










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.30 no.3 Bogotá July/Sept. 2015
Epigastric Pain related to Posture as a Possible Symptom of Gastritis due to Cytomegalovirus in a Renal Transplant Patient: A Case Report
Mónica Zuluaga Quintero MD. (2), Arbey Aristizábal Alzate MD. (1), John Fredy Nieto-Ríos MD. (1), Catalina Ocampo Kohn MD. (1), Lina María Serna-Higuita MD. (1), Juan Camilo Pérez Cadavid MD. (3), Gustavo Adolfo Zuluaga Valencia MD. (1)
(1) Nephrologist at the Hospital Pablo Tobon Uribe and the Universidad de Antioquia in Medellín, Colombia.
(2) Internal Medicine Resident at the Universidad Pontificia Bolivariana in Medellín, Colombia.
(3) Pathologist at the Hospital Pablo Tobón Uribe in Medellín, Colombia.
Received: 12-02-15 Accepted: 21-07-15
Abstract
Cytomegalovirus is an entity which causes significant morbidity and mortality among solid organ transplant patients. It may occur as a primary infection or be reactivated. In either case clinical manifestations vary. We report the case of a patient with severe epigastric pain related to posture which was the primary symptom of a cytomegalovirus infection.
Keywords
Cytomegalovirus, renal transplantation, gastritis, epigastric pain.
INTRODUCTION
Cytomegalovirus (CMV) infections are important complications in solid organ transplant patients, with high morbidity and mortality rates associated with the cytopathic effects of the virus and effects on the immune system (1).
CMV infections are diagnosed when there are signs or symptoms associated with the virus with evidence of tissue invasion and the virus is isolated using one or another technique (2). An infection is classified as either primary or as a reactivation. Primary infections are those that occur in patients who were previously seronegative. Reactivations are those infections that develop in patients who carry the virus or had previously been treated for the infection. Clinical manifestations vary. They include fever, fatigue, loss of appetite, abdominal pain, diarrhea, vomiting and headache. Tests may show leucopenia, thrombocytopenia, hyponatremia and evidence of visceral involvement. Physicians and care-givers must have a high index of suspicion for this entity in the post-transplant period during which the gastrointestinal compromises occur frequently (1, 2). The British transplant society has noticed that postural epigastric pain is a clinical manifestation of the disease that is useful for diagnosis of CMV infections (3). The pain is attributed to CMV induced gastritis. This article presents the case of a man who had been suffering from CMV for five months following a transplant whose principal symptom was postural epigastric pain.
CLINICAL CASE
The patient was a 64 year old man with a history of hypertension, diabetes mellitus, obesity, dyslipidemia, and chronic renal disease that had been managed with hemodialysis. He received a transplant of cadaveric kidney in March 2014, received basiliximab induction therapy plus IV methylprednisolone with immunosuppressant maintenance treatment with tacrolimus (target levels of 4 to 7 ng/ml), mycophenolate mofetil equivalent to 720 mg MPA, and 10 mg/day prednisone. Blood tests for CMV IgG were negative, but blood tests for CMV IgG of the donor were positive.
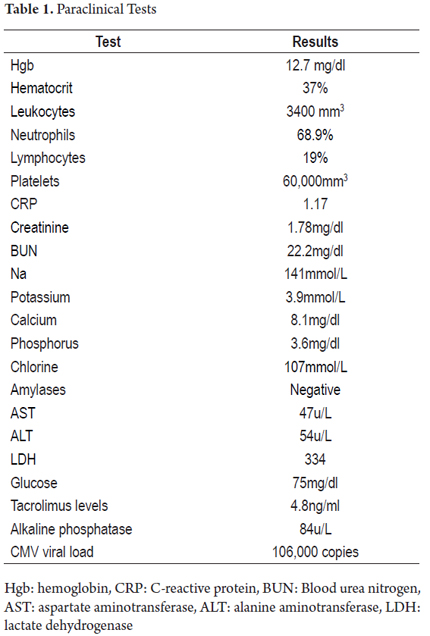
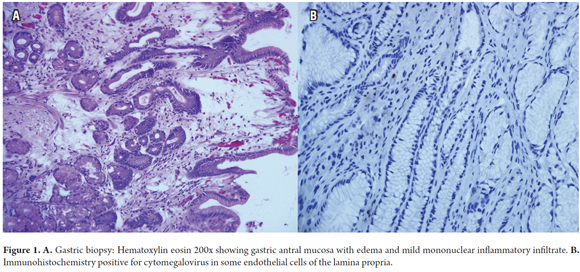
The patient was treated with valganciclovir for 100 days. Five and a half months after transplantation the patient developed intense burning and stabbing pain in the epigastric area which worsened when standing and walking and improved in a supine position. Physical examination showed tenderness of the epigastrium but no signs of peritoneal irritation. Multiple differential diagnoses had to be discarded. At the beginning we thought the patient might have suffered an acute coronary event, but the pain was not typical of angina, there was no compromise of oxygen saturation, and an electrocardiogram and biomarkers were negative. Echocardiography showed no abnormalities of the myocardium or pericardium. Abdominal ultrasound showed that the patient's gallbladder and liver were normal sized. The patient tested negative for hepatitis B and C negative. An enzyme profile including amylase, lipase and lactic dehydrogenase was performed. Pancreatitis, cholecystitis and hepatitis were ruled out. An x-ray showed no signs to suggest pain related to pneumonia, to the mediastinum, or to the large blood vessels. Attention focused on the patient's high levels of transaminases and the presence of leukopenia, thrombocytopenia, and renal dysfunction (see Table 1). These were associated with the timing of the abdominal pain following transplantation and the CMV serology of the donor. An opportunistic infection was suspected. The patient tested positive for CMV with a viral load of 106,900 copies/ml. Upper gastrointestinal endoscopy showed antral erosive gastritis, and pathology of the biopsy sample showed acute inflammation of the mucosa with immunohistochemistry positive for CMV (see Figure 1). Treatment was initiated with IV ganciclovir, adjusted to the patient's weight and kidney function. Symptoms improved within a week of initiation. Treatment was completed in 21 days with resolution of symptoms.
DISCUSSION
CMV infection is the most common cause of infection following kidney transplantation. Although the usual time of appearance is within the first 6 months following transplantation when the maximum cumulative dose of immunosuppression is received, CMV infections can occur at any time (1). It manifests in three ways: primary infections, reactivated infections, and superinfections. Primary infections occur in patients who have had no previous contact with the virus. Reactivation occurs when a patient has had no previous contact with the virus and becomes infected from a seropositive donor or from blood transfusions. Reactivation occurs when a patient who is CMV seropositive undergoes transplantation and the infection is reactivated as the effect of immunosuppression. Superinfections are those instances in which a seropositive recipient acquires a different strain from a CMV positive donor. The importance of suspicion and early recognition lies in their direct relations to increased morbidity and mortality (2, 3).
Because the clinical picture of CMV is nonspecific and variable, CMV can be confused with multiple clinical conditions. This makes the initial diagnosis difficult. Usually, its onset is insidious. Fever lasting for three to four weeks is a classic symptom. This is especially true when it occurs together with systemic manifestations such as fatigue, weakness, muscle pain and arthralgia (3). Nevertheless, there are no typical findings that will cause suspicion. A common laboratory finding is cytopenia which occurs in 50% to 60% of cases. It can cause anemia, thrombocytopenia, and leucopenia or a combination of any of these. Multiorgan disease with compromises of the liver, gastrointestinal tract, respiratory system, kidney, and/or brain can occur and is seen in up to 30% of cases. Still, a more common sign is graft dysfunction either alone or in conjunction with other signs. There is a large incidence of acute rejection in cases of this opportunistic infection (1). Gastrointestinal manifestations remain the most common signs. Any part of the gastrointestinal tract can be affected, and symptoms can include epigastric pain, nausea, vomiting, diarrhea, ulcers, gastrointestinal bleeding and perforation (2, 4). Characteristic endoscopic findings include diffuse erythema, erosion, nodules, plaques and ulcers. These findings should raise suspicion and be followed up with blood tests and histology to determine cytopathic changes and to check for CMV viral loads which remains the gold standard for diagnosis of this disease (2, 5, 6).
The difficulty of diagnosis requires strategies based on timely suspicion of CMV. The most important is to categorize risk as high or low and, on the basis of clinical studies, request laboratory studies for confirmation. When both the donor and the recipient are seronegative for CMV, it is considered to be a low risk situation. High-risk situations include when the organ donor has tested positive for CMV while the recipient has tested negative especially when other factors come into play such as the type of immunosuppression, transplant time, contacts, comorbidities and the type of antiviral prophylaxis used (1). If these conditions are present and there is clinical suspicion, blood tests should be performed to determine whether there is a primary infection, and a biopsy of the lesions should be cultured. Viral load should be monitored to determine response to treatment whether or not there is diagnostic probability of another disease since this opportunistic infection is easy to confuse with other pathologies and because early antiviral treatment has high success rates and direct effects on patient and graft survival (2).
Our patient's description of epigastric pain that increased when standing or walking, and improved in a supine position drew our attention. We considered that this was not a unique manifestation of one entity and that it therefore required ruling out all the possibilities mentioned above. Finally, we diagnosed gastrointestinal compromise due to a CMV infection. Appropriate treatment was administered which led to improvement of symptoms. Based on this, we subsequently found descriptions of postural epigastric pain as a manifestation of CMV gastritis. To date, seven cases in solid organ transplant patients have been reported in the literature. Six of these patients had kidney transplants and either primary or reactivated CMV infections. All were confirmed with endoscopy and histology, and the symptoms of all patients were resolved by the completion of treatment.
Giladi et al. published a report of the first three cases. Three months after transplantation, these patients developed epigastric pain which increased while standing or walking and decreased while supine (5), All three had primary CMV infections, and all three had complete resolution of pain and other symptoms following antiviral therapy. Also in 2006, P. Moustafellos et al. described the case of a woman with a primary CMV infection who developed epigastric pain 6 weeks after transplantation (6), Her pain appeared when she began to sit or walk and subsided with bed rest. Her symptoms resolved in the second week of treatment with ganciclovir. Three years later, Li W et al. described as similar situation that developed in a young man with CMV infection four months after transplantation (7). His symptoms had developed the week before he came to the physician and resolved within two weeks of starting treatment with ganciclovir. In this case, both donor and recipient were CMV seropositive suggesting that these symptoms are not exclusively signs of primary infections. Tapan et al. recently published a report in which a 36-year-old man presented postural epigastric pain. Suspicion of CMV gastritis was confirmed by biopsy (8). We published the case of a man who presented postural epigastric pain as the first symptom of this pathology following a kidney transplant. Other diseases may present with epigastric pain, but the exacerbation of symptoms related to standing and walking as the main feature has not been described as the main feature of any of them. In fact, pain even becomes worse in supine positions in some of them. In the few cases that have been documented to date, this symptom has been found during the active phase of gastrointestinal CMV infections and has resolved with antiviral treatment. On this basis, we suggest that postural epigastric pain can be a unique manifestation of CMV infections in renal transplant recipients even though only a few cases have been described and a universal conclusion cannot yet be reached. Most often, patients cannot spontaneously describe these symptoms and must therefore be questioned specifically about symptoms suggesting a diagnosis of CMV gastritis. This suspicion should always be confirmed by serological studies, endoscopy and biopsies.
CONCLUSION
Intense postural epigastric pain is a clinical symptom that may suggest gastric compromise due to CMV infections in patients following solid organ transplants. These infections are not exclusively primary. This entity should be suspected and either confirmed or ruled out whenever this symptom develops since it may be the only initial manifestation. This is especially important since the differential diagnosis is so broad and complex that performance of all necessary studies to rule out other conditions may place the integrity of the patient at risk.
REFERENCES
1. De la Torre J, Farinas M, Castón J, Aguado J, Cantisá S, Carratalá J, et al. GESITRA-SEIMC/REIPI recommendations for the management of cytomegalovirus infection in solid-organ transplant patients. Enferm Infecc Microbiol Clin. 2011;29(10):735-58. [ Links ]
2. Kotton C, Kumar D, Caliendo A, Åsberg A, Chou S, Snydman D. International Consensus Guidelines on the management of cytomegalovirus in solid organ transplantation. Transplantation. 2010;89(7):779-95. [ Links ]
3. Guidelines for the prevention and management of cytomegalovirus disease after solid organs transplantation. 3rd edition. British Transplantation Society; 2011. [ Links ]
4. Linares L, Sanclemente G, Cervera C, et al. Influence of cytomegalovirus disease in outcome of solid organ transplantpatients. Transplant Proc. 2011;43(6):2145-8. [ Links ]
5. Giladi M, Lembo A, Johnson B Jr. Postural epigastric pain: A unique symptom of primary cytomegalovirus gastritis? Infection. 1998;26:234-5. [ Links ]
6. Moustafellos P, Hadjianastasiou V, Gray D. Postural epigastric pain as a sign of CMV gastritis: A case report. Transplant Proc. 2006;38(5):1357-8. [ Links ]
7. Li W, Fan H, Yiping L. Postural epigastric pain as a sign of cytomegalovirus gastritis in renal transplant recipients: A case based review. Transplant Proc. 2009;41(9):3956-8. [ Links ]
8. Tapan U, Kutlugun AA, Arici M, Altun B. Postural epigastric pain: A challenging symptom for cytomegalovirus (CMV) gastritis. Ren Fail. 2012;34(2):235-6. [ Links ]
