










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.30 no.1 Bogotá Jan./Mar. 2015
Hepatitis B Infections in Individuals with Exposure Factors in Quibdo and Apartado, Colombia
David Ríos Patiño MD. (1), Diana di Filippo V. MSc. (1), Margarita Insuasty E. MD. (1), Julio C. Rendón L. MSc. (1), Wilson Alfredo Ríos O. MSc. (1), Carlos Medina L. Biol. (1), María Cristina Hoyos MSc. (1), Carlos Julio Montoya G. MD. PhD. (2), María Cristina Navas N. MSc. PhD. (1)
(1) Gastro Group, Faculty of Medicine, Universidad de Antioquia in Medellin, Colombia.
(2) Fundación Antioqueña de Infectología. Immunovirology Group, Universidad de Antioquia in Medellin, Colombia.
Source of financial support: Strategy for Sustainability, Vice-Rector for Research, Universidad de Antioquia and Bristol-Myers Squibb.
Presentation of project results: IV National Virology Symposium, November, 2011 in Medellin, Colombia.
Received: 23-05-14 Accepted: 02-02-15
Abstract
Introduction: Colombia has a varied geographical pattern of prevalence of hepatitis B virus (HBV) infections with regions of high, moderate and low prevalences.
Objective: The objective of this study was to identify cases of HBV infection and characterize viral genotypes in population with factors of exposure in the cities of Quibdo and Apartado, Colombia.
Materials and Methods: The study population included 768 asymptomatic individuals with factors of exposure to HBV infections. An HBV surface antigen (HBsAg) rapid detection test was the first test used. Samples from individuals who tested positive were tested with ELISA to confirm the diagnosis and with PCR to detect the HBV genome. Viral genotypes were determined by sequencing and phylogenetic analysis.
Results: Seventeen individuals (17/768, 2.2%) were diagnosed with HBV infections by both the Rapid Test and Elisa. Phylogenetic analyses allowed identification of genotypes F (F3 and Subgenotype F1a) and A in the samples.
Conclusions: We report for the first time the presence of the F1a subgenotype in Colombia and confirme the presence of subgenotype F3 and genotype A.
Keywords
Hepatitis B, Epidemiology, risk factors, genotypes.
INTRODUCTION
Globally, infection with Hepatitis B Virus (HBV) is a public health problem. In January, te World Health Organization (WHO) estimated that there are more than 240 million cases of chronic HBV infections. HBV carries the risk of developing into cirrhosis and hepatocellular carcinoma (HCC) (1).
HBV is classified in the Hepadnaviridae family. Its genome consists of a circular DNA (deoxyribonucleic acid) molecule that is a partial double strand encoding seven proteins (surface antigens (HBsAg), core antigens (HBcAg), antigen E, viral polymerase and protein X) (2, 3).
The prevalence of HBsAg was used to define the country's regions as having low, intermediate or high levels of HBV endemicity (4). Colombia has a heterogeneous pattern of prevalence, but as of April, its overall endemicity was considered to be moderate (4).
Currently ten HBV genotypes have been characterized (genotypes A through J) (5-8). A correlation between certain genotypes of HBV and variables such as transmission efficiency, tendency to chronicity, response to antiviral therapy and progression to cirrhosis and HCC has been suggested (9). For example, genotype C is associated with a higher risk of HCC than is genotype B. Also, infections with genotypes A and B respond better to interferon treatment than do infections with genotypes C and D (9).
Studies of blood donors and patients with terminal liver disease have identified Genotype F and subgenotype F3 as the most frequently occurring genotypes in Colombia. In addition, genotypes A, D, C and G have been described, but at lower frequencies (10-12). Genotype E has been identified in pregnant Afro-Colombian women, and subgenotype F1b has been identified among indigenous people (13-15).
This study aims to identify cases of HBV infection and characterize viral genotypes in an asymptomatic population with exposure factors in the municipalities of Quibdó and Apartadó, Colombia.
MATERIALS AND METHODS
Study Population
Between September and November 2009, a study was conducted in an asymptomatic population in Quibdó, the capital of the department of Chocó, and Apartadó, a municipality in Antioquia Department. The study population was selected by the hospitals in these cities according to risk factors such as blood transfusion, surgery, sexually transmitted diseases (STDs) and family histories of hepatitis. Prior to signing of informed consent form by patients, or a parent or guardian in the case of minors, a researcher explained the purpose of the study. After administration of the HBsAg rapid detection test, a researcher provided advice participants who tested positive. The researcher explained HBV infection risk factors, the likelihood of chronic infection, sequelae of infection, testing to confirm the diagnosis, and treatment. The study was approved by the ethics committee of the Fundación Antioqueña de Infectología.
Rapid Test for detection of HBsAg
A total 768 people in urban and rural areas of Apartadó and Quibdó agreed to participate in the study. A sample of whole blood was obtained by puncture with a lancet from each of the participants, and a rapid test for the detection of HBV surface antigen (HBsAg) (One Step HBsAg Rapid Test Kit) (Intec, China) was performed according to the manufacturer's recommendations.
All participants filled out an initial survey about socio-demographic variables. A second survey that included socio-demographic variables and risk factors was filled out for each of the participants who tested positive when the HBsAg rapid test was performed. Subsequently, a peripheral blood sample by venipuncture from each individual was obtained, and serum was obtained by centrifugation and stored at -70o C.
All samples from participants who tested positive were confirmed by Elisa (HBsAg confirmatory, Abbott), and the patients were referred to health centers in Quibdó (DASALUD) and Apartadó (Secretary of social protection) for monitoring and treatment.
Detection of Viral Genome
All DNA from serum samples was extracted by the Trizol method (Invitrogen, USA), following the instructions of the manufacturer. Open reading frame (ORF) S of HBV (S region, nucleotides 203-787) was amplified. Amplification conditions were adapted from published protocols (16). Both rounds of PCR reaction were performed in final volumes of 25ul (1X Buffer, 50 mM MgCl2, 2.5 mM dNTPs (Promega), 10 uM primers and 50 U/ul of Biolase DNA polymerase (Bioline)). In the first round of PCR, S1R and PRsS2 primers were used. In the second round, YS1 and YS2 were used. (16) PCR conditions were 93° C for 3 min, 35 cycles at 94° for 45 sec, 53° C for 1 min, 72 ° C for 1:30 min, and a final extension step at 72 ° C for 6 min. The amplified fragment of 585 base pairs (bp) was visualized on 2% agarose gel stained with ethidium bromide. DNA obtained from a liver explant (TH79) from a patient with chronic HBV infection was used as a positive control of testing. Nuclease free water (Invitrogen, Ambion® Nuclease-Free Water) was used as the negative control.
Genotyping of HBV
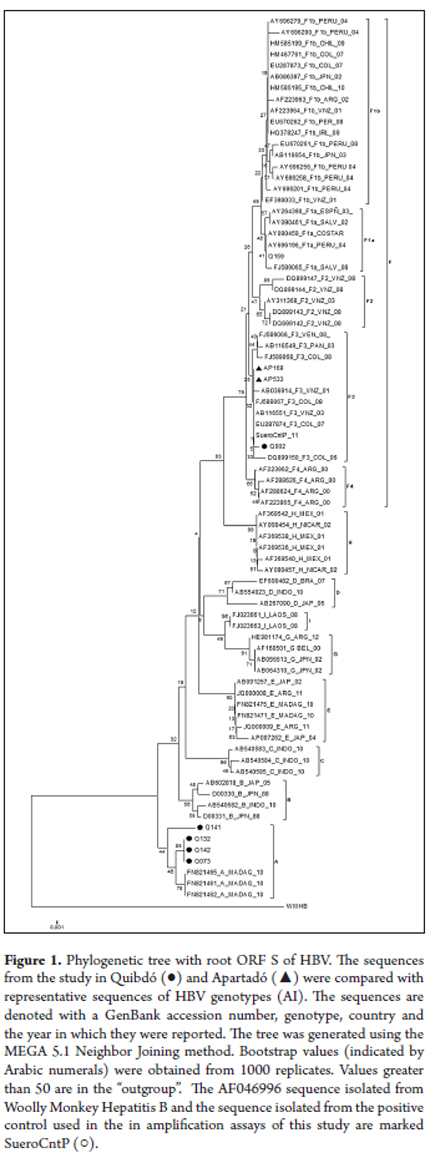
PCR products were purified and sequenced by the automated dideoxynucleotide method (Big Dye TM Terminator, Macrogen, Korea). The sequences obtained were compared to published HBV sequences from the GenBank. Sequences were aligned with ClustalW which is contained in Bioedit 7.0.5.3. Phylogenetic analysis was done with the Neighbor Joining and Maximum Parsimony method using MEGA 5.0 with 80 HBV sequences from GenBank. The reliability of the trees was evaluated using bootstrap values from 1,000 replicates.
Statistical Analysis
An Excel database was developed with the information obtained from the surveys and was subsequently analyzed using EPI-INFO and EPI-DAT. The prevalence ratio was calculated with a 95% confidence interval considering p <0.05 to be statistically significant.
RESULTS
Study Population
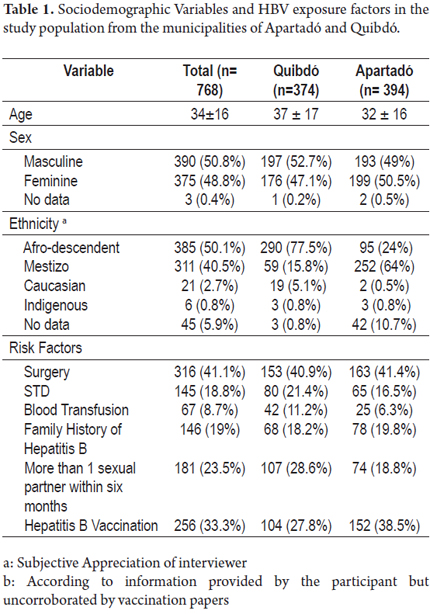
A total of 768 individuals participated in the study, 394 people (51.3%) enrolled during a visit to Apartadó and 374 people (48.6%) enrolled during two visits to Quibdó. Of the study population, 50.8% were male and 49.2% were female: the average age was 34 years with a 95% CI of 23 to 45.
The main factors of HBV exposure in the study population were surgery (41.1%), more than one sexual partner in the last six months (23.4%), STDs (18.7%), family histories of hepatitis (18.9%) and blood transfusions (8.6%). According to the surveys, at least 1 dose of hepatitis B vaccine had been received by 59.3% of the participants although it is worth mentioning that this information was not corroborated by vaccination papers. There were marked differences in vaccinations reported: 43.1% in Quibdó and 75.2% in Apartadó (Table 1).
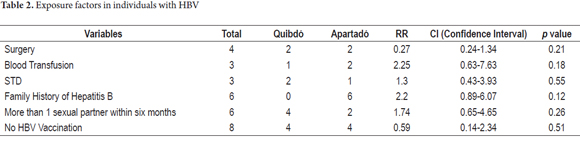
Of the total population, 17 individuals (2.2%) tested positive with the HBsAg Rapid Test and ELISA. Eight (2.03%) were from Apartadó, and nine (2.4%) were from Quibdó. The average age of those who tested positive was 18 years with an age range of 19 to 77 years. Ten of those who tested positive were 10 men, and seven were women. The two main exposure factors of in the 17 cases were the absence of vaccination (8 cases) and family histories of hepatitis (6 cases). This second factor was so important in this study because five of the cases involved members of the same family in Apartadó, while in Quibdó none of the cases were related to each other (Table 2). Other exposure factors identified were surgery (4 cases), blood transfusions (3 cases) and STDs (3 cases).
Detection of Viral Genome and HBV Genotypes
The viral genomes of eight out of the seventeen (47.05%) serum samples from the individuals who tested positive with the HBsAg rapid test were amplified. This frequency of detection may be due to serum viral loads lower than the detection limit for the amplification technique (100 IU/mL) (16).
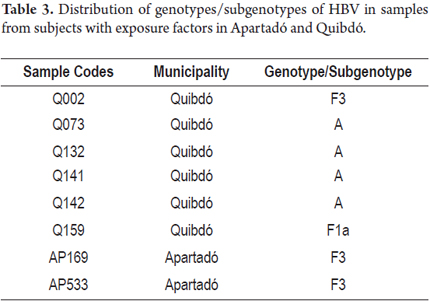
Phylogenetic analyses of the sequences showed the presence of genotype F in four samples (50%) of which three samples were identified as subgenotype F1b, and one was identified as subgenotype F1a. The four remaining samples (50%) were all characterized as genotype A. All samples from the municipality of Apartadó were genotype F, subgenotype F3. Four of the samples from Quibdó were classified as genotype A and two samples were classified as genotype F, one of which was subgenotype F3 while the other was subgenotype F1a (Table 3).
DISCUSSION
Quibdo's population of 162,803 inhabitants consists mainly of people of African descent with varying degrees of mixture with other groups. Apartadó is located in northwestern Antioquia and has a population of 148,745 inhabitants. It is characterized by an ethnic mix of Afro-descendants, mestizos, and caucasians.
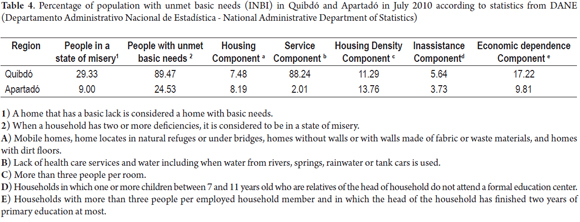
The socioeconomic conditions of Quibdó and Apartadó differ as evidenced by the Index of Unsatisfied Basic Needs (NBI). In 2010, the percentage of the population with unsatisfied basic needs in Quibdó was 89.47% while it was only 24.53% in Apartadó. This difference has persisted historically. The percentage of the population living in poverty in Quibdó is well above the national average of 18.5% and is three times the percentage in Apartadó (Table 4) (17).
From 1976 to 1998, 53.2% of the departments of Colombia, including the departments of Antioquia and Choco, were classified as areas of high endemicity for HBV infections (18, 19). From 1998 to 2007, epidemiological information comes from population surveys, occasional notifications, and data nested in sentinel studies of other STDs and does not represent the real situation of HBV (20). Since 2007, the National Institute of Health has provided information derived from individual reports of HBV. The reported incidences in the departments of Antioquia and Chocó from 2008 to 2012 may be due to the quality of reporting (Table 5) (21).
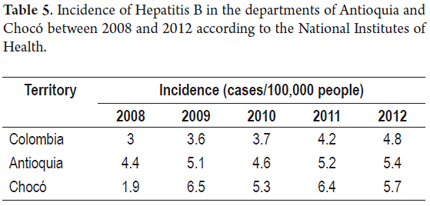
As of the fifth week of 2013, the incidence of Hepatitis B in Colombia was 1.84 cases per 100,000 inhabitants, but there were great variations among the country's regions. The incidence of HBV in the department of Antioquia in 2013 was 2.29 cases per 100,000 people while in Choco it was 3.06 cases per 100,000 people (22).
In this study 17 cases (2.2%) of HBV infections were identified from a total of 768 individuals with risk factors. The percentage in Apartadó was 2.03% while it was 2.4% in Quibdó.
Prevalence studies of HBV in Quibdó and Apartadó in 1987 and 1988 reported a frequency of HBsAg of 11% in the general population and among health personnel in Apartadó and in two other municipalities in the region of Urabá, as well as a prevalence of 7% in the rural population of Quibdó (19, 20).
As mentioned in the methodology section, cases of HBV were first identified with a rapid test for HBsAg the technical specifications of which state that is has high sensitivity and specificity. Nevertheless, this research group evaluated the test's sensitivity and specificity in a separate study after this study was complete. This validation was performed by analysis of 60 serum samples. Using ELISA, forty-two had tested positive for HBsAg and anti-HBc while eighteen had negative serological markers for hepatitis B. The rapid test identified eight out of forty-two (19%) of the HBsAg positive samples confirmed eighteen (100%) of the negatively diagnosed samples. According to these results, the rapid test has a sensitivity of 55.2% and a specificity of 100%. These data suggest that some proportion of samples from HBV infected individuals were not identified by the rapid test. Although high test specificity (100%) and ease of administration for evaluating large study populations in a short time are two advantages of this technique in the field, its low sensitivity (55.2%) is a disadvantage that limits its use for identifying cases of HBV infection (14).
The frequency of HBV found by the rapid test in the study population (2.2%, 17/786) is similar to the frequency observed in an asymptomatic indigenous population in the department of Amazonas (2.6%, 23/862) using the same rapid test in a recent study performed by this research group (14).
Cases of HBV infection in this study correspond to a fraction of this at-risk population. The cases of HBV infection identified by rapid test probably correspond to individuals with higher viral loads than other cases which remained undetected.
The differences in the frequency of exposure factors between these two both populations, may be due to the different epidemiological and sociocultural profiles of Quibdó and Apartadó. Most of the cases in Apartadó occurred in members of the same family, a women and four of her ten children. They had previously lived in the city of Quibdó for at least 13 years, and all of them had refused to be vaccinated against HBV. They lived in overcrowded conditions with shared kitchen utensils. In addition, three of these people reported having family contacts with a person with hepatitis.
Familial transmission may be a significant risk variable in the city of Quibdó, as it was in the decade of the 1980's (18, 19).
In addition, the country decentralized its health care system beginning in 1997. Autonomy was granted to local authorities to manage public health programs. This measure resulted in very significant decreases in vaccination coverage which had reached 76% for HBV before the decentralization was implemented. Decreases in vaccination coverage were greater among the populations with unmet basic needs. From 1994 to 2010, the percentage of coverage for the vaccine against HBV in the department of Chocó were lower than 75%. This suggests that vaccination against HBV in Colombia is an effective program to prevent hepatitis B, but coverage must be maintained and should be extended to other age groups (23).
In this study we demonstrate the presence of genotype F (4/8; 50%), subgenotype F3 (3/4; 75%) subgenotype F1a (1/4; 25%), and genotype A (4/8; 50%) (Figure 1).
A study of blood donors in the cities of Bogota and Bucaramanga found a predominance of genotype F (subgenotype F3) (86%; 43/50) with lower frequencies of genotype D (8%; 4/50), C (2%; 1/50) and G (2%; 1/50) 10. Cortes, Mancera and colleagues have characterized HBV isolated from patients diagnosed with cirrhosis and/or HCC and found a predominance of genotype F, subgenotype F3 (83.3%; 5/6) in the study population. Subgenotype F1a (16.7%; 1/6) was described in a sample from a foreign patient from El Salvador (11).
This study describes for the first time the circulation of subgenotype F1a in Colombia. This finding was unexpected because subgenotype F1a had previously been described only in Central America (9). However, recently some isolates of this subgenotype have been described in South American countries such as Peru (24). The results of this and these other studies suggest that subgenotype F1 is circulating in South American countries as a minority variant.
Recently, Alvarado and colleagues identified HBV genotypes in samples of blood donors in Bogotá, Bucaramanga, Neiva, Tunja and Pasto. Genotype F was the most prevalent (77%; 40/52) which included subgenotype F3 (75%; 39/52), followed by genotype A2 (15.3%; 8/52) and genotype G (7.7%, 4 / 52). In addition, the circulation of subgenotype F1b was described in 2% (1/52) of the samples. (12) Two recent studies describe genotype F1b in the indigenous population of the department of Amazonas (14, 15, 25).
The predominance of genotype F in South and Central America suggests that it is indigenous to the Americas (26-29). In fact, its distribution is directly related to migration patterns and to the dispersal of the first settlers of the Americas. Genetic studies suggest that populations of Colombia and Venezuela have a larger Amerindian genetic component (90%) than do Brazilian populations in which genotypes A and D are the most common. (30-34). This would explain the predominance of genotype F in Colombia and Venezuela.
On the other hand, genotype A has been reported in some South American countries like Venezuela and Brazil, specifically in African-descendant populations. Some researchers suggest that genotype A may have been introduced in America through the slave trade in African people during the eighteenth century (31). This would explain the fact that this HBV genotype was most frequent in Quibdó where most of the people are of African descent.
CONCLUSION
In conclusion, seventeen cases of infection were identified in the study population by the rapid HBV test. All were older individuals. The circulation of genotypes F and A in these populations is consistent with what has been reported by previous studies in Colombia in which the ethnic diversity of these regions seems to influence the geographic distribution of genotypes. Additional studies are needed to establish the importance of certain risk factors such as familial transmission of HBV in the town of Apartadó.
Acknowledgements
Sustainability Strategy for 2009-2010 of the Office of the Vice-Rector for Research at the Universidad de Antioquia; Bristol-Myers Squibb Pharmaceutical Company; Fundación Antioqueña de Infectología.
REFERENCES
1. World Health Organization. Hepatitis B Fact Sheet [Internet]. World Health Organization. 2013 [citado 28 de abril de 2014]. Recuperado a partir de: http://www.who.int/mediacentre/factsheets/fs204/en/ [ Links ]
2. Lee WM. Hepatitis B virus infection. N Engl J Med 1997;337(24):1733-45. [ Links ]
3. Moolla N, Kew M, Arbuthnot P. Regulatory elements of hepatitis B virus transcription. J Viral Hepat 2002;9(5):323-31. [ Links ]
4. Seeger C, WS Mason. Hepatitis B virus biology. Microbiol Mol Biol Rev 2000;64(1):51-68. [ Links ]
5. Ott, J, Stevens GA, Groeger J, Wiersma ST. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine 2012;30(12). [ Links ]
6. Franco E, Bagnato B, Marino MG, Meleleo C, Serino L, Zaratti L. Hepatitis B: Epidemiology and prevention in developing countries. World Journal of Hepatology 2012;4(3):74. [ Links ]
7. Instituto Nacional de Salud [sitio web]. Bogotá: Robayo Rico RE; 2010 [acceso 19 de diciembre de 2012]. Informe epidemiológico de evento, Hepatitis B. Disponible en: http://www.ins.gov.co/lineas-de-accion/Subdireccion-vigilancia/Informe%20de%20Evento%20Epidemiolgico/Hepatitis%20B%202010.pdf [ Links ]
8. Norder H, Couroucé AM, Coursaget P, Echevarria JM, Lee SD, Mushahwar IK, et al. Genetic diversity of hepatitis B virus strains derived worldwide: genotypes, subgenotypes, and HBsAg subtypes. Intervirology 2004;47(6):289-309. [ Links ]
9. Tanwar S, Dusheiko G. Is there any value to hepatitis B virus genotype analysis? Curr Gastroenterol Rep 2012;4(1):37-46. [ Links ]
10. Cortes-Mancera F, Loureiro CL, Hoyos S, Restrepo JC, Correa G, Jaramillo S, et al. Etiology and viral genotype in patients with end-stage liver diseases attended in a Hepatology unit in Colombia. Hepatitis Research and Treatment 2011. 2011:363205. doi: 10.1155/2011/363205. Epub 2011 Sep 20. [ Links ]
11. Devesa M, Loureiro CL, Rivas Y, Monsalve F, Cardona N, Duarte MC, et al. Subgenotype diversity of hepatitis B virus American genotype F in Amerindians from Venezuela and the general population of Colombia. J Med Virol 2008;80(1):20-6. [ Links ]
12. Alvarado Mora MV, Romano CM, Gomes-Gouvêa MS, Gutierrez MF, Botelho L, et al. 2011. Molecular characterization of the Hepatitis B virus genotypes in Colombia: a Bayesian inference on the genotype F. Infect Genet Evol 2011;11(1):103-8. [ Links ]
13. Alvarado Mora MV, Romano CM, Gomes-Gouvêa MS, Gutierrez MF, Carrilho FJ, Pinho JR. Molecular epidemiology and genetic diversity of hepatitis B virus genotype E in an isolated Afro-Colombian community. J Gen Virol 2010;91(Pt 2):501-8. [ Links ]
14. Di Filippo, D. Infección por el virus de la hepatitis B y el virus de la hepatitis D en comunidades indígenas del departamento del Amazonas. (Tesis de Maestría). Medellín, Universidad de Antioquia; 2013. [ Links ]
15. Alvarado-Mora MV, Romano CM, Gomes-Gouvêa MS, Gutierrez MF, Carrilho FJ, Pinho JR. Dynamics of hepatitis D (delta) virus genotype 3 in the Amazon region of South America. Infect Genet Evol 2011;11(6):1462-8. [ Links ]
16. Zeng GB, Wen SJ, Wang ZH, Yan L, Sun J, Hou JL. A novel hepatitis B virus genotyping system by using restriction fragment length polymorphism patterns of S gene amplicons. World J Gastroenterol 2004;10(21):3132-6. [ Links ]
17. DANE [sitio web]. Bogotá: 2009 [acceso 23 de julio de 2012]. Índice de necesidades básicas insatisfechas. Disponible en: http://www.dane.gov.co/index.php/estadisticas-sociales/necesidades-basicas- insatisfechas-nbi [ Links ]
18. Padilla JC, Arriaga AL. Hepatitis A, B y D en Chocó. Biomédica 1997;17(4):286-91. [ Links ]
19. Arboleda M, Jaramillo C, Echeverry ML, Arbeláez MP, Gutierrez F, Yaruro C, Muriel AJ, et al. Un nuevo Foco de hepatitis fulminante por virus delta. Urabá, Colombia - 1987. Bol EpiAnt 1987;12(4):339. [ Links ]
20. Instituto Nacional de Salud [sitio web]. Bogotá; 2000-2008 [acceso 15 de julio de 2012]. Informe epidemiológico de evento, Hepatitis B. Disponible en: http://www.ins.gov.co/lineas-de-accion/Subdireccion-Vigilancia/Paginas/informes-de-evento.aspx [ Links ]
21. Instituto Nacional de Salud [sitio web]. Bogotá; 2007-2012 [acceso 19 de julio de 2012]. Informe epidemiológico de evento, Hepatitis B. Disponible en: http://www.ins.gov.co/lineas-de-accion/Subdireccion-Vigilancia/Paginas/informes-de-evento.aspx [ Links ]
22. Instituto Nacional de salud. [sitio web]. Bogotá; 2013. [acceso de Agosto de 2013]. Reporte de evento periodo V del 2013. Disponible en: http://www.ins.gov.co/lineas-de-accion/Subdireccion-Vigilancia/Informe%20de%20Evento%20Epidemiolgico/HEPATITIS%20B%20Y%20C%20Periodo%20V%202013.pdf [ Links ]
23. Organización Panamericana de la Salud [sitio web]. Bogotá: Muñóz S; 2000 [acceso 19 de marzo de 2013]. Coberturas de vacunación. Disponible en: http://www.col.ops-oms.org/pai/coberturas.htm [ Links ]
24. National Center for Biotechnology Information, (NCBI), National Library of Medicine [acceso 2 de noviembre de 2013]. Hepatitis B virus isolate HBV-L29 envelope protein (HBsAg) gene, partial cds. Disponible en: http://www.ncbi.nlm.nih.gov/nuccore/ay696196 [ Links ]
25. Jaramillo CM. Identificación de variantes de escape del VHB en individuos de comunidades indígenas en el departamento de Amazonas. (Tesis de Maestría). Medellín, Universidad de Antioquia; 2013. [ Links ]
26. Blitz L, Pujol FH, Swenson PD, Porto L, Atencio R, Araujo M, et al. Antigenic diversity of hepatitis B virus strains of genotype F in Amerindians and other population groups from Venezuela. J Clin Microbiol 1998;36(3):648-51. [ Links ]
27. Nakano T, Lu L, Hu X, Mizokami M, Orito E, Shapiro C, et al. Characterization of hepatitis B virus genotypes among Yucpa Indians in Venezuela. J Gen Virol 2001;82(2):359-65. [ Links ]
28. Campos RH, Mbayed VA, Pineiro FG. Molecular epidemiology of hepatitis B virus in Latin America. J Clin Virol 2005;34(Suppl 2):S8-S13. [ Links ]
29. Bedoya G, Montoya P, García J, Soto I, Bourgeois S, Carvajal L, et al. Admixture dynamics in Hispanics: A shift in the nuclear genetic ancestry of a South American population isolate. Proc Natl Acad Sci USA 2006;103:7234-9. [ Links ]
30. Martínez H, et al. Admixture estimates for Caracas, Venezuela, based on autosomal, Y-chromosome, and mtDNA markers. Human Biol 2007;79(2):201-13. [ Links ]
31. Devesa M, Pujol FH. Hepatitis B virus genetic diversity in Latin America. Virus Res 2007;127:177-84. [ Links ]
32. Carvalho-Silva DR, Santos FR, Rocha J, Pena SD. The phylogeography of Brazilian Y-chromosome lineages. Am J Hum Genet 2001;68:281-86. [ Links ]
33. Nabuco LC, Mello FC, Gomes S de A, Perez RM, Soares JA, Coelho HS, et al. Hepatitis B virus genotypes in Southeast Brazil and its relationship with histological features. Mem Inst Oswaldo Cruz 2012;107:758-89. [ Links ]
34. Días AL, Oliveira CM, Castilho Mda C, Silva Mdo S, Braga WS. Molecular characterization of the hepatitis B virus in autochthonous and endogenous populations in the Western Brazilian Amazon. Rev Soc Bra Med Trop 2012;45:9-12. [ Links ]
