










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957
Rev Col Gastroenterol vol.27 no.4 Bogotá oct./dic. 2012
Original articles
(1) Gastroenterology and Endoscopy Group at the Instituto Nacional de Cancerología de Colombia
(2) Medical Department at Sanofi-aventis Colombia S.A.
Conflict of interest: REGATE was sponsored by SANOFI.
Received: 18-05-12 Accepted: 23-10-12
Abstract
Purpose: The purpose of this study was to collect and analyze data related to the diagnosis, treatment, and outcomes of patients with newly diagnosed gastric cancer (GC) no matter at what stage of the disease diagnosis occurred. Methods: REGATE is an international, multicenter, observational survey of patients with GC. Patients with newly diagnosed primary GC were enrolled from August 2004 to July 2008. Data were collected at an initial visit and again within 10 months of the first consultation. We collected baseline characteristics, staging, diagnosis, and treatment information. Results for Colombia are presented in this article. Results: 600 subjects were enrolled. The mean age among participants was 62.80±12.89 years. 65.2% of the participating subjects were males. 98% had experienced gastric symptoms, and 97.6% had had a previous endoscopy. Mean time from first symptoms to diagnosis was 6.45±6.84 months. Only 6% (36) had family histories of gastric cancer while 68.3% (409) of the subjects had not been assessed for H. pylori infections. Of those assessed only 7.7%, (46) were positive for H. pylori infection. The most frequent primary tumor site was in the antrum (40.9%). 34.4% had poorly differentiated tumors while 34.7% had stage II disease. Surgery was the most frequent treatment (62.0%) followed by palliative therapy (46.3%). The most common neoadjuvant therapies were fluoropyrimidines and platinum salts. Conclusions: More than 95% of the 600 patients were enrolled in REGATE Colombia had complained of gastric symptoms and had had at least one endoscopy. Mean time to diagnosis was 6.45months. The great majority of these subjects had poorly differentiated tumors and had been diagnosed at stage II. The most common treatment was surgery, followed by palliative therapy.
Key words
Registry, gastric cancer, epidemiology.
Gastric cancer (GC) is the second leading cause of death worldwide. There are multiple risk factors with low magnitudes of association. These include genetic factors, Helicobacter pylori infections, and consumption of large quantities of salty foods, smoked foods, or foods with nitrites. Worldwide, the highest incidence rates are in Japan, Eastern Europe, South America, and some parts of the Middle East (1). According to 2008 GLOBOCAN statistics, in Colombia the age-adjusted incidence of GC is estimated to be 17.4/100,000 while the age-adjusted mortality age rate is estimated to be 13.3/100,000 inhabitants: GC is the second leading cause of cancer mortality in Colombia (2,3).
It has been reported that the incidence of GC has been dropping in most countries because of changing nutritional habits, including changes in food preparation, and because of changes in specific environmental factors (4, 5). Additionally, in countries with high incidences of GC such as Japan, the introduction of mass screening programs has reduced mortality rates associated with this disease (4). Screening and early diagnosis have helped achieve 5 year survival rates of over 50% for patients with stage I GC (1,4). However, in most countries, the disease is diagnosed in later stages and has higher mortality rates (4, 5). There are significant regional diferences in the therapeutic approach to GC. Surgical resection is the primary treatment for gastric cancer, but additional resection of lymph nodes remains a point of controversy. In some western countries extended lymph node dissection (D2 resection) is not usual and eventually lymph node preservation results. In Japan, endoscopic mucosal resection is performed for early gastric carcinoma lesions that meet specific routine requirements (6). There are also diferences regarding the use of new agents or combinations of adjuvant therapies as well as regarding the roles of other forms of treatment such as chemoradiotherapy, chemoimmunotherapy, intraperitoneal adjuvant therapy, and neoadjuvant chemotherapy (7).We consider that it is essential to understand the Colombian situation and thus determine the possible gaps in diagnosis and management of these patients that may exist in comparison with other countries. REGATE is a disease registry designed for capturing and analyzing data from newly diagnosed GC patients at any stage of the disease. It seeks to discover the patterns in diagnoses, treatments and outcomes. We present the results for Colombia below (9).
MATERIALS AND METHODS
From August 2004 to July 2008 adult patients from Colombia were included in REGATE (Registry of Gastric Cancer Treatment Evaluation), an international multicenter, observational registry for patients who have been newly diagnosed with gastric cancer (9). Sample size was calculated independently for each country so that it would be representative of the country and allow for 95% confdence intervals. To ensure the scientifc integrity of this work, the design and conduct of the study was done with the guidance of an International Scientifc Advisory Commitee composed of 6 academic experts in the area of gastric cancer from around the world. The registry was implemented by the SANOFI research center.
Participating centers were selected on the basis of a list of medical oncologists and oncology specialists in public or private practice at medical centers in Colombia. To avoid selection bias from this list participating centers were randomly chosen and eligible patients in each center were consecutively ordered during the study period. All required protocol information for each patient was included on a standardized data collection form by the physician or a designee who had been trained in study procedures. During enrollment all information regarding patient demographics, staging at the time of diagnosis of gastric cancer, and the patient's treatment plan were registered on the form. During the follow-up visit (final visit) about 8-10 months after the enrollment visit, treatment received by the patient was recorded.
Demographic information, tumor staging, diagnostic assessment, and treatment at each visit were analyzed for the entire population using descriptive analysis and central tendency measures.
Researchers in Colombia who participated in the REGATE study included Dr. Ricardo Oliveros (Instituto Nacional de Cancerologia Bogotá), Dr. Eduardo Minuche and Dr.Carlos Narvaez (Hospital Departamental, Pasto, Nariño), Germán Echeverria (Instituto de Cancerologia Tunja, Boyacá), Dra. Lucy Rocillo (ISS Rafael Uribe Uribe, Cali) and Dr. Ernesto Benavides (Liga de Lucha Contra el cancer seccional Huila, Neiva).
RESULTS
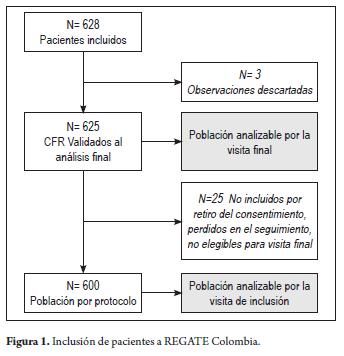
From August 2004 to July 2008 628 patients newly diagnosed with gastric cancer were identified in 6 medical centers in Colombia. Of these patients 625 were included in the analysis of the initial visit. By the end of monitoring 600 patients had completed the study (Figured 1 and 2). Descriptive demographic characteristics are shown in Table 1.
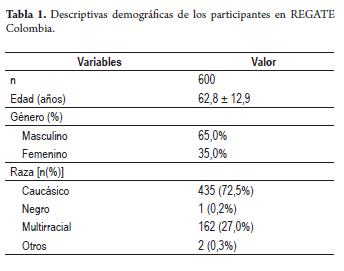
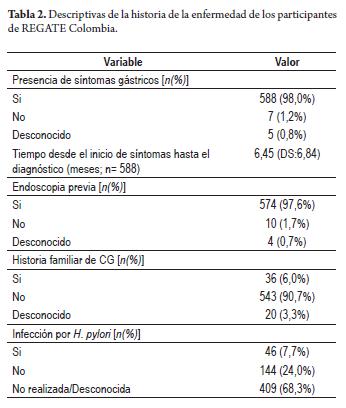
The average age of the participants was 62. 8 ± 12.9 years. Nearly two out of three patients in the registry were male (n = 408, 65.0%). Most patients (98.0%) reported having symptoms associated with GC at the time of diagnosis. The average time from first symptoms to the time of diagnosis was approximately 6.45 months (SD 6.84, n = 574), and most patients had had previous endoscopic evaluations (97.6%, n = 574). 6.0% (n = 36) of patients included in the registry had family histories of gastric cancer. 7.7% (n = 46) of patients had documented H. Pylori infections although 68.3% (n = 409) of patients were not evaluated for H. Pylori infections or the results were unknown (Table 2).
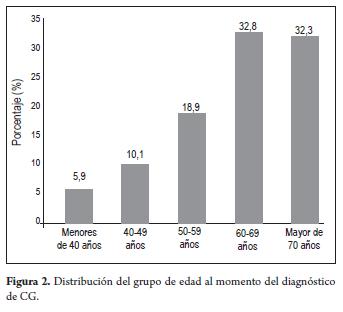
Primary tumors were found in the following locations in order of frequency: antrum (40.9%, n = 245) corpus (30.1%, n = 180), and proximal (22.2%, n = 133). Only 6.8% (n = 41) were classified as engaging the whole stomach (Figure 2). The diagnostic method most frequently used was the endoscopy (98.0%, n = 589). Histopathological staging of tumors was reported for 95.7% of patients (n = 572). Most of the histopathological reports used the Lauren criteria (52.3%, n = 299). This was followed by the combination of the Lauren criteria with the World Health Organization (WHO) criteria in 27.8% of cases. The Ming criteria and the WHO Classification alone were only used in a few cases. Histological subtypes in order of frequency were intestinal (75.9%), difuse (19.7%), and mixed (4.3%). Histologic grade was documented in 474 patients. Most had poorly differentiated tumors (34.4%, n = 163) or moderately differentiated tumors (31.4%, n = 149). Well-differentiated tumors and undifferentiated tumors were less frequent, 19.2% (n = 91) and 11.4% (n = 54) respectively.
Only 476 subjects (79.7%) had preoperative clinical staging available (Figure 3). According to staging by the AJCC/UICC (American Joint Commitee on Cancer and International Union Against Cancer) staging systems, the only ones used in Colombia, 62 patients (13%) were classified as stage I, 165 (34.7%) at stage II, 120 (25.2%) at stage III, and 128 (26.9%) at stage IV (Figure 3). Working diagnoses and tumor staging for these patients in Colombia were broad and used primarily physical examinations (96%, n = 464) and diagnostic imaging. Imaging techniques included simple radiography (n=417 patients or 86.3%), ultrasound (15.3%), abdominal CT scans (n = 464patients or 96.0%) laparoscopy (n = 27 patients or 5.4%) and endoscopic ultrasound (n = 6 patients or 1.2%).
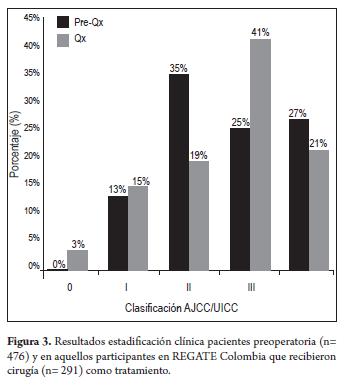
A comparison of preoperative staging results and diagnosis from results of final pathology following surgery showed that whereas 35% of patients diagnosed as stage 2 prior to surgery 19% were in fact at stage 2, but the number of III diagnoses increased from 25% to 41%. Final results showed lower percentages of stage I and II lesions and higher percentages of stage III and IV lesions.
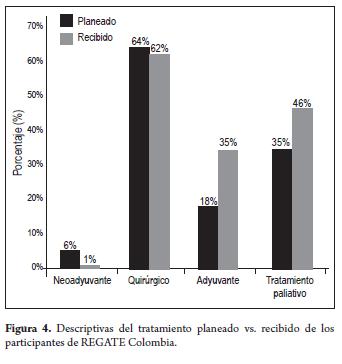
Initial decisions to treat were made primarily on the basis of patient staging. Decisions were made by multidisciplinary teams in 61.5% of the cases. The surgeon alone decided on treatment in 26.9% of the cases (n = 161) while the clinical oncologist decided alone in 10.5% (n = 63) of the cases. During the initial visit decisions on initial treatment plans for patients were recorded. Results showed surgery as primary treatment in 64% of cases (n = 384), adjuvant chemotherapy in 18.2% (n = 109), neoadjuvant in 5.5% (n = 33) and palliation in 34.8% (n = 209). These alternatives were not mutually exclusive but could be combined. The most frequent combination planned was surgery + adjuvant (17.7%). Among considerations that were taken into account for treatment selection, the most relevant were, in order of importance: tumor staging, general condition of the patient (including comorbidities and age), and to lesser extents the histological type and tumor location.
The final monitoring visit for the 600 patients took place on average 8.65 (SD 3.55) months after the initial visit. This final visit documented the treatment to which the patient was finally subjected. Treatment changed from the initial plan for some patients, including 19.3% of the patients who received no treatment for their tumors (Figure 4). Primary treatments received by patients in order of frequency were surgery (62%, n = 300), adjuvant chemotherapy (34.5%, n = 167), neoadjuvant (1.4%, n = 7) and palliation (46. 3% n = 224). These alternatives were not mutually exclusive, meaning that they could be combined. The most common operations were distal subtotal gastrectomy (50%, n = 127) and total gastrectomy (47.2%, n = 120). Clinical staging of patients who underwent surgery (n = 291) was as follows: 3.4% stage O, 14.8% stage I, 19.2% stage II, 41.2% stage III, and 21.3 %, stage IV.
Lymph node resections were performed in 85.3% (n = 250) of patients who had surgery. The most frequently planned combination of treatments was surgery + adjuvant (26.3%). Of the 386 patients who received any treatment in addition to surgery, 76.3% received some form of chemotherapy, 54.0% received some form of radiation therapy, and 47.9% received the combination of these two treatments. Chemotherapy agents most frequently used were fluoropyrimidines (100%: 5-fluorouracil [5FU] and capecitabine) and platinum salts (85.7%: carboplatin and cisplatin). The most frequently used palliative treatments were monotherapy with 5FU (97.6%) and polychemotherapy.
When analyzing the results according to the year of inclusion in the record, a tendency for the average time between onset of symptoms and diagnoses of GC to decrease was found. It was 7.19 ± 10.36 months in 2004, but had decreased to 6.83 ± 4.84 months in 2008. There was also a tendency to treat a greater percentage of patients surgically: 24 (46.2%) in 2004, 105 (66.9%) in 2005, 92 (68.1%) in 2006, 145 (62.2%) in 2007 and 18 (78.3%) in 2008.
DISCUSSION
The REGATE study is the largest multicenter prospective register established for gastric cancer patients in the world (9). Colombia is one of the fve countries with the highest incidences of this tumor. The others are Japan, Costa Rica, Singapore, and Chile (2, 3, 10). The 600 patients who form the Colombian share of the registry account for 5.8% of the global sample.
This analysis reports the Colombian data and allows for an assessment of demographic and clinical characteristics of patients at diagnosis, as well as an assessment of considerations related to choices of treatment plans between 2004 and 2008. Except for the higher proportion of multiple racial origins, the demographic characteristics of the Colombian GC population were very similar to those reported in the rest of the world (9). The median age of 62 years for this Colombian population of newly diagnosed GC patients is similar to the median age of 60 years reported in the overall analysis of REGATE.
Among the similarities with the overall data, a greater presence of gastric symptoms was also found in Colombia than in the rest of the world. 90% of the Colombian study population reported gastric symptoms (9). The duration of symptoms before diagnosis is consistent with the findings in the Valdivia record (8), in which 40% of the patients had had symptoms for more than 6 months prior to diagnosis. This may refect the lack of knowledge of the Colombian population about the need for consulting a doctor in case of digestive symptoms, and it may also refect poor accessibility to specialized medical care (3). As in the rest of the world, the main method of diagnosis in Colombia was upper endoscopy which was used for 98.5% of patients. However, this report calls our atention to the lack of assessment for Helicobacter pylori, unknown or not reported for 68.3% of this population.
Figures on tumor location reveal that in Colombia the most common tumor location remains the antrum. This is unlike the rest of Latin America and the world, where this location has been decreasing (24% and 39%, respectively). Histopathologic typing of 88.1% of patients was consistent with endoscopic diagnosis and confirmed most diagnoses. The most widely used histological Classification was the Lauren Classification, but there were also pathology reports based on Lauren/WHO Classification which made analysis of this population difficult. In Colombia a lower percentage of patients were diagnosed with stage IV (26.9%) than in the overall data which reported 37.7% of patients at stage IV. The most frequently used clinical method for staging in Colombia was the CT scan (96%) which is a much higher percentage than for global REGATE which reported the use CT scans in 75.7% of patients. This number may refect a certain bias in the selection of patients being enrolled from tertiary care hospitals. The factor most ofen considered for therapeutic decisions were overall patient condition including comorbidities and age. In the world series in which in addition to the clinical stage, tumor location was the most important factor. It is valuable to note that in most cases (61.5%) the treatment plan was decided by on by a multidisciplinary team, a figure higher than that reported in the rest of the world and for Latin America as a whole (53.5%).
In conclusion, in Colombia gastric cancer is still diagnosed relatively long after symptoms developed and at advanced stages. Diagnosis is done by endoscopy with histological confirmation in most cases. This study allowed confirmation that surgery is part of the treatment plan in the majority of cases while adjuvant or neoadjuvant therapies are ofered to only 1 out of 4 patients diagnosed. However, more than half of the patients were evaluated by a multidisciplinary committee to establish the therapeutic plan.
Conflicts of interest
The researchers would like to state that they have received honorariums for research from SANOFI.
REFERENCES
1. Parkin DM, Bray F, Pisani F, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74-108. [ Links ]
2. GLOBOCAN 2008. Disponible en el siguiente URL: http://globocan.iarc.fr/factsheets/populations/factsheet.asp?uno=170, descargado en noviembre 02 de 2011. [ Links ]
3. Correa P, Piazuelo MB. Gastric cancer: The Colombian enigma. Revista Colombiana de Gastroenterología 2010; 25(4): 334-337. [ Links ]
4. Catalano V, Labianca R, Bereta GD, Gata G, de Braud F, Van Cutsem E. Gastric cancer. Crit Rev Oncol 2009; 71(2): 127-164. [ Links ]
5. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA: a cancer journal for clinicians 2011. [ Links ]
6. Liakakos T, Roukos DH. More controversy than ever- Challenges and promises towards personalized treatment of gastric cancer. Annals of surgical oncology 2008; 15(4): 956-960. [ Links ]
7. Fatouros M, Ziogas D. Controversy in the treatment of gastric cancer. Annals of surgical oncology 2008; 15(6): 1795-1797. [ Links ]
8. Heise K, Bertran E, Andia ME, Ferreccio C. Incidence and survival of stomach cancer in a high-risk population of Chile. World journal of gastroenterology: WJG 2009; 15(15): 1854. [ Links ]
9. Ter-Ovasenov M, Bang Y, Yalcin S, Roth A, Zalcberg J, Soloviev V. Registry of gastric cancer treatment evaluation (REGATE): Baseline characteristics of 10.299 patients from 22 countries. J Clin Oncol 2009; 27(15 Suppl. 1): 220S. [ Links ]
10. Bertuccio P, Chatenoud L, Levi F, et al. Recent patterns in gastric cancer: A global overview. International Journal of Cancer 2009; 125(3): 666-673. [ Links ]
