










Serviços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista colombiana de Gastroenterología
versão impressa ISSN 0120-9957
Rev Col Gastroenterol vol.31 no.1 Bogotá jan./mar. 2016
Findings from anorectal endosonography in a prospective cohort
Edgar Julián Ferreira B. MD. (1), Lázaro Antonio Arango M. MD. (2), Edelberto Mulett V. MD. (3), Mauricio Osorio Ch. MD. (3), Dínimo José Bolívar S, MD. (1)
(1) Clinical and Surgical Gastroenterology Fellow, Universidad de Caldas. Manizales, Colombia.
(2) Clinical and Surgical Gastroenterology Program Coordinator, Universidad de Caldas. Clinical and Surgical Gastroenterology Professor, Universidad de Caldas. Manizales, Colombia.
(3) Clinical and Surgical Gastroenterology Professor, Universidad de Caldas. Manizales, Colombia.
Received: 02-12-15 Accepted: 26-01-16
Abstract
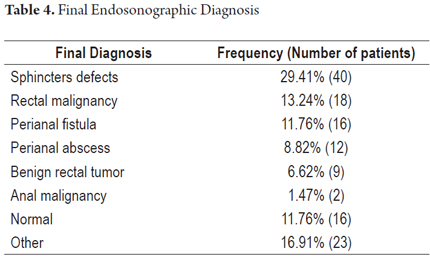
Anorectal endosonography can diagnose many diseases of the anal canal and rectum. In Colombia, the procedure is performed in only a few medical centers because of the scarcity of trained personnel. Four years ago, a group of teachers from the gastroenterological surgery clinical at the University of Caldas received training in endoluminal ultrasonography in Chile and Spain and have been practicing these procedures ever since. This is a descriptive study of a prospective cohort using data from patients who underwent endoluminal ultrasonography between October 2014 and September 2015. Data were obtained from 136 patients, of whom 72.05% were women. 20.6% of the patients came from departments other than Caldas. Fecal incontinence was the reason for the procedure for 44 patients (32.35%, 86% of whom were women). Other indications were rectal malignancies (23.5%), perianal fistulas (12.5%), anal pain (11.03%), endometriosis (7.35%), and perianal abscesses (6.62%). The most common final diagnoses were defective sphincters in 40 patients (29.41%), rectal malignancy in 13.24% of the patients, perianal fistulas in 11.76% of the patients, perianal abscesses in 8.82% of the patients, and benign rectal neoplasms in 6.62% of the patients . The results are consistent with those found in the international literature where the most common final diagnoses reported for the reason for fecal incontinence are sphincter defects and obstetric disorders.
Anorectal endosonography is of great importance when used alone or to support other diagnostic tools. It is recommended that this procedure be done in a referral center such as ours which performs a large volume of these procedures and which follows international guidelines.
Keywords
Endosonography, anal canal, rectum, fecal incontinence.
INTRODUCTION
Endosonography began to be used in the gastrointestinal tract in 1993, but the most rapid advances in the anorectal area have been made within the last decade. Now, equally good, and sometimes better, results than other diagnostic studies can be achieved. (1) In Chile, one of the largest studies of this technique yet performed, looked at 1,000 cases of patients who underwent anorectal endosonography has been published. It describes the main reasons for endosonography and final endosonographic diagnoses. (4)
Nevertheless, in Colombia there have been few studies of the use of endosonography in the gastrointestinal tract, and there is generally very little information from the referral centers where the procedure is performed. (2, 3)
Currently, the examination is most frequently done to study fecal incontinence, perianal fistulas, and perianal abscesses and for staging and monitoring of anal and rectal cancer and rectal pain. (4)
The diagnostic performance of anorectal endosonography varies depending on the reason for the examination. It has a sensitivity of 87% for perianal fistulas and between 82% and 95% for tumors but is less sensitive for other indications. (5, 6, 7)
A group of teachers of clinical and surgical gastroenterology at the University of Caldas received training in performance of anorectal endosonography in Chile and later in Spain. Four years later, the results of that training have been excellent.
This study was conducted in order to increase awareness of experience using anorectal endosonography. It describes findings from anorectal endosonography in a prospective cohort of adult patients cared for together with surgeons in Manizales between October 2014 and September 2015.
MATERIALS AND METHODS
This is a descriptive study of adult male and female patients who underwent anorectal endosonography for any reasons in the Department of Surgical and Clinical Gastroenterology of the Clínica La Presentación of the Union of Surgeons at the University of Caldas between October 2014 and September 2015. Patients were only excluded when all data could not be collected.
A data collection form was designed for this study which included the patients name, age, sex, occupation, place of birth, duration of any current disease related to the reason for undergoing the procedure, womens gynecological histories, history of births including tearing, reason for procedure, final findings and endosonographic diagnosis and measurements of anatomical structures in the anal canal.
Technical Procedure
Standard radial endosonography was used with endoscopic and endosonographic vision for all examinations by the same team in all cases. Frequencies between 5 and 15 MHz were used as needed. A high resolution processor unit was used. Patients were evaluated in left lateral decubitus position. Detailed perianal inspection, digital rectal examination and endoscopic evaluation until the upper rectum was performed. The endosonographic assessment located anatomical structures to be used as guides. The uterus, or bladder when the uterus was absent, was used for women, and the prostate gland, male urethra when the prostate was absent, was used for men. In addition, the pubic-rectal muscle was located for both men and women. The left was located at 3 oclock and the right at 9 oclock. In cases in which masses were evaluated, water was used as the acoustic medium.
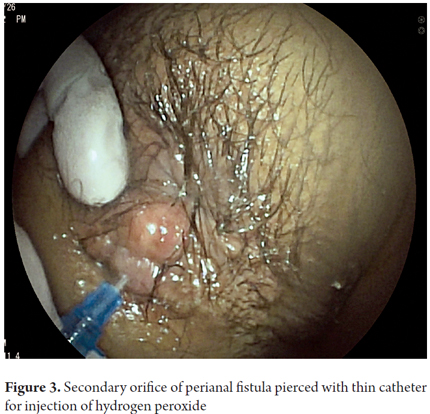
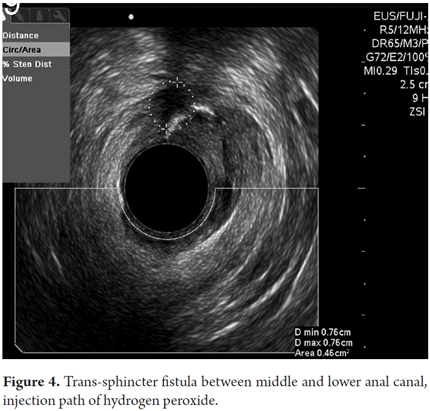
For perianal fistulas, a secondary perianal orifice was cannulated with the blunt portion of a 18 or 20G catheter, hydrogen peroxide was injected to produce contrast along the length of the fistula to make it completely visible endosonographically. The thickness of the sphincters were measured at 3 or 9 oclock, masses were measured, and tumors were staged according to the TNM system. For the measurement of the female perianal region, simultaneous vaginal examination was performed and the hyperechoic measurement was taken using a gloved finger inserted to the mucosa as the point of reference.
Data Analysis
Descriptive data are expressed as percentages, means and standard deviations.
RESULTS
Although 162 patients underwent anorectal endosonography, data from 26 patients was not available for various reasons, so one hundred thirty six patients were included in this study.
Demographics
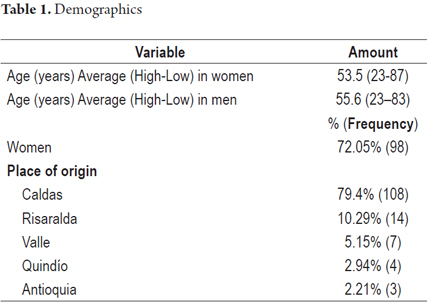
There was a predominance of female patients (72.05%, n = 98). The average ages of men and women were similar: 55.6 years for men with a standard deviation of 14.46 years, and 53.5 for women with a standard deviation of 14.98 years. Most patients (79.4%) came from the Department of Caldas, and the remainder came from Risaralda, Valle, Quindío and Antioquia (Table 1).
GYNECOLOGICAL HISTORIES
Of the 98 female patients, 34 reported histories of vaginal deliveries, and of these 30 reported history of tearing during at least one delivery (88.2%). The maximum number of reported births was 6, and the minimum was 1.
Reasons for examinations
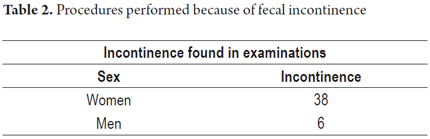
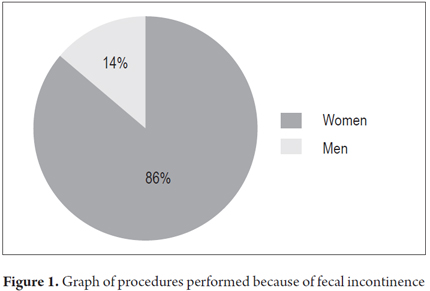
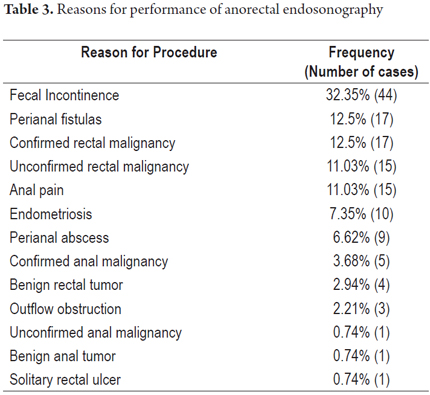
Forty-four patients (32.35%) underwent examination because of fecal incontinence. Thirty eight of these patients (86%) were women (Table 2 and Figure 1). Within this group, 28 (76.7%) of the 38 women also reported histories of obstetrical laceration. Examinations because of perianal fistula accounted 12.5% of all cases, while those for perianal abscess accounted for 6.62%. The entire list of reasons for the procedure is presented in Table 3.
Final Endosonographic Diagnosis
Sphincter defects were found in 40 patients (29.41%), of which 6 were men and 34 women. Here it should be noted that 93.33% (n = 28) of women who had histories of incontinence also had histories of tearing.
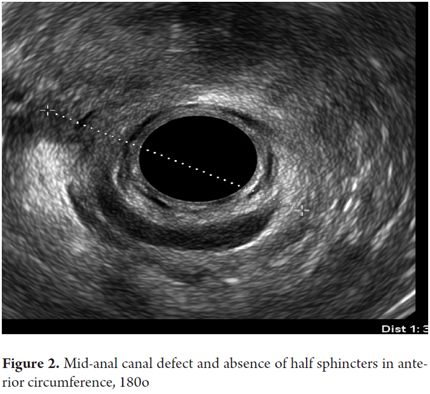
Of the 34 women with sphincter defects, 32 they were located in the anterior middle anal canal. One of these cases had diffuse atrophy of the sphincters and another had a compromised lower anal canal (Figure 2).
On the other hand, among men with fecal incontinence, all diagnoses showed atrophy of the sphincter apparatus that could be seen from all views of the anal canal. It was evident as general thickening of the muscles seen as diffuse changes of echogenicity. It was not possible to determine limits of areas affected by atrophy.
Perianal fistulas were found in 16 patients (11.8%). Of these 37.5% were trans-sphincter fistulas with fewer cases of inter-sphincter and anal-vaginal fistulas (Figures 3 and 4).
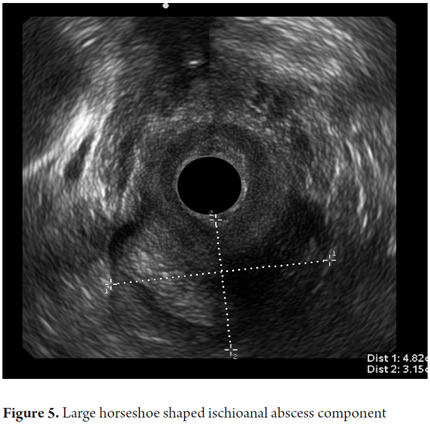
Twelve patients had perianal abscess (8.8%). Of these, 83% were ischiorectal or submucosal abscesses (Figure 5).
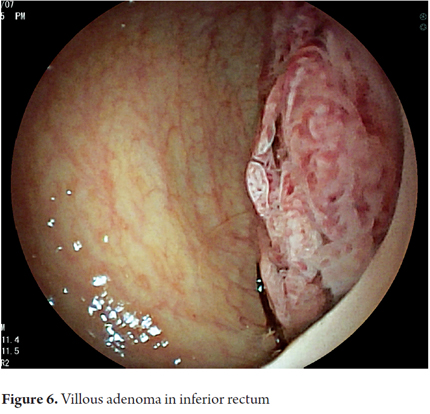
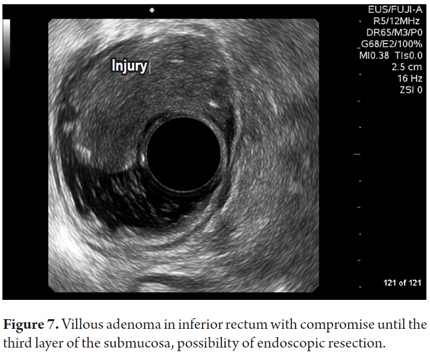
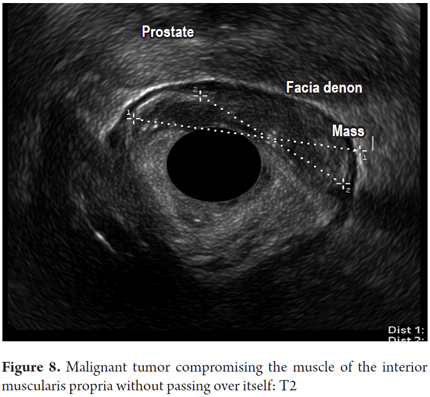
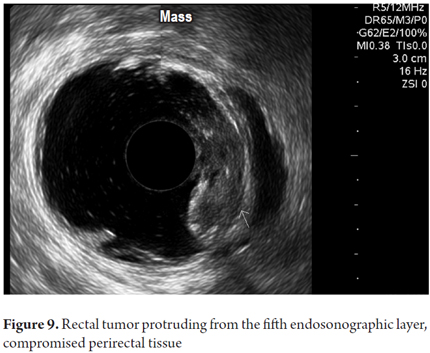
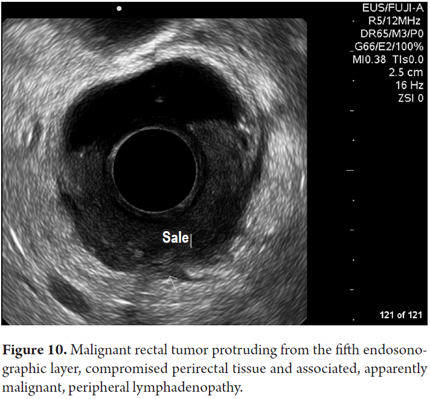
Other final diagnoses are presented in Table 4. It is noteworthy that endoscopic resections of lesions were possible and were performed for benign neoplasms of the rectum that had been scheduled for more invasive surgical procedures (Figure 6 and 7). Also worthy of note is the fact that it was determined that it was possible to recover the sphincters of three patients who were examined because of anal canal cancer that had been treated by oncologists. Two early diagnoses of malignant neoplasms of the rectum were made at TNM stages of less than T2 and N0 (Figure 8). In 88.8% of the cases, advanced lesions were found (Figures 9 and 10). Within the other category are, in order of frequency from highest to lowest, endometriosis, enteroceles, anal fissures, rectal varices and one case of sigmoid colon cancer.
Among patients whose results were normal, reasons for the procedure from most frequent to least frequent were anal pain (n = 5), unconfirmed rectal neoplasm (n = 2), endometriosis (n = 2), fecal incontinence (n = 2), unconfirmed anal neoplasia (n = 2), and one case each of perianal fistula, perianal abscess, solitary rectal ulcer and obstruction.
Sphincter Measurements
Pubic-rectal measurements were normal in 92.59% of patients (n = 125). The measurement of the internal anal sphincter in the upper anal canal was reported to be normal in all cases. In the middle anal canal, all internal anal sphincter measurements were normal while 97.78% of the measurements of the external anal sphincter in the middle of the anal canal were normal (n = 132). All measurements of the external anal sphincter at the lower end of the anal canal were normal. Perineal measurements were abnormal in 11.22% of women (11 of 98).
DISCUSSION
The most important reason endosonography was fecal incontinence which affected the majority of the women in the study and which is consistent with world literature. (12-16) Also consistent with world literature was the fact that women in this study who had fecal incontinence usually had suffered obstetrical tearing. The descriptive study by Lopez-Kostner et al. found that fecal incontinence was the main reason for anorectal endosonography: out of 1,000 cases, 336 patients (33.6%) underwent the procedure for this reason. (4) In our study it was even more: 44%, and these patients were also predominantly women (86%).
Perianal fistulas were the second most frequent reason for conducting this procedure which highlights its importance because it can accurately characterize the surgical anatomy for proper classification of the fistula. Various authors also use hydrogen peroxide for endosonographic contrast to provide details of fistulas. (4,8,17,18)
Similarly, there was a significant number of patients for whom malignant rectal tumors were confirmed. This is an indication of the growing acceptance here in Colombia and elsewhere of interdisciplinary teams including oncologist. Endosonography plays a key role in these teams as a complement to other diagnostic tools for regional staging and proper treatment planning. (4,9,19-22)
The study of anal pain, a complex pathophysiology misunderstood by all, and the high probability that imaging and traditional endosonography will not be able to find the cause, has made room for anorectal endosonography. (10)
Sphincter defects are the most common final diagnosis for the symptom of fecal incontinence: they go hand in hand in the majority of women with a history of obstetric lacerations. (10,11)
There is a large group of patients whose endosonography reports were normal who underwent the procedure for various reasons but especially for anal pain. Of those patients who underwent the procedure for anal pain, 33% had normal endosonography which is consistent with what is reported in the world literature. (23-26)
In most cases, sphincters measurements were normal but this is influenced the nine oclock and three oclock positions at which measurements were taken (lateral aspect of the sphincters). This is far less than the abnormalities found with endosonography for fecal incontinence, which is the most frequent reason. (24-27)
Perineal measurements were smaller than normal in a significant number of women who had incontinence as the main reason for the procedure.
This paper highlights the fact that anorectal endosonography is already being conducted following international standards here in Colombia in institutions like ours and the fact that the reasons for conducting the procedures are in line with international experience. It is also evident that there is a significant volume of work which makes the surgical group of clinical gastroenterology at the University of Caldas a referral center for this type of examination.
Although the great majority of patients come from our own department of Caldas, more than 20% are from other departments. This highlights the fact that this referral group receives patients from various parts of the country.
This in turn underlines the difficulties of accessing health care in our country and the often long distances patients must travel for diagnosis and treatment.
This simple study is a starting point to stimulate others to use this technology that is increasingly becoming important worldwide and is at the forefront of advances that are now being made and are about to be made. This study looks at the main reasons directions anorectal endosonography is performed which should allow health institutions to develop clinical practice guidelines that achieve enormous benefits for patients.
REFERENCES
1. Armengol JR, Benjamin S, Binmoeller K. Consensus Conference. Clinical applications of endoscopic ultrasonography in gastroenterology: state of the art. Endoscopy. 1993;25:358-66. [ Links ]
2. Gómez M, Otero W, Arbeláez V, Rodríguez J. Ecoendoscopia. Indicaciones de la A a la Z. Rev Col Gastroenterol. 2005;20(2):34-64. [ Links ]
3. De Nubbila E, Montes J, Spath A, Serrano S, Díaz-Yúñez I, Parra G. Endosonografía del esfínter rectal. Rev Colomb Radiol. 2007;18(4):2233-9. [ Links ]
4. López-Köstner F, Zárate A, García-Huidobro M, Pinedo G, Molina M, Krônberg O, et al. Indicaciones y resultados de la endosonografía anorrectal. Análisis de las primeras 1000 endosonografías. Rev Chil Cirug 2007;50(1):31-37. [ Links ]
5. Alós R, de la Portilla, F. La ecografía anorrectal en las neoplasias de recto. En: Principios Prácticos de Ecografía anal y Rectal. Madrid. 2004. Ed. Díaz de Santos. 81- 95. [ Links ]
6. Garcés M, García S, Esclápez P, Sanahuja A, Espí A, Flor B, et al. Evaluación de las fístulas perianales mediante ecografía endoanal tridimensional y correlación con los hallazgos intraoperatorios. Cir. Esp. 2010;87(5):299-305. [ Links ]
7. Stamatiadis A. Endoanal ultrasound in perianal abscesses. Dis Colon Rectum. 2002;45:710-11. [ Links ]
8. Glaser F, Schlag P, Herfarth C. Endorectal ultrasonography for the assessment of invasion of rectal tumours and lymph node involvement. Br J Surg. 1990;77:883-887. [ Links ]
9. Jordán J, Roig JV, García Armengol J, Esclápez P, Jordán Y, García Granero E, Alós R, Lledó S. Importancia de la exploración física y técnicas de imagen en la valoración diagnóstica de las fístulas de ano. Cir.Esp. 2009;85(4):238-245. [ Links ]
10. Alos R, Roig JV. Utilidad y limitaciones de la ecografía anorrectal. Rev Sdad Valenciana Patol Dig. 1999;18:56-67. [ Links ]
11. Saranovic D, Barisic G, Krivokapic A, Masulovic D, Djuric-Stefanovic A. Endoanal ultrasound evaluation of anorectal diseases and disorders: Technique, indications, results and limitations. Eur J Radiol. 2007;61:480-489. [ Links ]
12. Starck M, Bohe M, Valentin L. The extent of endosonographic anal sphincter defects after primary repair of obstetric sphincter tears increases over time and is related to anal incontinence. Ultrasound Obstet Gynecol. 2006;27(2):188–97. [ Links ]
13. Oberwalder M, Thaler K, Baig MK, Dinnewitzer A, Efron J, Weiss EG, Vernava Am 3rd, et al. Anal ultrasound and endosonographic measurement of perineal body thickness: A new evaluation for fecal incontinence in females. Surg Endosc. 2004;18(4): 650-4. [ Links ]
14. Starck M, Bohe M, Valentin L. Results of endosonographic imaging of the anal sphincter 2–7 days after primary repair of third- or fourth-degree obstetric sphincter tears. Ultrasound Obstet Gynecol. 2003;22:609–15. [ Links ]
15. Siddiqui MR , Ashrafian H, Tozer P, Daulatzai N, Burling D, Hart A, Athanasiou T, Phillips RK. A diagnostic accuracy meta-analysis of endoanal ultrasound and MRI for perianal fistula assessment. Dis Colon Rectum. 2012;55:576-85. [ Links ]
16. Hildebrandt U, Feifel G. Preoperative staging of rectal cancer by intrarectal ultrasound. Dis Colon Rectum. 1985;28:42-6. [ Links ]
17. Doornebosch PG, Bronkhorst PJ, Hop WC, Bode WA, Sing AK de Graaf EJ. The role of endorectal ultrasound in therapeutic decision-making for local versus. Transabdominal resection of rectal cancer. Dis Colon Rectum. 2008;51(1):38-42. [ Links ]
18. Garcia-Granero E, Faiz O, Flor B, Garcia S, Esclapez, P, Cervantes A. Prognostic implications of circunferential location of distal rectal cancer. Colorrectal Dis. 2011;13(6):650-7. [ Links ]
19. Giovannini M, Bardou VJ, Barclay R, Palazzo L, Roseau G, Helbert T, et al. Anal carcinoma: Prognostic value of endorectal ultrasound. Results of a prospective multicenter study. Endoscopy. 2001:33(3):231-6. [ Links ]
20. Parikh J, Shaw A, Grant LA, Schizas AM, Datta V, Williams AB, Griffin N. Anal carcinomas: The role of endoanal ultrasound and magnetic resonance imaging in staging, response evaluation and follow-up. Eur Radiol. 2011;21:776-85. [ Links ]
21. Martellucci J. Endoanal ultrasound for anal cancer follow up. Int J Colorectal Dis. 2011;26:679-80. [ Links ]
22. Beer-Gabel M, Carter D, Venturero M, Zmora O, Zbar AP. Ultrasonographic assessment of patients referred with chronic anal pain to a tertiary referral centre. Tech Coloproctol. 2010;14(2):107-12. [ Links ]
23. Naldini G, Cerullo G, Mascagni D, Orlandi S, Menconi C, Zeri K, Felli E, Martellucci J. Hiding intersphincteric and transphincteric sepsis in a novel pathological approach to chronic anal fissure. Surg Innov. 2012;19:33-6. [ Links ]
24. Stamatiadis A. Endoanal ultrasound in perianal abscesses. Dis Colon Rectum. 2002;45:710-1. [ Links ]
25. Millan M, García-Granero E, Esclápez P, Flor-Lorente B, Espí A, Lledó S. Management of intersphincteric abscesses. Colorectal Dis. 2006;8:777-80. [ Links ]
26. AG, Parks, PH Gordon, JD Hardcastle. A classification of fistula-in-ano. BR J Surg. 1976;63:1-12. [ Links ]
27. Cho Dong-Yoon. Endosonographic criteria for an internal opening of fistula-in ano. Dis Colon Rectum. 1999;42 (4):515-8. [ Links ]
