










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.28 no.3 Bogotá July/Sept. 2013
Images of early gastric cancer: a series of cases
Martín Alonso Gómez, MD. (1)
(1) Assistant Professor of Gastroenterology in the Internal Medicine Department at the Universidad Nacional de Colombia in Bogotá, Colombia.
Received: 02-09-12 Accepted: 26-06-13
Abstract
This article presents a study of a series of 5 cases of early gastric cancer, which seeks to raise awareness among young gastroenterologists about the importance of early detection of cancer. It presentsimages of how these tumors were found and evaluated in our hospital. These 5 cases show each of the types of cancer according to the Paris classification through endoscopic images is shown, pathology, and how each case was treated. Some EUS images are also included.
Key words
Gastric cancer, endoscopic mucosal resection, endoscopic ultrasound.
In 1903 German physician M. Versé first described early gastric cancer in his book Die Histogenese der Schleimhautcarcinome (1), but the first to use the term early gastric cancer was the Frenchman Bayle in 1833 who called it "Gastric cancer in its early stages" (2).
This term is used for patients with gastric cancer whose tumors invade into the submucosa whether or not lymph nodes are compromised (3). The 5-year survival rate among these patients can reach almost 100% as our group recently demonstrated (4). However, advanced gastric cancer (muscularis propria) has dramatically reduced 5 year survival rates of less than 10% (5).
Gastric cancer is the second leading cause of cancer in men and the fourth leading cause in women in Colombia. It is the leading cause of cancer mortality according to the INC (2005) (6). 80% of these lesions are diagnosed in late stages with the dismal prognosis already noted. This makes prevention and detection of these tumors at an early stage a prime target in order to change this reality.
For endoscopic classification of tumors we use the Japanese classification system established in 1962, modified by the Paris classification of 2003 (Figure 1) (7). For advanced cancer we use the Bormann classification (Figure 2).


In this paper we present the images of some of our patients with early cancer to illustrate each of the types described by the Paris classification. We not only show these tumors which are characterized as rare in our environment but also show their treatment.
CASE 1
Early gastric cancer 0-Ip
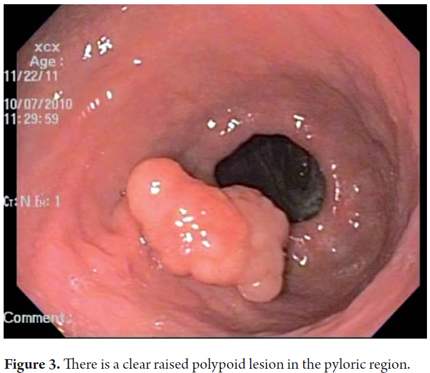
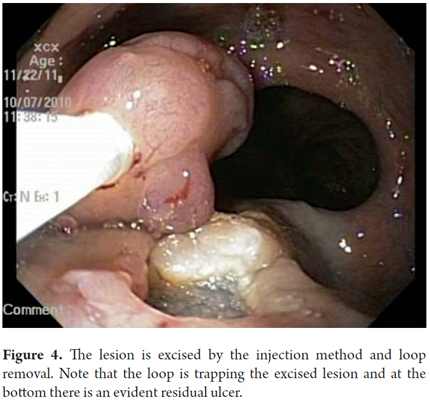
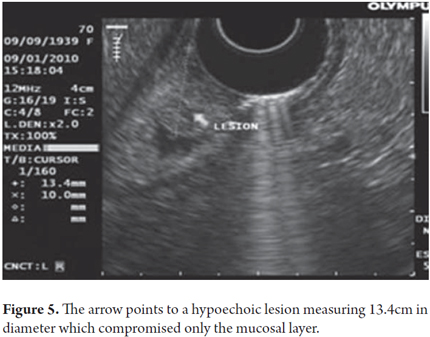
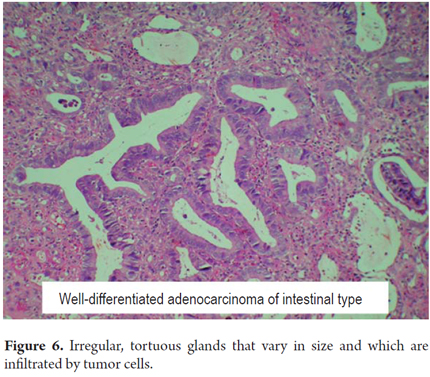
Upper endoscopy was performed on a 75 year old patient who had developed dyspeptic symptoms without any prior warning signs. A raised20 mm lesion found in the prepyloric region was classified as a type 0-I lesion (Figure 3). Endoscopic mucosal resection performed with the lift and cut with loop method achieved complete removal without complications (Figure 4). A previous endoscopy had shown compromise by a tumor in only the first two ultrasound layers i.e. the mucosa (Figure 5). The pathology report indicated a well-differentiated adenocarcinoma with lateral edges and depths that were negative for a tumor (Figure 6).
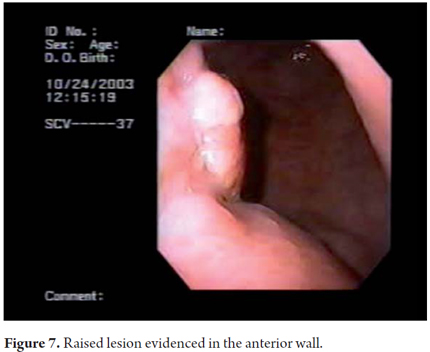
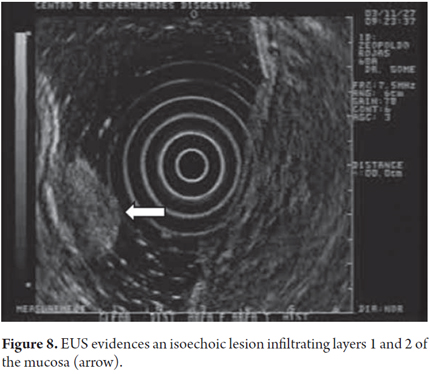
In this other case a raised lesion in the anterior wall of the mid-corpus (Figure 7) can be seen. It was reported as a well-differentiated adenocarcinoma. An endoscopy showed that the lesions compromised only the first two ultrasound layers (mucosa) (Figure 8).
CASE 2
Early gastric cancer 0-II a + II c
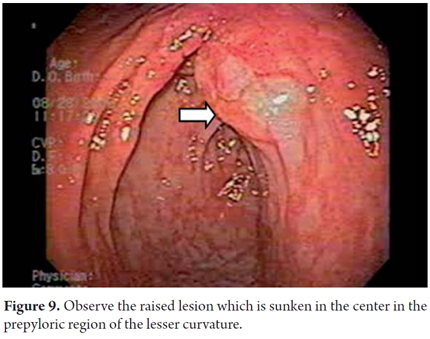
Endoscopy of a 45-year-old patient with dyspeptic symptoms without warning signs such as bleeding, weight loss or vomiting showed a raised lesion in the pre-pyloric antral region that appeared to be ulcerated in the center (Figure 9).
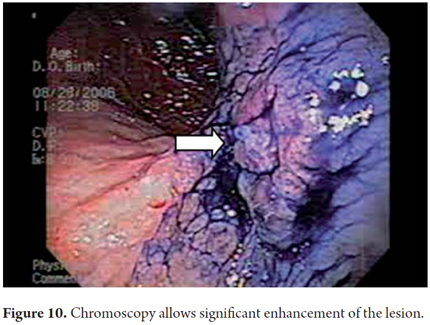
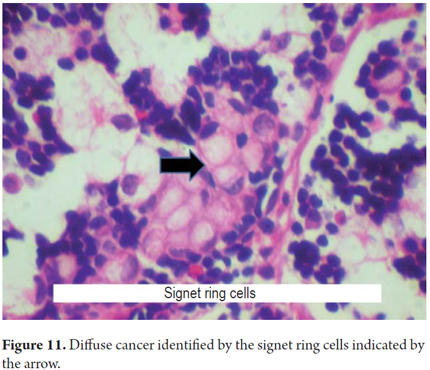
Chromoscopy with a mixture of 0.4% carmine indigo plus 15 ml of acetic acid (vinegar) to better characterize the lesion showed a raised lesion with a sunken center which corresponds to a cancer type 0 - IIa + IIc (Figure 10). The biopsy confirmed diffuse cancer, so the patient was referred to surgery (Figure 11).
CASE 3
Early gastric cancer 0-II b
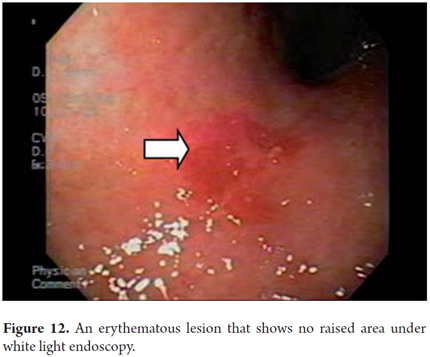
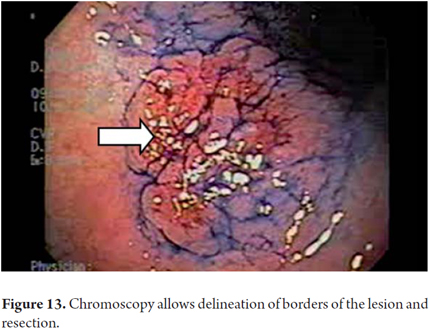
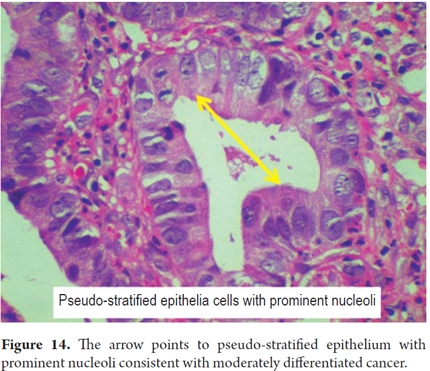
The first endoscopy of a 74-year-old patient who had suffered 6 years of evolving epigastric pain without bleeding or weight loss showed an erythematous lesion on the lesser curvature toward the gap (Figure 12). Chromoscopy using 0.4% indigo carmine achieved fine highlighting of the lesions' boundaries as shown in Figure 13. The lesion was classified as IIb lesion after biopsies showed that it was a moderately differentiated cancer (Figure 14). Mucosal resection was performed.
CASE 4
Early gastric cancer 0- IIc
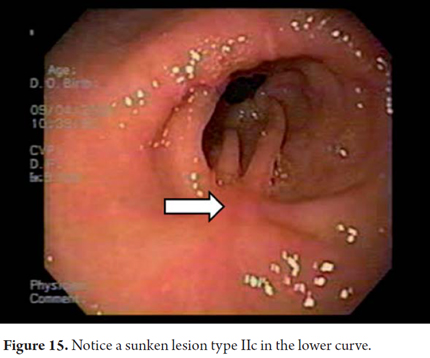
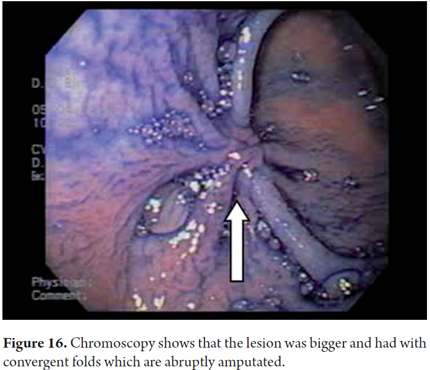
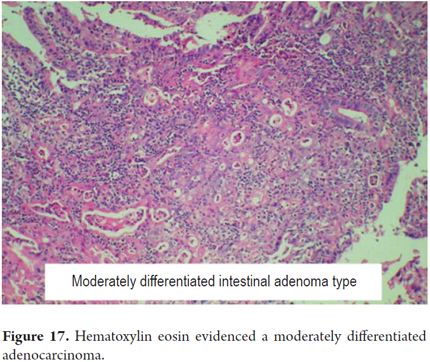
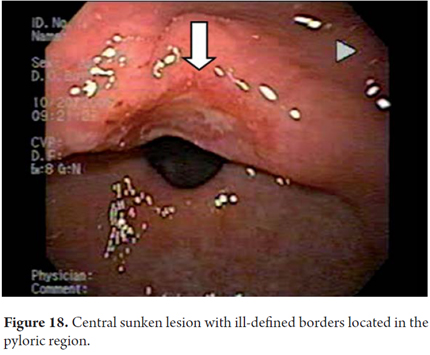
Endoscopic examination of a 66 year old patient with megaloblastic anemia revealed a lesion in the greater curvature of the antrum. The lesion had convergent folds and was sunken in the center but had no atrophy (Figure 15). Chromoscopy with indigo carmine provided excellent definition of the lesion which allowed characterization as IIc (Figure 16). A biopsy confirmed that it was a moderately differentiated adenocarcinoma (Figure 17). In this other case there is a patient with a prepyloric sunken lesion reported as a poorly differentiated adenocarcinoma (Figure 18).
CASE 5
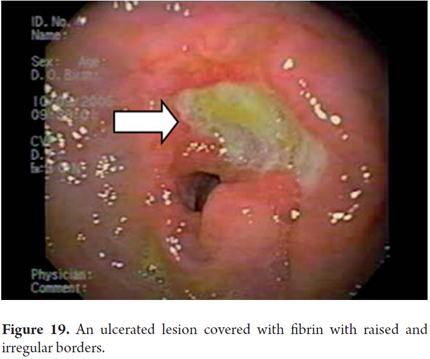
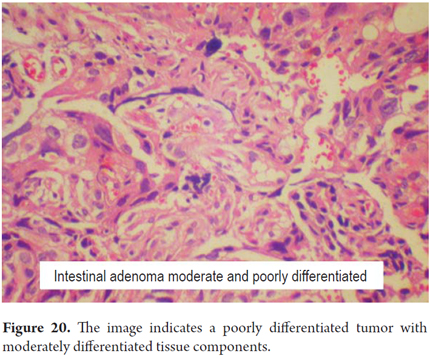
Early Gastric Cancer TYPE: 0 III
Upper endoscopy of a 60-year-old patient admitted to the emergency room with hematemesis and melena, but without weight loss, showed a pre-pyloric ulcerated lesion with irregular borders which was covered with fibrin (Figure 19). The lesion was diagnosed as a moderately differentiated adenocarcinoma (Figure 20), and the patient was referred to surgery which confirmed that the lesion extended into the submucosa.
In conclusion, we can see that the early gastric cancer can be diagnosed and treated through upper endoscopy. Although most of the lesions described were small and were resolved through mucosal resection, we consider that, despite the proliferation of techniques, submucosal dissection will become the standard therapy for these tumors (8-11). On the other hand, even though in our service approximately 20% of cases of gastric cancer are detected in early stages, we are still far from reaching the 60% figures (12) of Japanese series. Nevertheless, we believe that with screening, training of gastroenterologists, and motivation for detection of these lesions we can reach these figures. This would radically change the burden of this disease in our environment.
REFERENCES
1. Hauser G. Das chronishe magensgeschwur, sein vermarbungsprocess un dessen beziehungen zur entwicklung des magenkarcinoma. Leipzig: FCW Vogel; 1883. [ Links ]
2. Versé M. Uber die entstenung, den bau und das waschstum der polypen, adenome und karcinome des magen-darmkanals. Arb Pathol Inst Leipzig 1908; 1: 40. [ Links ]
3. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma. 2nd English ed. Tokyo: Kanehara; 1998. [ Links ]
4. Gómez M. Otero W, Arbeláez V. Tratamiento endoscópico de cáncer gástrico temprano en Colombia con seguimiento a cinco años. Rev Col Gastroenterol 2009; 24: 347-352. [ Links ]
5. Tsukuma H, Ohshima A, Narahara H, et al. Natural history of early gastric cancer: a non-concurrent, long-term, follow-up study. Gut 2000; 47: 618-621. [ Links ]
6. Piñeros M, Ferlay J, Murillo R. Incidencia estimada y mortalidad por cáncer en Colombia. Instituto Nacional de Cancerología; 2005. [ Links ]
7. Ohshiba S, Ashiba K, Tanaka M, et al. Curative endoscopic resection of early gastric cancer: the possibility of extending its indications. Stomach Intest 1993; 28: 87-98. [ Links ]
8. Rembacken BJ, Gotoda T, Fujii T, et al. Endoscopic mucosal resection. Endoscopy 2001; 33: 709-718. [ Links ]
9. Soetikno R, Gotoda T, Nakanishi Y, et al. Endoscopic mucosal resection. Gastrointest Endosc 2003; 57: 567-579. [ Links ]
10. Soetikno R, Kaltenbach T, Yeh R, et al. Endoscopic mucosal resection for early cancers of the upper gastrointestinal tract. J Clin Oncol 2005; 4490-4498. [ Links ]
11. Gotoda T. Endoscopic resection of early gastric cancer. Gastric Cancer 2007; 10: 1-11. [ Links ]
12. Yamashita K, Sakuramoto S, Nemoto M, Shibata T, Mieno H, Katada N, Kikuchi S, Watanabe M. Trend in gastric cancer: 35 years of surgical experience in Japan. World J Gastroenterol 2011; 17(29): 3390-7. [ Links ]
