










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.31 no.1 Bogotá Jan./Mar. 2016
Two Case Reports of Spontaneous Transverse Colon Volvulus
Diego Severiche B. MD (1), Reinaldo Andrés Rincón S. MD (2), Andrés Montoya D. MD (2), Alejandro Concha M. MD (2), Diana Carolina Hennessey C. MD (3)
(1) Internist at the Universidad De la Sabana in Bogotá, Colombia.
(2) Gastroenterologist, Gastroenterology and Endoscopy Unit at Fundación Clínica Shaio in Bogotá, Colombia.
(3) Internist at Universidad El Bosque in Bogotá, Colombia.
Establishment where the study was done: Fundación Clínica Shaio
Received: 04-05-15 Accepted: 26-01-16
Abstract
Transverse colon volvulus is rare due to the anatomic location which impedes twisting. In the literature of the world, there have been fewer than 100 documented cases. This article presents two cases of transverse colon volvulus. They were suspected because of clinical evidence, images were obtained, colonoscopic reduction was performed and the disorders were confirmed intraoperatively.
Keywords
Volvulus, transverse colon, colonoscopy, intestinal obstruction, abdominal pain.
INTRODUCTION
The term volvulus is Latin for torque and is used to refer to twisting of the colon around an axis. It occurs most frequently in the sigmoid colon and can cause bowel obstruction with subsequent development of ischemia and necrosis and can result in perforation, peritonitis, sepsis and death. (1, 2)
Volvulus accounts for 10% to 15% of all cases of colonic obstruction and for 1% to 20% of all intestinal obstructions. (1) The sigmoid colon is the location of 43% to 80% of all cases of volvulus, 15% to 42% occur in the cecum, and only 2% to 4% occur in the transverse colon. (2, 3)
The two fundamental properties for the formation of volvulus are redundant colon and looseness of a colonic segment. The ascending and descending portions of the colon are fixed, but the sigmoid colon, the cecum and transverse colon are mobile within the peritoneum, attached only to the mesentery. (2)
We report two cases of spontaneous volvulus of the transverse colon: one man and one woman who both consulted because of pain and bloating.
Case 1
A 52 year old man came to the emergency room after four days of suffering severe abdominal pain and bloating without being able to defecate. He was initially treated simethicone and trimebutine but without improvement. The patient reported that epigastric pain radiated to the right iliac fossa and was associated with two episodes of vomiting of his stomach contents and abundant defecation of normal feces. According to the patient, he had been diagnosed with irritable bowel syndrome several years earlier.
Upon physical examination, the patient was alert but mildly dehydrated with a distended and tympanic abdomen. Auscultation showed decreased bowel sounds. Noticeable abdominal distension was widespread pain and tenderness was evident on palpation, but there were no clear signs of peritoneal irritation.
The blood count showed leukocytosis with neutrophilia. Tests of kidney functioning and urine tests were normal. A complete abdominal CT scan with contrast revealed thick distended bowel loops with twisting of the mesenteric vessels projecting into the right upper quadrant with a transition area in the ascending colon (Figures 1 and 2).


Volvulus was diagnosed, and we decided to perform endoscopic devolvulation. During the procedure an impassable volvulus was found at the splenic flexure but without any signs of ischemia. We decided to suspend the procedure and transfer the patient to the operating room for laparotomy. During the surgical procedure, an abnormally long large intestine with transverse colon volvulus was encountered. It was dilated an large areas were ischemic although there were no perforations. The ascending and descending colon was released. Then the transverse mesocolon was clamped, cut and ligated and the redundant piece was removed. A stapled side-to-side anastomosis was created. Postoperatively, the patients evolution was satisfactory, and he was discharged within a few days.
Case 2
An 80 year old woman came to the emergency room after five days of vomiting and generalized abdominal pain of moderate intensity that did not respond to analgesics and antispasmodics. The patient had a history of high blood pressure and chronic obstructive pulmonary disease (COPD), had a pacemaker because of third-degree atrioventricular (AV). She had undergone a cystopexy and a hysterectomy.
Physical examination showed that the patient was hypotensive, did not have a fever, but had widespread moderate to severe pain on palpation and a distended and tympanic abdomen with decreased bowel sounds on auscultation.
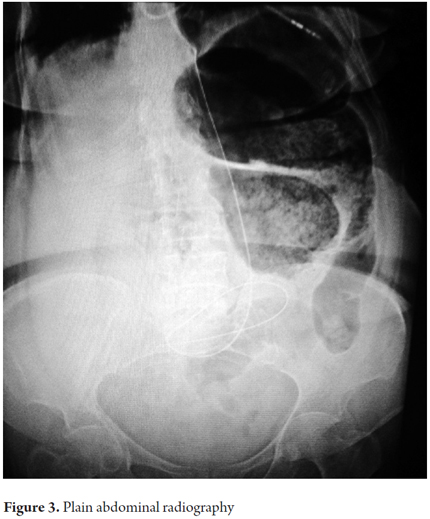
Her blood tests were normal. Her BUN was 89 and arterial gases showed severe metabolic acidosis (pH 7.31) with hyperlactatemia (11mg / dl). An abdominal x-ray showed distended colonic loops with air-fluid levels but no observable distal gas (Figure 3).
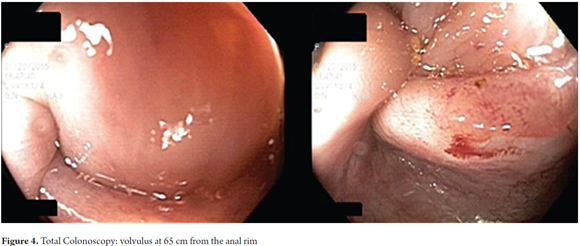
We diagnosed her with volvulus of the colon and decided to perform devolvulation through colonoscopy. We encountered a point of the volvulus in the descending colon which we were able to revert is achieved reverse and negotiate into an area marked colonic dilation. We encountered a second point of volvulus at 65 cm from the anal rim, but could not pass the colonoscope through it (Figure 4). We decided on urgent consultation with general surgery.
The patient underwent a laparotomy approximately eight hours after admission. During the surgical procedure we found fecal peritonitis secondary to perforation of the ascending colon and transverse colon volvulus. There was marked tissue friability due to hypoperfusion. A subtotal colectomy was performed which resulted in bleeding from the secondary layer of the splenic artery and a liver laceration. It required a laparostomy and packing. The patient was given blood transfusions, placed on vasopressor support, and transferred to intensive care after surgery. Twenty-four hours later, she underwent surgery again because of bleeding. She underwent peritoneal lavage and repacking. The patient died 36 hours after surgery.
DISCUSSION
A volvulus is an axial twisting or rotation of a portion of the colon around a portion of mesentery. It can be primary or secondary. (4) Globally, volvulus of the colon is the third leading cause of intestinal obstruction and bowel dilation. (2) Transverse colon volvuli account for only 3% of volvuli. (5)
In 1932, a Finnish surgeon named Kallio described the first case of transverse volvulus. (5, 6) In 1981, Anderson reviewed 66 patients who had been reported in the literature, and in 1994 Medina et al. documented a total of 72 cases. (6)
Transverse colon volvuli have two peaks of occurrence: in the second or third decade of life (slightly more frequently among women than among men), and among elderly patients with abundant comorbidities, especially among elderly men. (2) There are anatomical, physiological and mechanical factors that predispose to development of volvulus. The most common anatomical factors are abnormal attachment to the mesentery and abnormal rotation of the midgut. (7) Physiological factors include distal impediments to defecation such as chronic constipation, elongated ion and redundant colons and narrow points of attachment to the mesentery. (2, 6) The most common mechanical factor is obstruction of the sigmoid colon that may be secondary to neoplasia or consequences of diverticulitis. This can also trigger sigmoid colon volvulus. (6)
There are two clinical presentations of transverse colon volvuli that have been described: acute fulminant and subacute progressive. Acute volvulus is characterized by nausea, vomiting, marked leukocytosis, acute abdominal pain, signs of peritoneal irritation and sometimes bloating. The subacute presentation is accompanied by less nausea and vomiting, mild abdominal pain, abdominal distention without significant peritonitis, and normal or slightly elevated leukocyte counts. (8)
Diagnoses are not normally made prior to surgery since the radiographic findings are nonspecific unlike the typical coffee bean image of sigmoid colon volvulus. (4, 8) Some authors mention that a distended colon with two air-fluid levels in the epigastric region or the presence of a handle shaped U in the left upper quadrant in abdominal radiography may suggest the diagnosis, but this is not consistent. (5, 11, 12) As for CT scans, a review by Vandendries et al. reports no typical radiological characteristics for transverse colon volvulus. (9)
Management of volvuli is controversial for patients with viable colons who have no clinical evidence of peritonitis. There is general agreement on the use of colonoscopic decompression as the initial treatment of colon volvulus, independent of the segment compromised and with or without insertion of a rectal probe. Colonoscopy, besides being a therapeutic measure, allows the physician to assess the status of the colonic mucosa and check whether or not there is any necrosis or signs of ischemia. It has been shown to be effective in over 70% of patients. In case of failure of endoscopic decompression, which usually happens in most cases of volvulus of the cecum and transverse colon, priority surgery is necessary. (5, 6, 13)
Surgical management may include open or laparoscopic untwisting, with or without colopexy. However, given the high rate of recurrence a right extended hemicolectomy or colectomy of the transverse colon is recommended. (2) It is important to mention that in a work published by Ballantyne et al., all patients with volvulus of the transverse colon who only underwent untwisting and fixation without intestinal resection, died. (10)
CONCLUSION
Volvulus of the transverse colon is a rare entity which is difficult to identify radiologically, and preoperative diagnosis is difficult to make with certainty. For this reason, we must have high clinical suspicion in order to get a proper diagnosis and to provide timely management. For most of these patients, this means urgent surgery. Contrary to treatment of volvulus of the sigmoid colon, there is insufficient evidence to recommend use or avoidance of colonoscopy. However, its use should be limited to differential diagnosis given that its capacity to resolve the disorder is minimal and recurrences occur frequently.
REFERENCES
1. Sana L, Ali G, Kallel H, Amine B, Ahmed S, Ali EM, et al. Spontaneous transverse colon volvulus. Pan Afr Med J. 2013 Jan;14:160. [ Links ]
2. Gingold D, Murrell Z. Management of Colonic Volvulus. Clin Colon Rectal Surg. 2012;25:236–244. [ Links ]
3. Valsdottir E, Marks JH. Volvulus: Small Bowel and Colon. Clin Colon Rectal Surg. 2008 May;21(2):91-3. [ Links ]
4. Deshmukh SN, Maske AN, Deshpande AP, Shende SP. Transverse colon volvulus with chilaiditis syndrome. Indian J Surg. 2010 Aug;347–9. [ Links ]
5. Walczak DA, Czerwińska M, Fałek W, Trzeciak PW. Volvulus of transverse colon as a rare cause of obstruction – a case report and literature review. Pol Przegl Chir. 2013;605-7. [ Links ]
6. Ramírez-Wiella-Schwuchow G, Villanueva SE, Bolaños BL, García H. Volvulus de colon transverso: reporte de caso. Rev Gastroenterol Mex. 2009;74:35-8. [ Links ]
7. Robin KM Volvulus of the transverse colon. Trop Gastroenterol. 2012;33(3):229–231 [ Links ]
8. Sparks DA, Dawood MY, Chase DM, Thomas DJ. Ischemic volvulus of the transverse colon: A case report and review of literature. Cases J. 2008;1:174. [ Links ]
9. Vandendries C, Jullès MC, Boulay-Coletta I, Loriau J, Zins M. Diagnosis of colonic volvulus: Findings on multidetector CT with three-dimensional reconstructions. Brit J Radiol. 2010;83:983–990. [ Links ]
10. Ballantyne GH, Brandner MD, Beart RWJr, Ilstrup DM. Volvulus of the colon. Incidence and mortality. Ann Surg. 1985;202(1):83–92. [ Links ]
11. Mortensen MJ, Hoffman G. Volvulus of the transverse colon. Postgraduate Med J. 1979;(55), 54-57 [ Links ]
12. Newton NE, Reines HD. Transverse Colon Volvulus. Am J Roentgenol. 1977;128:69-72. [ Links ]
13. Mulas C, Bruna M. Management of colonic volvulus. Experience in 75 patients. Rev Esp Enferm Dig. 2010;102 (4):239-248. [ Links ]
