










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.30 no.3 Bogotá July/Sept. 2015
Three varieties of Kaposi's sarcoma with gastrointestinal involvement
Karina Jiménez MD. (1), Julián D. Martínez MD. (2), Geovanny Hernández MD. (3), Martín A. Garzón MD (3), Natán Hormaza MD. (3), Jorge Iván Lizarazo MD. (3), Juan Carlos Marulanda MD. (3), Juan Carlos Molano MD. (3), Mario H. Rey MD. (3), Martín Gómez Zuleta MD. (2)
(1) Internal Medicine Resident at the Universidad de la Sabana and the Hospital Universitario de la Samaritana in Bogotá, Colombia.
(2) Faculty of Medicine of the National University of Colombia in Bogotá, Colombia.
(3) Gastroenterology Unit of the Hospital Universitario de la Samaritana in Bogotá, Colombia.
Received: 29-09-14 Accepted: 21-07-15
Abstract
This article presents the cases of four adult patients with three varieties of Kaposi's sarcoma: epidemic, associated with human immunodeficiency virus infections; iatrogenic, associated with chronic immune suppression (and in this case in a man with alcoholic cirrhosis); and classic, occurring in elderly patient without previously known immunosuppression. All four cases had gastrointestinal involvement. A brief review of the disease is included.
Keywords
Kaposi's sarcoma, sarcoma, gastrointestinal compromiso.
INTRODUCTION
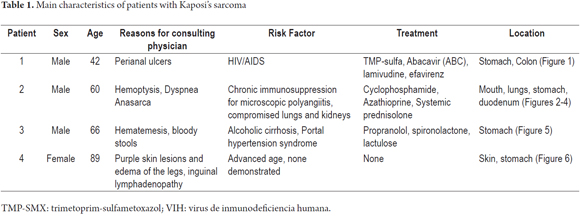
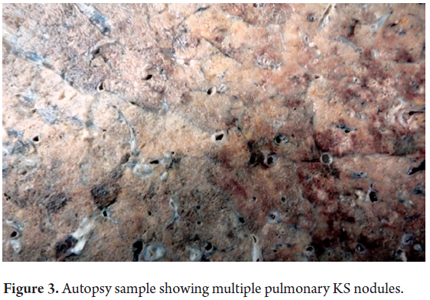
Kaposi's sarcoma (KS) is a complex malignant tumor of mesenchymal origin which is associated with human herpes virus 8 (KSHV). It normally coincides with an immune disorder that promotes an environment that is ideal for its development (1, 2). There are four types of KS: classical, endemic, African and iatrogenic. The endemic and African types have specific racial and geographic distributions, are more benign, and are associated with HIV/AIDS. To date, iatrogenic KS has been described in close association with immunosuppression used with transplantation and has the worst prognosis. The most common location of KS is in the skin. The second most common is in lymph nodes, and in third place is the gastrointestinal tract. Endoscopic indications vary from ulcers to purple nodular submucosal lesions. The most important histological indications are vascular proliferation characterized by the presence of vascular slits, extravasation of erythrocytes with hemosiderin deposits, and immunohistochemistry that is positive for herpes virus-8 (1-5).
CASE PRESENTATIONS
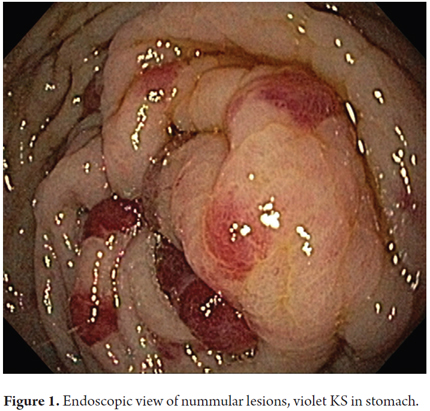
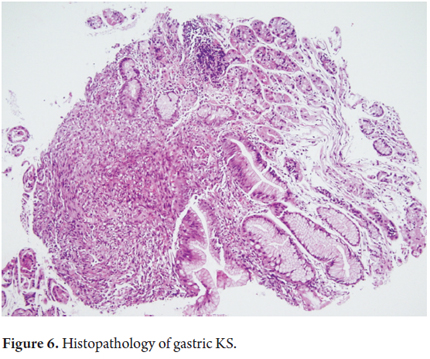
We present the cases of four patients with histologically confirmed Kaposi's sarcoma who were treated in the gastroenterology unit of the Hospital Universitario de la Samaritana in Bogotà, Colombia in 2012 and 2013. For educational purposes, Table 1 summarizes the most important characteristics of the patients and macroscopic and microscopic findings from these cases. Figures 1, 2, 3, 4, 5 y 6.


DISCUSSION
In 1872, the Hungarian dermatologist Moritz Kaposi described five patients who had "sarcoma idiopaticum multiplexhemorrhagicum" with compromised blood and lymph vessels. This was the first time the disease was described so it was later named him as Kaposi's sarcoma (KS) (6). There are several types of KS. The classic type is usually diagnosed in elderly patients in Mediterranean populations or descendants of Jews from Eastern Europe. It grows slowly and consists mainly of skin lesions affecting the lower limbs. The endemic type of KS has been described in black preadolescents and youth in sub-Saharan Africa. The epidemic type is associated with HIV/AIDS and has a gender ratio of compromise of 10 men to each woman affected. The risk of developing this type of KS is highest among homosexual men and those with low CD4 counts and high viral loads. The iatrogenic type of KS is secondary to immunosuppressant drugs, especially their use in treating diseases and in transplantation with most reports related to kidney transplants. Although the histology of the different types of KS is identical, the outcomes are different. KS associated with HIV/AIDS has the worst prognosis due to its rapid development and usually fatal outcome (1, 2, 6).
KS has been associated with infection by human herpes virus 8 (HV-8). The virus was described in 1994 and later found to be associated with KS leading to the use of the initials KSHV. In 2010 it was declared to be a Group I carcinogen by the International Agency for Research on Cancer (IARC) (7).
The prevalence of KSHV infection varies from place to place throughout the world. Areas in which it is endemic are associated with HIV/AIDS, but after the association of KS and HV was discovered its diagnosis increased dramatically. Rates of diagnosis subsequently stabilized after introduction of effective antiretroviral therapy (8). Although the overall seroprevalence of herpes virus-8 is not well known yet because of the great regional variability, it is estimated that the incidence of KS among HIV/AIDS patients is 20,000 times higher than in the general population and 300 times higher than among people with other causes of immunosuppression (9). KS accounts for 60% of the tumors diagnosed in patients with HIV/AIDS (2, 8, 9).
For the year 2012, the Colombian National Public Health Monitoring System (Sistema Nacional de Vigilancia en Salud Pública SIVIGILA) estimated that 122,197 people had HIV/AIDS in this country, but no specifics are known for KS. Saldarriaga and colleagues published a study which assessed patients with KS and HIV/AIDS in Cali between 1962 and 2007. The study was based on the population register of cancer patients and data from SIVIGILA. The time period with the highest rate of diagnosis for men, four per 100,000, was between the years 1996 and 2002. After 2002, diagnoses of extracutaneous KS increased from a previous level of was only 10% (10). We have no statistical data regarding the diagnosis of iatrogenic KS in Colombia. There are data in the literature indicating that classic KS accounted for 1% of neoplasms in patients with a mean age of 65 years for the year 1985 (11). In Medellin, Orozco and colleagues published a study that used the immunofluorescence technique to test the relationship between KS and HHV-8. The study found that 83.3% of a group of patients with KS and HIV/AIDS were positive for antibodies to HHV-8 (12).
The literature has frequently documented cases of Kaposi's sarcoma associated with HIV/AIDS. These are predominantly cases of skin lesions or lesions in visible mucous oral or pharyngeal membranes suspected of being KS and subsequently confirmed histopathologically (13). There are currently no international recommendations for active pursuit of the systemic disease. When there is gastrointestinal compromise, it is usually diagnosed incidentally and not as the result of direct suspicion of its existence. Although indications for performance of endoscopic studies on immunosuppressed patient are not different from those for their performance on immunocompetent patients, more than 50% of HIV/AIDS patients have gastrointestinal symptoms and the causative etiology is likely to be associated with an opportunistic infection (2, 13). KS with gastrointestinal involvement may be asymptomatic, but abdominal pain, gastrointestinal bleeding and even intestinal obstruction may present, and these symptoms are indications for endoscopic study. Endoscopic findings vary from purple or red submucosal nodules and plaques to polypoid formations (3, 14).
The first case reported here raises the question as to whether or not a patient who has been diagnosed with an advanced stage of HIV/AIDS but who does not have gastrointestinal symptoms should be subjected to gastrointestinal tract endoscopy as a screening test. This is especially relevant since it has been documented that up to 15% of patients with visceral KS do not occur have gastrointestinal compromise, so there is a likelihood of gastrointestinal KS despite the absence of skin lesions (15).
Very few cases of iatrogenic Kaposi's sarcoma have been reported in publications. Most are related to drug immunosuppression for rheumatologic diseases. In general, there are multiple reports of iatrogenic KS associated with transplants. In the English language literature, there are a few cases of patients who have been chronically immunocompromised pharmacologically with steroids and azathioprine and who have been diagnosed with ulcerative colitis, systemic lupus erythematosus and vasculitis (16,17).
In the Latin American literature in LILACS (Literatura Latino-Americana e do Caribe em Ciências da Saúde) on-line medical and health science bibliographic database, some cases of iatrogenic KS in patients who have been chronically immunosuppressed with steroids for kidney transplants have been reported (18, 19). The second case that we report is rare. The immense magnitude of the compromise that triggered the death of the patient suggests that patients with immunosuppression from causes other than HIV/AIDS, especially those with drug-induced immunosuppression associated with autoimmune diseases, are more susceptible to infection with HHV-8 and its manifestation as KS. This implies that the comorbidity worsens their prognosis. It also implies that prevalence may be increasing due to the progressively increasing diagnosis of rheumatic diseases and the early use of immunosuppressive therapies and to the increasing number of transplants of various organs and the higher survival rates achieved by these patients in our country.
The third case reported is a clarion call to consider that systemic diseases such as cirrhosis and alcoholism, which are frequent in our environment, lead to impaired immune function, to increased susceptibility to viral infections, and to development of gastrointestinal malignancies such as KS. This is in addition to the high frequency of squamous tumors of the mouth and esophagus and to gastric and pancreatic adenocarcinomas associated with these systemic diseases. Biopsies need to be taken from these patients from focal gastric lesions that are endoscopically similar to other vascular lesions such as portal hypertension gastropathy and gastric antral vascular ectasia (GAVE) syndrome (water melon stomach) (3, 5, 13, 14).
The last case presented demonstrates presence of classic KS in elderly patients with gastrointestinal compromise, lower limb edema and compromised inguinal lymph nodes. As reported in the literature, lower limb edema accompanies these lesions in 48% of cases, and compromised inguinal lymph nodes are found in 23% of these cases (20). This leads us to consider endoscopic diagnosis of possible gastrointestinal KS in elderly patients with cutaneous findings. This could be beneficial in terms of timely treatment with positive results for these patients.
REFERENCES
1. Schwartz RA, Lamber WC. Kaposi sarcoma. Medicine Oncology [home page on the internet] [Updated: Apr 23, 2009, cited 2010 Jun 20] [about 4 screens]. Available from: http://emedicine.medscape.com/e medicine\Kaposi Sarcoma eMedicine. [ Links ]
2. Douglas Jl, Gustin JK, Moses A, Dezube BJ, Pantanowitz L. Kaposi sarcoma pathogenesis: A triad of viral infection, oncogenesis and chronic inflammation. Transl Biomed. 2010;14(7):172. [ Links ]
3. Martínez JD, Hernández G, Salinas C, Hormaza N, Garzón M, Lizarazo J, et al. Sarcoma de Kaposi gástrico en un paciente con virus de inmunodeficiencia humana (VIH): informe de caso. Rev Gastroenterol Perú. 2014;34:145-7. [ Links ]
4. Jiménez F, Barbaglia Y, Juárez L, Bucci P, Tedeschi F, Zalazar F. Sarcoma de Kaposi gastrointestinal asociado a síndrome de inmunodeficiencia adquirida. Descripción de un caso. Acta Gastroenterol Latinoam. 2011;41:308-11. [ Links ]
5. Taccogna S, Crescenzi A, Stasi R, Turrini L, Gallo A, Rossi Z. Kaposi sarcoma of the stomach: A case report. BMJ Case Rep. 2009: 2009.pii:bcr03.2009.1666. [ Links ]
6. Hengge UR, Ruzicka T, Tyring SK, et al. Update on Kaposis sarcoma and other HHV8 associated diseases. Part 1: Epidemiology, environmental predispositions, clinical manifestations, and therapy. Lancet Infect Dis. 2002;2(5):281-92. [ Links ]
7. Chang Y, Cesarman E, Pessin MS, Lee F, Culpepper J, Knowles DM, et al. Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposis sarcoma. Science. 1994;266:1865-9. [ Links ]
8. Rohner E, Wyss N, Trelle S, Mbulaiteye SM, Egger M, Novak U, et al. HHV-8 seroprevalence: A global view. Syst Reviews. 2014;12(3):11. [ Links ]
9. Mohanna S, Maco V, Bravo F, Gotuzzo E, Bhaijee F, Subramony Ch, et al. Epidemiology and clinical characteristics of classic Kaposis sarcoma, seroprevalence, and variants of human herpesvirus 8 in South America: A critical review of an old disease. Int J Infect Dis. 2005;9: 239-50. [ Links ]
10. Saldarriaga-Cantillo A, Bravo LE, Londoño O, García LS, Collazos P. Vigilancia epidemiológica del complejo VIH/SIDA a través del análisis de tendencia de la incidencia del sarcoma de Kaposi. Colomb Med. 2012;43(4):273-80. [ Links ]
11. García A, Olivella F, Valderrama S, Rodríguez G. Kaposi´s sarcoma in Colombia. Cancer. 1989;64:2393-8. [ Links ]
12. Orozco B, Gómez LM, Estrada S, Restrepo BN, Cataño JC. Relación entre el virus humano herpes 8 y el sarcoma de Kaposi en pacientes positivos y negativos para el VIH. Infectio. 2007;11(3):111-7. [ Links ]
13. Bhaijee F, Subramony Ch, Tang SJ, Pepper DJ. Human immunodeficiency virus-associated gastrointestinal disease: common endoscopic biopsy diagnoses. Pathol Res Int. 2011;2011:247923. [ Links ]
14. Sánchez del Monte J, Hernández-Guerrero A, Sobrino-Cossio S, Lárraga A, Sánchez-Benítez G, López Blanco P, et al. Manifestaciones clínicas y características endoscópicas del sarcoma de Kaposi en pacientes con síndrome de inmunodeficiencia adquirida. Rev Gastroenterol Mex. 2005;70(4):17-20. [ Links ]
15. Attia S, Dezube BJ, Torrealba JR, Sossman JM, Pau PR, et al. AIDS-related Kaposi´s sarcoma of the gastrointestinal tract. J Clin Oncol. 2010;28(6):e250-1. [ Links ]
16. Jakob L, Metzler G, Chen KM, Garbe C. Non-AIDS associated Kaposis sarcoma: Clinical features and treatment outcome. PLoS ONE. 2011;6(4):e18397. [ Links ]
17. Svrcek M, Tiret E, Bennis M, Guyot P, Fléjou JF. KSHV/HHV8-associated intestinal Kaposi´s sarcoma in patient with ulcertive colitis receiving immunosuppressive drugs: Report the case. Dis Colon Rectum. 2009;52(1):178-80. [ Links ]
18. Koche B, Hohmann C, Lima AC, Becker FL, Bonamigo R. Sarcoma de Kaposi associado à corticoterapia sistémica. Rev AMRIGS. 2010;54(2):202-5. [ Links ]
19. Jiménez E, Jiménez EE. Sarcoma de Kaposi en un adulto con transplante renal. Medisan. 2010;14(7):1000-4. [ Links ]
20. Bejar C, Ayaipoma A, Chián C. Casos clínicos, Sarcoma de Kaposi clásico. Folia Dermatol Perú. 2008;19 (1):27-31. [ Links ]
21. Hiatt KM, Nelson AM, Lichy JM, Fanburg JC. Classic Kaposi sarcoma in the United States over the last two decades: A clinicopathologic and molecular study of 438 non-HIV-related Kaposi sarcoma patients with comparison to HIV-related Kaposi sarcoma. Mod Pathol. 2008;21(5):572-582. [ Links ]
