










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev Col Gastroenterol vol.26 no.4 Bogotá Oct./Dec. 2011
Gastric gastrointestinal stromal tumor with unusual skull metastasis
Alfredo Ernesto Romero Rojas, MD (1), Oscar Alberto Mesa Botero, MD (1), Mario Alexander Melo Uribe, MD (2), Sandra Isabel Chinchilla Olaya, MD (1), Paula Alejandra Barajas Solano, MD (2)
(1) Grupo de Patología del Instituto Nacional de Cancerología (INC) in Bogotá, Colombia.
(2) Grupo Patología Estructural Funcional y Clínica de la Universidad Industrial de Santander (PATUIS) in Bucaramanga, Colombia.
Translation from Spanish to English by T.A. Zuur and The Language Workshop
Received: 16-05-11 Accepted: 11-10-11
Abstract
Gastrointestinal stromal tumors (GISTs) originate in the wall of the digestive tract from the esophagus to the anus. Approximately 25% of gastric GISTs are clinically malignant. Most often they metastasize to the liver, less commonly to soft tissues and bone. The clinical case of a patient with a gastric GIST, liver and unusual cranial metastasis is presented.
Key words
Gastrointestinal stromal tumors, cranial neoplasms, immunohistochemistry.
INTRODUCTION
Gastrointestinal stromal tumors (GIST) originate in the wall of the digestive tract from the esophagus to the anus. They are derived from the interstitial cells of Cajal, the gastrointestinal pacemaker cells of Auerbachs plexus (1).
GISTs were first described by Martin and Stout (2) who published several cases of stomach tumors formed by rounded epitheloid cells. Stout coined the term "leiomyoblastoma" for these lesions in the belief that they were primitive tumors of the smooth muscle. In 1983 Mazur and Clark documented the absence of muscular markers in the majority of these lesions and the unexpected immunohistochemistry finding of neural markers. They later proposed the term "stromal tumor" which they subsequently modified to gastrointestinal stromal tumor (3). In 1998, Hirota et al. observed that the presence of c-KIT proto-oncogene, a class III receptor tyrosine kinase, was necessary for the normal development of the interstitial cells of Cajal. The loss of this gene resulted in absence of interstitial cells of Cajal and/or mutations in them. This could be related to the formation of this type of neoplasia (4).
GISTs constitute the most common mesenchymal tumor of the gastrointestinal tract. These mainly affect adults with an average age of 55 to 60 years, and less frequently affect children from ten to twenty years of age (<1%). 60% are located in the stomach, 35% in the small intestine and less than 5% in the rectum, esophagus, mesenterium and omentum (1). Approximately 25% of gastric GISTs and 50% of small intestine GISTs are clinically malignant. They metastasize primarily within the abdominal cavity and liver, less commonly in soft tissues, lymphatic skin, ganglia, lung and bone. Metastatic compromise of the skull is very infrequent: our search documented only one case (5).
We describe the clinical case of a patient with histopathologic and immunohistochemical diagnosis of gastric GIST and a very unusual metastatic compromise of the skull.
MATERIALS AND METHODS
Clinical case
The patient was a 38 year old male endoscopically diagnosed with a 6 centimeter neoplastic mass located in the gastric corpus. A biopsy of the lesion showed a high risk GIST. Later, a CAT scan showed a hepatic nodule and an enlarged perigastric lymph node. Palliative partial gastrectomy was performed followed by a definitive histopathological study which also showed a high risk GIST which had metastasized to a lymph node and to the liver. The immunohistochemical analysis showed the presence of CD117 (c-KIT), was positive for CD34 and showed smooth muscle actin with 15% Ki67; it was negative for S-100 and desmin. The section margins were negative (Figure 1).
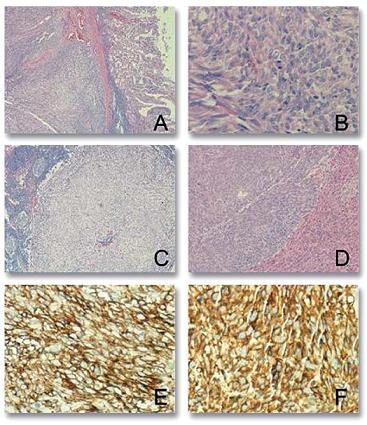
Figure 1. A) High Risk Gastric GIST. B) Hypercellular Tumor constituted by fusiform cells (H&E10X) with high mitotic activity (H&E40X). C) Metastasis in lymph node (H&E10X). D) Hepatic metastasis (H&E10X). E) Intense positivity for CD117 (c-KIT) (20X). F) Positive for CD34 (20X).
After surgery the patient received no additional treatment. Twenty-eight months later the patient presented progressive growth of a mass in the left frontoparietal region of the skull. A CAT scan of the skull showed a neoplastic mass at calotte level that compromised the frontal and left parietal bone together with signs of edema of the ipsilateral cerebral parenchyma covering an area of 10cm x6cm x 8 cm. An MRI demonstrated hyperintense and hypointense areas suggesting bleeding and calcifications. Bone scintigraphy showed an increased fluorodeoxyglucose (FDG) uptake lesion in the left parietal-temporal region with no other metastatic bone lesions. An abdominal CAT scan showed an enlarged liver with the presence of multiple metastases that almost replaced the totality of the parenchyma without evidence of any residual tumor in the area affected by earlier surgery (Figure 2).
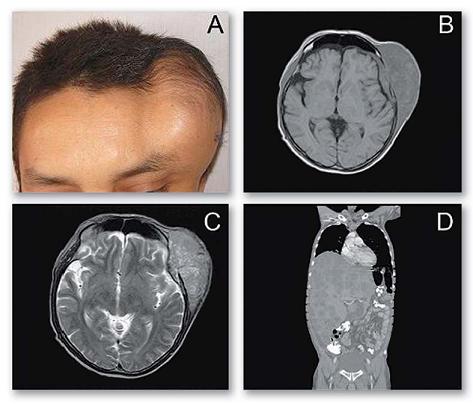
Figure 2. A) Image of mass in left frontoparietal region B and C) MRIs of T1 and T2 show a heterogeneous lesion with hyperintense and hypointense areas suggesting bleeding and calcifications. D) The abdominal CAT scan identified an enlarged liver with multiple metastases that almost replace the totality of the parenchyma without evidence of residual tumor in previous surgical area.
Pathological examination of a biopsy taken from the skull lesion demonstrated compromise by a tumor with histological characteristics similar to those of the gastric lesion. For this reason it was diagnosed as a GIST metastasis. A new immunohistochemical study tested positive for CD117, CD34 and AML, and 40% Ki67 but negative for cytokeratins, CD99, S-100 and D240 (Figure 3).
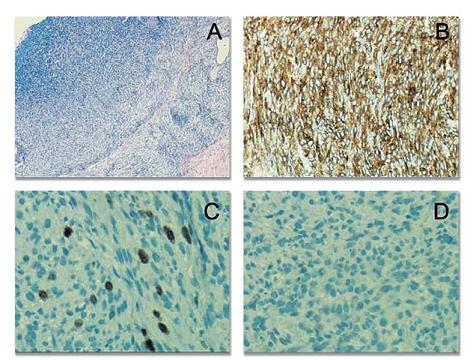
Figure 3. GIST skull metastasis. A) Image of the tumor composed of hypercellular fusiform cells (H&E10X) B) Intense positivity for CD117 (c-KIT) (20X). C) Elevated expression of Ki67 (40X). D) Negative for cytokeratin (20X).
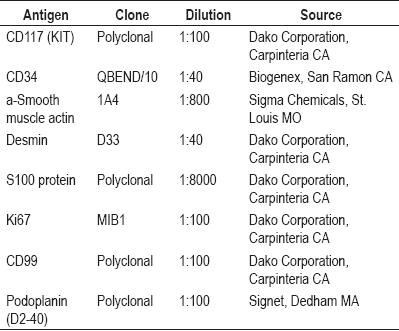
The most important technical characteristics of the immunohistochemistry markers are summarized in Table 1.
Table 1. Primary antibodies used in this study with their dilutions and commercial sources.
DISCUSSION
GISTs are a heterogeneous group of neoplasias for which prediction of biological behavior requires an evaluation of multiple microscopic and macroscopic parameters. The most commonly used classification is based on two predictive characteristics: size and mitotic index (6). High risk GISTs are defined as those that measure more than 5 centimeters, have a mitotic index > 5/50 HPF, an MiB1 index > 10%, and show invasion of lymph nodes or metastasis (7). All of these criteria were present in our case.
The main molecular characteristics of these tumors found in up to 85% of the cases are mutations that activate a tyrosine kinase that produces protein overexpression that can be detected by immunohistochemistry through CD117 (8, 9). Up to 70% of GISTs are positive for CD34 and H-Caldesmon, 30% are positive for smooth muscle actin (AML), less than 10% are positive for desmin, and less than 5% are positive for S100 protein (8, 9). Currently DOG1.1 appears to be the most specific immunohistochemical marker for GIST diagnosis (10).
Imatinib, a tyrosine kinase Kit/PDGFRA inhibitor can be used satisfactorily for treatment of metastatic GIST (1). Hematogenous metastasis commonly develops in the liver and is very rare in the bones where their incidence is approximately 5.5% (5). They have been described in vertebrae and other bones without specified locations. In our review of the literature we found one description of metastasis to the skull which was similar to the case described here.
The differential diagnosis of skull lesions using contrast media to enhance computerized tomography must evaluate and rule out meningiomas (5), primary meningeal sarcomas, cutaneous or metastatic sarcomatoid carcinomas and histiocytic sarcomas. All of these require pathological evaluation in every case.
No oncogene mutation (kit or PDGFRA) correlates with high metastatic potential, although mutations in KIT exon 9 are related to a worse prognosis and to poor response to imatinib. The anatomical location, the mutational state and other characteristics of the GIST must be taken into account in the prognosis (5).
In conclusion, we have described the clinical case of a patient with a GIST that had metastasized to the liver, lymph nodes and skull. Because the metastasis to the skull is rare it became necessary to extend the study of this pathology and to consider a differential diagnosis of cranial metastasis.
REFERENCES
1. Miettinen M, Lasota J. Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med 2006; 130(10): 1466-78.
2. Weiss S. Tumores del estroma extragastrointestinal. En Weiss S, Goldblum J. Tumores de partes blandas. 5 ed. Elsevier Mosby 2009. p. 565.
3. Mazur MT, Clark HB. Gastric stromal tumors: reappraisal of histogenesis. Am J Surg Pathol 1983; 7: 507.
4. Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S, Kawano K, Hanada M, Kurata A, Takeda M, Muhammad Tunio G, Matsuzawa Y, Kanakura Y, Shinomura Y, Kitamura Y. Gain-of-funtion mutations of c-KIT in human gastrointestinal stromal tumors. Science 1998; 279: 577.
5. Gil-Arnaiz I, Martínez-Trufero J, Pazo-Cid Roberto A, Felipo F, Lecumberri MJ, Calderero V. Skull metastasis from rectal gastrointestinal stromal tumours. Clin Transl Oncol 2009; 11: 625-627.
6. Fletcher CDM, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, Miettinen M, OLeary TJ, Remotti H, Rubin BP, Shmookler B, Sobin LH, Weiss SW. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol 2002; 33: 459-465.
7. Bucher P, Egger JF, Gervaz P, Ris F, Weintraub D, Villiger P, Buhler LH, Morel P. An audit of surgical management of gastrointestinal stromal tumours (GIST). Eur J Surg Oncol 2006, 32: 310-4.
8. Goldblum JR. Gastrointestinal stromal tumors. A review of characteristics morphologic, immunohistochemical, and molecular genetic features. Am J Clin Pathol 2002; 117 Suppl: S49-61.
9. Turner MS, Goldsmith JD. Best practices in diagnostic immunohistochemistry: spindle cell neoplasms of the gastrointestinal tract. Arch Pathol Lab Med 2009; 133(9): 1370-4.
10. Liegl B, Hornick JL, Corless CL, Fletcher CD. Monoclonal antibody DOG1.1 shows higher sensitivity than KIT in the diagnosis of gastrointestinal stromal tumors, including unusual subtypes. Am J Surg Pathol 2009; 33(3): 437-46.
1. Miettinen M, Lasota J. Gastrointestinal stromal tumors: review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch Pathol Lab Med 2006; 130(10): 1466-78. [ Links ]
2. Weiss S. Tumores del estroma extragastrointestinal. En Weiss S, Goldblum J. Tumores de partes blandas. 5 ed. Elsevier Mosby 2009. p. 565. [ Links ]
3. Mazur MT, Clark HB. Gastric stromal tumors: reappraisal of histogenesis. Am J Surg Pathol 1983; 7: 507. [ Links ]
4. Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S, Kawano K, Hanada M, Kurata A, Takeda M, Muhammad Tunio G, Matsuzawa Y, Kanakura Y, Shinomura Y, Kitamura Y. Gain-of-funtion mutations of c-KIT in human gastrointestinal stromal tumors. Science 1998; 279: 577. [ Links ]
5. Gil-Arnaiz I, Martínez-Trufero J, Pazo-Cid Roberto A, Felipo F, Lecumberri MJ, Calderero V. Skull metastasis from rectal gastrointestinal stromal tumours. Clin Transl Oncol 2009; 11: 625-627. [ Links ]
6. Fletcher CDM, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, Miettinen M, OLeary TJ, Remotti H, Rubin BP, Shmookler B, Sobin LH, Weiss SW. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol 2002; 33: 459-465. [ Links ]
7. Bucher P, Egger JF, Gervaz P, Ris F, Weintraub D, Villiger P, Buhler LH, Morel P. An audit of surgical management of gastrointestinal stromal tumours (GIST). Eur J Surg Oncol 2006, 32: 310-4. [ Links ]
8. Goldblum JR. Gastrointestinal stromal tumors. A review of characteristics morphologic, immunohistochemical, and molecular genetic features. Am J Clin Pathol 2002; 117 Suppl: S49-61. [ Links ]
9. Turner MS, Goldsmith JD. Best practices in diagnostic immunohistochemistry: spindle cell neoplasms of the gastrointestinal tract. Arch Pathol Lab Med 2009; 133(9): 1370-4. [ Links ]
10. Liegl B, Hornick JL, Corless CL, Fletcher CD. Monoclonal antibody DOG1.1 shows higher sensitivity than KIT in the diagnosis of gastrointestinal stromal tumors, including unusual subtypes. Am J Surg Pathol 2009; 33(3): 437-46. [ Links ]

