment of choice for primary tumors and for recurrences (2-4, 6, 7, 10).
Including broad free margins around the tumor in the area of resection should be the first step in preventing recurrences of this lesions, although this depends on tumor size, location and the presence or absence of disease within the surgical margin (1, 2, 6, 8).
Laparoscopic surgery for pelvic tumors in the ischioanal area has been reported. The rectum is fully mobilized to the plane of the elevators muscles, and then the mass in adjacent planes is dissected. A small incision in the right perianal margin is made to remove the last adhesions and the resected piece (7).
FOLLOW-UP
Follow-up examinations at intervals of one to two years in which ultrasound and MRI examinations are alternated are sufficient, given the slow growth and low likelihood of metastasis of this tumor (3). Nevertheless, longer-term follow-up using the same studies should be considered (11, 14).
ADYUVANT THERAPY
The cells of this neoplasm typically express estrogen and progesterone receptors which suggests hormonal influence on the development and growth of the lesion and that the angiomyxoma may arise from specialized cells of the stroma of the perineum. This could explain why these tumors occur most frequently during reproductive age. This feature has been used for preoperative endocrine therapy which has achieved reduction of tumor size in several reported cases (2, 5, 7, 8, 10).
Many studies have described encouraging results from the use of a single monthly 3.75 mg injection of leuprolide acetate, an agonist of gonadotropin-releasing hormone (GnRH), for treatment of these lesions in women. Lesions disappear or their size, as measured clinically and with imaging, decreases within three months to a year. Results depend on the size of the lesion and on whether it is a primary or secondary tumor. Clinically measurable response requires 3 to 4 months (2, 6, 10, 14, 16).
However GnRH agonists are used primarily mainly as adjuvant therapy for residual or recurrent tumors among patients who are poor candidates for surgery (or for those who refuse surgery) but who test positively for estrogen and progestin receptors, independently of the strength of that positivity (2, 6, 7). In the absence of sufficient studies hormone therapy cannot replace surgery. Moreover, long-term treatment with GnRH agonists may induce adverse effects such as osteoporosis and depression even among young women. This has led some authors to propose intermittent dosages of leuprolide (2, 4, 6, 8, 16).
Whether or androgen agonists should be used to treat male patients who test positive for androgen receptors has not yet been determined (2).
The use of oral doses of 25 mg/day of Aromasin, an aromatase inhibitor, has been reported for the medical treatment of aggressive angiomyxoma. It reduces high levels of circulating estrogen and prevents conversion of endogenous estrogen and has achieved tumor volume reduction from transverse measurements of 8.7cm x 5.5 cm to 6.3cm x 3.2 cm. Administered prior to surgery it reduces tumor extension and thus reduces resulting morbidity (2, 8).
In light of current knowledge, the role of hormonal therapy in the management of this particular tumor remains to be determined (5). Chemotherapy and radiation therapy are considered to be inadequate adjuvant therapies following surgical removal of aggressive angiomyxoma due to the low mitotic activity of neoplastic cells and because angiomyxoma has almost no potential for metastasis (2, 4, 6, 7, 10).
CONCLUSIONS
Soft tissue aggressive angiomyxoma is associated with a high risk of local recurrence after removal, but metastasis is almost unheard of. It most frequently involves the pelvic and perineal region of women during reproductive age and is uncommon among men. It should be considered in the differential diagnosis of any mass with perineal symptoms in female patients of childbearing age.
MRIs, CAT scans or pelvic ultrasound examinations are recommended for initial imaging of any pelvic-perineal-inguinal mass. Complete excision of the lesion with wide surgical margins is the treatment of choice. Also, due to the high rate of local recurrence, follow-up examinations with MRI and ultrasound alternating at intervals of one to two years should be sufficient.
Case reports suggest that medical treatment with GnRH agonists are a viable option for both primary and recurrent tumors, especially given the radical and often debilitating nature of the surgery required to remove the tumor. Further evidence is required to establish the true value of this treatment.
REFERENCES
1. Martínez AA, Hernández-González M, Carrera González E. Angiomixoma agresivo en hombres. Rev Med Hosp Gen Mex 2007; 70(2): 78-81.
2. Jingping Z, Chunfu Z. Clinical Experiences on Aggressive Angiomyxoma in China (Report of 93 Cases). Int J Gynecol Cancer 2010; 20: 303-307.
3. Adwan H, Patel B, Kamel D, Glazer G. A solitary encapsulated pelvic aggressive angiomyxoma. Ann R Coll Surg Engl 2004; 86: W1-3.
4. Camps Lasa J, Navarro Luna A, Muñoz Duyos A, García Domingo M, Molina CM. Angiomixoma agresivo pelviperineal en el varón. Cir Esp 2008; 84(2): 101-11.
5. Hastak MS, Raghuvanshi SR, Sahu S, Vyankatesh A, Ramraje SN, Ranjan A. Aggressive Angiomyxoma in men. JAPI 2008; 56: 373-5.
6. Boren T, Lapolla J, Martino M, Nirgudkar P. Aggressive Angiomyxoma: A Case of Multiple Recurrences and Review of the Literature. Journal of Pelvic Medicine & Surgery 2006; 12: 151-6.
7. Mera Velasco S, Cabello Burgos AJ, Ruiz López M, González Poveday I, Santoyo Santoyo J. Resección laparoscópica de angiomixoma pélvico agresivo. CIR ESP. 2010; 88(2): 119-132.
8. Giles DL, Liu PT, Lidner TK, Magtibay PM. Treatment of aggressive angiomyxoma with aromatase inhibitor prior to surgical resection. International Journal of Gynecological Cancer 2007; 8: 369-385.
9. Outwater EK, Marchetto BE, Wagner BJ, Siegelman ES. Aggressive Angiomyxoma: Findings on CT and MR imaging. AJR 1999; 172: 435-438.
10. Xambre L, Cerqueira M, Guimarães I. Angiomixoma agresivo penoescrotal. Actas Urológicas Españolas 2009; 33(3): 321-326.
11. Kondo T. Aggressive angiomyxoma in the inguinal region: a case report. Journal of Medical Case Reports 2010; 4: 396.
12. Wu Ch, Shei-Dei S, Chin D. Scrotal aggressive angiomyxoma mimicking inguinal hernia. Asian J Androl 2007; 9: 1-3.
13. Kidric D, MacLennan G. Aggressive Angiomyxoma of the Male Genital Region. The Journal of Urology 2008; 180: 1506.
14. Morag R, Fridman E, Mor Y. Aggressive Angiomyxoma of the Scrotum Mimicking Huge Hydrocele: Case Report and Literature Review. Case Reports in Medicine. 2009. p. 1-3.
15. Andres LA, Mishra MJ. Angiomyxoma diagnosed in a man presenting for abdominal lipectomy. Can J Plast Surg 2007; 15: 163-164.
16. Poirier M, Fraser R, Meterissian S. Unusual Abdominal and Pelvic Tumors. Journal of Clinical Oncology 2003; 21: 3535-3541.
17. Rawlinson NJ, West WW, Nelson M, Bridge JA. Aggressive Angiomyxoma with t(12;21) and HMGA2 Rearrangement: Report of a Case and Review of the Literature. Cancer Genet Cytogenet 2008; 181(2): 119-124.
18. Rabban JT, Dal Cin P, Oliva E. HMGA2 Rearrangement in a case of vulvar Aggressive Angiomyxoma. Int J Gynecol Pathol 2006; 25(4): 403-407.
19. McCluggage WG, Connolly L, McBride HA. HMGA2 is a Sensitive but Not Specific Immunohistochemical Marker of Vulvovaginal Aggressive Angiomyxoma. Am J Surg Pathol 2010; 34(7): 1037-1042.
1. Martínez AA, Hernández-González M, Carrera González E. Angiomixoma agresivo en hombres. Rev Med Hosp Gen Mex 2007; 70(2): 78-81. [ Links ]
2. Jingping Z, Chunfu Z. Clinical Experiences on Aggressive Angiomyxoma in China (Report of 93 Cases). Int J Gynecol Cancer 2010; 20: 303-307. [ Links ]
3. Adwan H, Patel B, Kamel D, Glazer G. A solitary encapsulated pelvic aggressive angiomyxoma. Ann R Coll Surg Engl 2004; 86: W1-3. [ Links ]
4. Camps Lasa J, Navarro Luna A, Muñoz Duyos A, García Domingo M, Molina CM. Angiomixoma agresivo pelviperineal en el varón. Cir Esp 2008; 84(2): 101-11. [ Links ]
5. Hastak MS, Raghuvanshi SR, Sahu S, Vyankatesh A, Ramraje SN, Ranjan A. Aggressive Angiomyxoma in men. JAPI 2008; 56: 373-5. [ Links ]
6. Boren T, Lapolla J, Martino M, Nirgudkar P. Aggressive Angiomyxoma: A Case of Multiple Recurrences and Review of the Literature. Journal of Pelvic Medicine & Surgery 2006; 12: 151-6. [ Links ]
7. Mera Velasco S, Cabello Burgos AJ, Ruiz López M, González Poveday I, Santoyo Santoyo J. Resección laparoscópica de angiomixoma pélvico agresivo. CIR ESP. 2010; 88(2): 119-132. [ Links ]
8. Giles DL, Liu PT, Lidner TK, Magtibay PM. Treatment of aggressive angiomyxoma with aromatase inhibitor prior to surgical resection. International Journal of Gynecological Cancer 2007; 8: 369-385. [ Links ]
9. Outwater EK, Marchetto BE, Wagner BJ, Siegelman ES. Aggressive Angiomyxoma: Findings on CT and MR imaging. AJR 1999; 172: 435-438. [ Links ]
10. Xambre L, Cerqueira M, Guimarães I. Angiomixoma agresivo penoescrotal. Actas Urológicas Españolas 2009; 33(3): 321-326. [ Links ]
11. Kondo T. Aggressive angiomyxoma in the inguinal region: a case report. Journal of Medical Case Reports 2010; 4: 396. [ Links ]
12. Wu Ch, Shei-Dei S, Chin D. Scrotal aggressive angiomyxoma mimicking inguinal hernia. Asian J Androl 2007; 9: 1-3. [ Links ]
13. Kidric D, MacLennan G. Aggressive Angiomyxoma of the Male Genital Region. The Journal of Urology 2008; 180: 1506. [ Links ]
14. Morag R, Fridman E, Mor Y. Aggressive Angiomyxoma of the Scrotum Mimicking Huge Hydrocele: Case Report and Literature Review. Case Reports in Medicine. 2009. p. 1-3. [ Links ]
15. Andres LA, Mishra MJ. Angiomyxoma diagnosed in a man presenting for abdominal lipectomy. Can J Plast Surg 2007; 15: 163-164. [ Links ]
16. Poirier M, Fraser R, Meterissian S. Unusual Abdominal and Pelvic Tumors. Journal of Clinical Oncology 2003; 21: 3535-3541. [ Links ]
17. Rawlinson NJ, West WW, Nelson M, Bridge JA. Aggressive Angiomyxoma with t(12;21) and HMGA2 Rearrangement: Report of a Case and Review of the Literature. Cancer Genet Cytogenet 2008; 181(2): 119-124. [ Links ]
18. Rabban JT, Dal Cin P, Oliva E. HMGA2 Rearrangement in a case of vulvar Aggressive Angiomyxoma. Int J Gynecol Pathol 2006; 25(4): 403-407. [ Links ]
19. McCluggage WG, Connolly L, McBride HA. HMGA2 is a Sensitive but Not Specific Immunohistochemical Marker of Vulvovaginal Aggressive Angiomyxoma. Am J Surg Pathol 2010; 34(7): 1037-1042. [ Links ]

