










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957
Rev Col Gastroenterol vol.31 no.2 Bogotá abr./jun. 2016
Endoscopic and Pathological Findings in Patients with HIV and Digestive Symptoms at a University Hospital
Luis Daniel Laguado V. MD (1), Reynaldo Mauricio Rodríguez Amaya MD (2), Jaime Gómez C. MD (3), Rómulo Arturo Bonilla G. MD (4), Gonzalo Rojas H. MD (4)
(1) Physician and Third-year Internal Medicine resident at the Universidad Industrial de Santander and member of the GERMINA research group in Bucaramanga, Colombia.
(2) Physician, MSc in Epidemiology, Professor in the Department of Internal Medicine and member of the GERMINA research group at the Universidad Industrial de Santander in Bucaramanga, Colombia. Mail: reynaldo.rodriguez@gmail.com
(3) Gastroenterologist in the Gastroenterology Unit at the Hospital Universitario de Santander, Professor and member of the GERMINA research group at the Universidad Industrial de Santander in Bucaramanga, Colombia.
(4) Gastroenterologist in the Gastroenterology Unit at the Hospital Universitario de Santander in Bucaramanga, Colombia.
Received: 17-11-15 Accepted: 18-04-16
Abstract
Introduction: Although the gastrointestinal tract is frequently affected by HIV, in clinical practice abnormalities related to HIV often appear to be normal when seen through an endoscope. The consequence is that these patients do not receive timely treatment for gastrointestinal diseases.
Methods: This is an observational study of HIV patients who came to the hospital of the Universidad Industrial de Santander because of digestive symptoms that required either endoscopy or colonoscopy, or both, during 2014. Socio-demographic, clinical and laboratory data were collected. A total of 41 upper endoscopies and 29 colonoscopies were performed in 54 patients. Biopsies were taken and analyzed in all cases.
Results: The mean patient age was 39 years old, the most frequent digestive symptoms were diarrhea and oral lesions, 87% of these patients had CD4 counts below 200, and only 24% currently receive HAART. The most frequent diagnoses were: esophageal candidiasis (17%), moderate chronic gastritis in the stomach (26.7%), and moderate chronic nonspecific colitis in the left colon (44.8%) and in the right colon (51.7%).
Conclusions: Endoscopic and pathological findings are consistent with the frequencies of presentations of gastrointestinal pathologies reported in the literature except that no tumors or infectious agents such as mycobacteria were found. The most common opportunistic infections were Candida and Cytomegalovirus. Diagnostic agreement between the endoscopist and pathologist varied. There was had only fair agreement for the esophagus, but there were large disparities for the stomach and colon. Consequently, when HIV/AIDS patients require endoscopy, it is important that the protocol call for biopsy samples and analysis.
Keywords
Digestive System, endoscopy, HIV infections, HIV enteropathy.
INTRODUCTION
According to the Joint United Nations Program on HIV/AIDS (UNAIDS), worldwide there are currently 35 million people living with HIV. Given the consequences and implications, this is considered to be a real public health problem. It is also estimated that 0.8% of adults aged between 15 and 49 are HIV-positive. (1) In 2013, 45,543 people in Colombia had HIV. The prevalence of the disease in the general population was 0.11%, but the prevalence in the population aged 15 to 49 years was 0.16%. (2) Clinical manifestations of HIV affect multiple organs and systems but vary in severity. They may be due to replication of HIV in infected tissue, to opportunistic infections, or to adverse drug effects. (3) The gastrointestinal tract is a site that is very frequently affected by HIV infection: up to 88% of HIV patients are reported to have had at least one abnormality in gastrointestinal functioning. (4) It has also been reported that the most frequent reasons for suspension of highly active antiretroviral therapy (HAART) are gastrointestinal manifestations which underscores the important role of endoscopy in the post-HAART era. (5)
Endoscopy is an invasive diagnostic test that helps clarify the etiology of most gastrointestinal diseases associated with HIV infection. Nevertheless, at times it is difficult to find a specific etiologic agent. This is partly explained by the virus's affinity for gastrointestinal tissues, and its generation of a pronounced loss of CD4 cells in the lamina propria of the intestinal mucosa. (6, 7) A review of the available literature shows that there are few studies in Latin America and in the world which offer information on endoscopic and histopathological reports for HIV patients. Usually, available studies provide information on very specific conditions. (8, 9) Therefore, this study aims at illustrating endoscopic and pathological clinical findings from a series of HIV patients whose chief complaints were digestive symptoms.
METHODS
Design and study population
This study was conducted in the Gastroenterology Unit of the University Hospital of Santander in Bucaramanga, Colombia. It is an observational and descriptive study of a number of patients admitted to the Hospital from January 1 to December 31, 2014. This hospital is a referral center for the public health care network in the northeastern region of Colombia. The study's inclusion criteria stated that patients had to be older than 18 years of age, to have an HIV diagnosis confirmed by Western Blot, to have been admitted to the hospital, and to have had digestive symptoms as their chief complaint. Similarly, patients had to have had clinical indications from the gastroenterology unit of the hospital for performance of upper digestive endoscopy or colonoscopy. Among the exclusion criteria were hemodynamic instability, psychomotor agitation, and neurological disorders that would have prevented performance of endoscopic studies or provision of informed consent.
Data collection
Once a patient met the inclusion criteria, we filled out a questionnaire with sociodemographic, clinical and paraclinical information. Clinical variables included information on gastrointestinal symptoms and on prior treatment received for HIV. Paraclinical variables included parameters such as complete blood count and CD4 cell count. Endoscopic findings and reports of any abnormal endoscopic diagnosis observed by gastroenterologists were also included. Finally, the diagnosis from the pathology laboratory of the Faculty of Health of the Industrial University of Santander (UIS) was recorded.
Endoscopic procedure
Preparation for diagnostic colonoscopy includes three oral colon cleansing doses, one rectal enema (sodium phosphate), a liquid diet the day before, and no oral intake the day of the exam. Preparation for upper endoscopy, includes fasting the night before (12 hours) and no oral intake on the day of the exam.
The following endoscopy and colonoscopy equipment was used:
Olympus CV-180 CLV-180 Evis Exera II Endoscopy System; OLYMPUS CV-160 & CLV-160 Evis Exera Video Endoscopy System; Olympus EVIS EXERA II GIF Type H180 endoscope; Olympus EVIS EXERA II CF-H180AL/I colonovideoscope Olympus GIF Type Q150/EVIS CF Type Q145L endoscope; Olympus EVIS CF-Q145L Video Colonoscope; All endoscopic procedures were performed in the gastroenterology service by one of the three gastroenterologists in the service. They performed endoscopic studies and prepared all reports in a standardized way.
Upper endoscopy explored from the esophagus to the second portion of the duodenum. The Kodsi scale was used to grade esophageal candidiasis, and the Los Angeles scale was used to grade esophagitis. (10, 11) Endoscopic characteristics were described and diagnoses were made for other abnormal findings. When a lesion was found, biopsies were taken at the discretion of the endoscopist (minimum four), if there were no macroscopic lesions and endoscopic examination was normal according to the protocol, two biopsy samples were taken from the distal esophagus and two more were taken from the stomach. Colonoscopy studied from the anal canal to the cecum. Ulcerative colitis was graded according to the Montreal classification, (12) endoscopic diagnoses were determined, and at least four biopsies were taken from lesions. When macroscopic findings were normal, the protocol called for four biopsies, two from the right colon and two from the left colon.
Processing and reading of biopsies
Biopsies were fixed in a wide mouth jar with 10% neutral buffered formalin, within the minimum proportion of 10:1 (formalin /sample). They were labeled and sent to the pathology laboratory for hematoxylin-eosin, Zieln Neelsen, Periodic Acid Schiff (PAS), Silver Methenamine and Giemsa staining. For this purpose, a stamp to identify samples from this study in the pathology service was developed. These samples were tested according to the protocol of the pathology department of the UIS with three observers and complementary studies as needed.
Measurement and Analysis of variables
Upon hospital admission, all patients in the study had an automated blood count taken. The sample was analyzed by a SYSMEX XN-1000 system. Hemoglobin anemia was defined as less than 12 g/dL in women and less than 13 g/dL in men, leucopenia was defined as less than 4000 leukocytes per mm3, and thrombocytopenia was defined as less than 150,000 platelets per mm3. Finally, the Beckman Coulter FC 500 flow cytometry system was used to measure CD4 lymphocytes to determine patients' immune statuses.
Statistical analysis
According to distribution, quantitative variables were analyzed by averages with standard deviations (SD) or by medians. Qualitative variables are presented as proportions with their respective confidence intervals.
ETHICAL CONSIDERATIONS
This study meets the guidelines of the Declaration of Helsinki and Colombian law (Resolution 8430 of 1993) with respect to health research. In addition, informed consent was obtain for the use of clinical information and laboratory tests of patients included in this study. Similarly, this study was approved by the University Hospital of Santander and the Ethics Committee of the Industrial University of Santander.
RESULTS
General
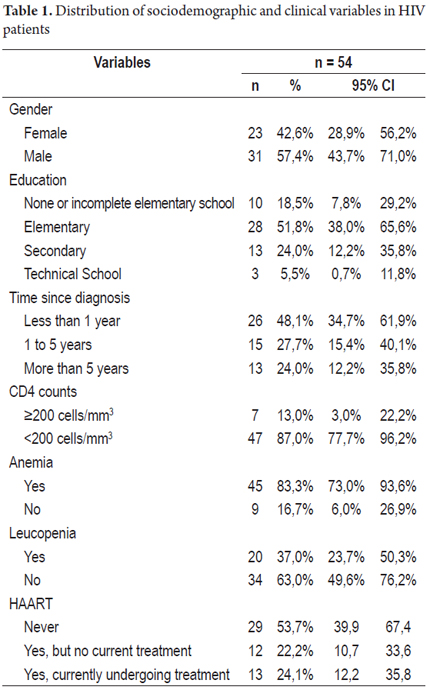
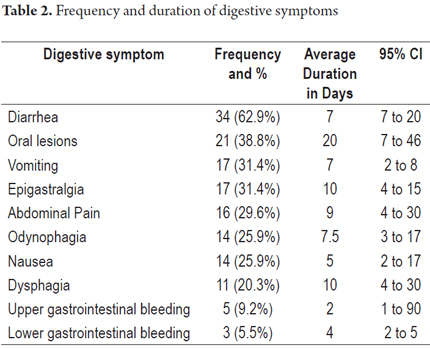
A total of 70 endoscopic procedures were performed on 54 patients, 41 upper endoscopies and 29 colonoscopies. Twenty-five patients underwent only upper endoscopies, thirteen patients underwent only colonoscopy, and sixteen patients underwent both. Average patient age was 39 years, the majority of patients were men, and the majority of patients had not finished elementary school. Table 1 shows the sociodemographic and clinical characteristics of patients in the study. Hemoglobin concentration averaged 10.9 g/dL (SD 2.8) in men and 9.6 g/dL (SD 1.9) in women. Anemia, according to the operational definition, was found in 45 patients (83.3%). Gender distribution of anemia was 24 men (53.3%) and 21 women (46.6%). The average CD4 count was 81.8 cells per mm3, and the average CD4 count for patients receiving HAART was 166.5 cells per mm3. HAART had been suspended in 44 patients (p = 0.014) who had an average of 59.7 cells per mm3 (p = 0.01). Two-thirds of the participants had hypoalbuminemia. The most common digestive symptoms were diarrhea and oral lesions. All the symptoms covered in the questionnaire are presented in Table 2 with their respective average durations.
Endoscopic and pathological findings of upper endoscopy
Table 3 shows that endoscopists reported more normal studies than any other type. Among the most frequent abnormal findings were esophagitis and erosive antral gastritis. Similarly, biopsy findings from both the esophagus and the stomach were most frequently normal.
Endoscopic and pathological findings of lower endoscopy
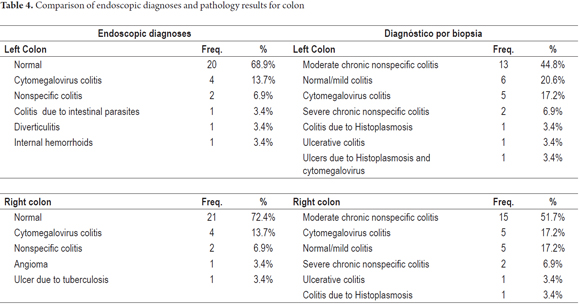
Table 4 shows that endoscopic diagnoses for both left and right colon were mostly normal study (about 70% of the sample). In contrast, the most common finding from biopsies for both left and right colon was moderate chronic nonspecific colitis.
DISCUSSION
According to our review of the academic literature, this study is one of the first to show the behavior of endoscopic and pathologic findings in a series HIV patients. In Latin America, the only similar study was conducted in Venezuela. (13) That study analyzed only the correlation between upper endoscopy and biopsies. Most of that patients in that study were men, as gender distribution that differs from that reported in the UNAIDS report which shows that the prevalence of HIV tends to be distributed equally between men and women. (1) In our series, the average age was 39.9 years which is similar to Colombian and regional references. In 2013 the average age of patients with HIV in Colombia was 39.3 years, and in the department of Santander the average age was 39.1 years indicating that this disease continues to be most prevalent during the years of working age. (2)
Diarrhea was the most frequently mentioned gastrointestinal symptom which is consistent with findings in the international literature. (14, 15) In our series the most frequently reported upper gastrointestinal symptoms were oral lesions. A recently published study done in Neiva, Colombia has found that the most frequent gastrointestinal symptoms in hospital patients with HIV were oral lesions (25.8%), diarrhea (23.7%) and abdominal pain (19.2%). (16 ) A 2004 study in Argentina found that the most frequent upper digestive tract symptoms were heartburn (73.5%), epigastric pain (73.5%) and postprandial bloating 65.7%. (17) A Belgian study found that abdominal discomfort (31.4%) was most common, that 16.1% had reflux, and that other symptoms accounted for 28.3%. (18) Since digestive signs and symptoms vary in patients with HIV/AIDS, they must be carefully studied to define a specific diagnosis.
Few publications disaggregate the diagnostic sensitivity of endoscopy and colonoscopy and even less in patients with HIV. Because the usual tendency is to present articles in which diagnostic performance targets a specific pathogen, this study's approach did not analyze data in terms of sensitivity and specificity of measures, given the heterogeneity of diagnoses found. Instead, we focused mostly on descriptions of endoscopic and pathologic findings but included the percentages of normal diagnoses reported by the endoscopists and pathologists for each abdominal organ.
Most of our pathology findings for the esophagus were normal, cases of candidiasis were second most numerous. It is noteworthy that there were no cases of eosinophilic esophagitis diagnosed since it is known to have an incidence of 0.4% in the general population, and its prevalence may be as high 54% in patients with histories of food impaction. (20) Other series have found candida, cytomegalovirus, herpes simplex virus and human papilloma virus to be frequent esophageal pathologies. (3, 13, 19, 20) Regarding comparison of the abilities of endoscopy and biopsies to detect normal, Table 3 shows that they are similar. This could be explained by the limited amount of opportunist infections in the esophagus. Nevertheless, it is still necessary to take biopsies from patients given that, when seen through an endoscope, the esophageal mucosa can appear to be normal when there are diseases such as eosinophilic esophagitis. (21)
Bibliographic references point to Cytomegalovirus and Mycobacterium avium opportunist infections in the stomach while they characterize Helicobacter pylori as non-opportunist. (22). In addition, neoplastic lesions such as non-Hodgkin's lymphoma and Kaposi's sarcoma are commonly found. (6, 18) This study's endoscopic findings for the stomach mucosa were mostly normal while pathological diagnoses found opportunist infections such as histoplasmosis and cytomegalovirus. Although no mycobacterial infections or gastric neoplasms were found, it is important to note that H. pylori was found in 8% of the sample. It should also be noted that the three cases of H. pylori appeared to be normal in the endoscopic study. The prevalence of H. pylori in the HIV population studied was lower than that reported in HIV-negative people in Colombia. (23) It should also be emphasized that the literature on Colombia contains no references on the prevalence of H. pylori in people with HIV. Limitations of this study were the size of the study population and lack of a control group. Additional studies are needed to properly determine the prevalence of H. pylori among the population of people with HIV in Colombia.
Table 4 shows results for the right and left colon. Unlike the results for the esophagus and stomach, the percentage of normal findings from histological study is much lower than the percentage of normal endoscopic diagnoses. This could be explained by the greater amount of bacteria and/or the large amount of lymphoid tissue in the colon which may lead to non-opportunistic diseases being the causes of symptoms. Nevertheless, it is clear that the numbers of pathologies and opportunistic diseases is higher in the colon than in the esophagus and stomach. (19) In turn, it is important to emphasize performance of diagnostic biopsies because mucosa that appears to be healthy to the endoscopist in patients with digestive symptoms may contain not only to opportunistic agents but other pathologies such collagenous colitis. (24 to 26) Another possible explanation for the high frequency of nonspecific pathological findings in the colon is that entities such as collagenous colitis, lymphocytic colitis and eosinophilic gastroenteritis are infrequently diagnosed in our environment and pathologists are unaccustomed to reporting them. (27)
Limitations of this study include not having used electron microscopy, immunohistochemistry, cultures, or molecular biology which implies that some patients who were reported to have normal mucosa may have actually had some pathological alteration. For example, electron microscopy can be used to identify small intestinal infections by Cryptosporidium and Histoplasma capsulatum. In terms of immunohistochemistry, FISH and PCR help identify viral infections such as cytomegalovirus and herpes simplex virus. (6, 28) Another limitation of this study was that viral load was not measured in patients. It is important to note that viral load can explain the direct action of the virus in causing mucosal symptoms if other causes are ruled out. Finally, it is possible that the sample size was not ideal for generalizations of findings, taking into account the heterogeneity of the diagnoses.
CONCLUSIONS
Endoscopic and pathological findings are consistent with frequencies of occurrence in the gastrointestinal tract reported in the literature, although no tumors or infectious agents such as mycobacteria, adenovirus, coronavirus were found. The most common opportunistic infection in the esophagus was Candida while the most common opportunistic infection in the colon was cytomegalovirus which was the overall most frequent opportunistic infection. There was a good correlation between endoscopic and pathological diagnosis only for normal findings in the esophagus. In the stomach and colon, disparity was evident. Therefore, atthis state of the art, it is recommended that regardless of observations of the endoscopist, protocols for patients with HIV/AIDS and digestive symptoms must include both endoscopies and biopsies. In addition, the prtocols for the pathological study should require microscopy with conventional staining, electron microscopy and immunohistochemistry to diagnose opportunistic and non-opportunistic etiologies. With this type of standard procedure, we should be able to arrive at precise etiologic diagnoses that can guide therapy appropriately in patients, prevent hospitalization and prevent severe or fatal outcomes.
Conflicts of interests
The authors declare that they have no conflicts of interest.
FINANCING
There was no special funding for this study.
REFERENCES
1. ONUSIDA, Informe sobre la Epidemia Mundial de SIDA 2012. [Internet]. [citado 24 de mayo de 2016]. Recuperado a partir de: http://www.unaids.org/sites/default/files/media_asset/20121120_UNAIDS_Global_Report_2012_with_annexes_es_1.pdf [ Links ]
2. CAC.CO_20150814_LIBROVIH2014_V-0.0.VERSIÓN FINAL---.pdf [Internet]. [citado 24 de mayo de 2016]. Recuperado a partir de: https://cuentadealtocosto.org/site/images/Publicaciones/CAC.CO_20150814_LIBROVIH2014_V-0.0.VERSI%C3%93N%20FINAL---.pdf [ Links ]
3. Torre D, Speranza F, Martegani R. Impact of highly active antiretroviral therapy on organ-specific manifestations of HIV-1 infection. HIV Med. 2005;6(2):66-78. [ Links ]
4. Knox TA, Spiegelman D, Skinner SC, Gorbach S. Diarrhea and abnormalities of gastrointestinal function in a cohort of men and women with HIV infection. Am J Gastroenterol. 2000;95(12):3482-9. [ Links ]
5. Fuyuno Y, Yamazaki K, Takahashi A, Esaki M, Kawaguchi T, Takazoe M, et al. Genetic characteristics of inflammatory bowel disease in a Japanese population. J Gastroenterol. 2015. [ Links ]
6. Bhaijee F, Subramony C, Tang S-J, Pepper DJ. Human immunodeficiency virus-associated gastrointestinal disease: common endoscopic biopsy diagnoses. Patholog Res Int. 2011;2011:247923. [ Links ]
7. Zeitz M, Ullrich R, Schneider T, Kewenig S, Riecken E. Mucosal immunodeficiency in HIV/SIV infection. Pathobiology. 1998;66(3-4):151-7. [ Links ]
8. Kearney DJ, Steuerwald M, Koch J, Cello JP. A prospective study of endoscopy in HIV-associated diarrhea. Am J Gastroenterol. marzo de 1999;94(3):596-602. [ Links ]
9. Sayilir A, Kurt M, Kekilli M, Onal IK, Beyazit Y, Turhan N, et al. Diagnostic value of terminal ileum biopsy in chronic diarrhea with normal endoscopic appearance. J Dig Dis. junio de 2011;12(3):188-92. [ Links ]
10. Nishimura S, Nagata N, Shimbo T, Asayama N, Akiyama J, Ohmagari N, et al. Factors associated with esophageal candidiasis and its endoscopic severity in the era of antiretroviral therapy. PLoS ONE. 2013;8(3):e58217. [ Links ]
11. Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut. 1999;45(2):172-80. [ Links ]
12. Satsangi J, Silverberg MS, Vermeire S, Colombel J-F. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut. junio de 2006;55(6):749-53. [ Links ]
13. Fernández S, Lecuna V, Ruiz ME. Comparación en el tracto digestivo superior entre los hallazgos endoscópicos y la biopsia en pacientes con síndrome de inmunodeficiencia adquirida (sida) con más de 200 células cd4 y menos de 200 células cd4. Gen. 2007;61(1):14-20. [ Links ]
14. Feasey NA, Healey P, Gordon MA. Review article: the aetiology, investigation and management of diarrhoea in the HIV-positive patient. Aliment Pharmacol Ther. 2011;34(6):587-603. [ Links ]
15. Ríos N, Núñez A, Chamorro C. Frecuencia de alteraciones gastrointestinales en pacientes con SIDA internados en el IMT en el año 2009 y 2010. Revista del Instituto de Medicina Tropical. 2014;6(2):6-10. [ Links ]
16. Agudelo González S, Murcia Sánchez F, Salinas D. Osorio J. Infecciones oportunistas en pacientes con VIH en el hospital universitario de Neiva, Colombia. 2007-2012. Infectio; 2015;52-59. [ Links ]
17. Olmos MA, et al. Evaluación endoscópica de pacientes VIH positivos con síntomas digestivos altos. Acta Gastroenterológica Latinoamericana. 2004;34:120-6. [ Links ]
18. Nkuize M, De Wit S, Muls V, Arvanitakis M, Buset M. Upper gastrointestinal endoscopic findings in the era of highly active antiretroviral therapy. HIV Med. 2010;11(6):412-7. [ Links ]
19. Al Anazi AR. Gastrointestinal opportunistic infections in human immunodeficiency virus disease. Saudi J Gastroenterol. abril de 2009;15(2):95-9. [ Links ]
20. Furuta GT, Katzka DA. Eosinophilic Esophagitis. N Engl J Med. 2015;373(17):1640-8. [ Links ]
21. Beltrán M, Constanza; García M, Raimundo; Espino E, alberto y Silva A, Claudia. Esofagitis Eosinofílica: Una entidad emergente. Rev. Otorrinolaringol. Cir. Cabeza Cuello. 2009;69(3):287-98. [ Links ]
22. Nevin DT, Morgan CJ, Graham DY, Genta RM. Helicobacter pylori gastritis in HIV-infected patients: a review. Helicobacter. octubre de 2014;19(5):323-9. [ Links ]
23. Gómez, Martín et al. Erradicación del Helycobacter pylori: encuesta realizada por la Asociación Colombiana de Gastroenterología. Rev Col Gastroenterol. 2015;30(1):25-31. [ Links ]
24. Narabayashi K, Murano M, Egashira Y, Noda S, Kawakami K, Ishida K, et al. Endoscopic and histopathological evaluation of collagenous colitis. Digestion. 2012;85(2):136-40. [ Links ]
25. Fernandes ER, Pagliari C, Tuon FF, de Andrade Junior HF, Averbach M, Duarte MIS. Chronic colitis associated with HIV infection can be related to intraepithelial infiltration of the colon by CD8+ T lymphocytes. Int J STD AIDS. agosto de 2008;19(8):524-8. [ Links ]
26. Arevalo F, Arias SC, Monge E. Biopsia de colon: características histológicas en diferentes tipos de Colitis Crónica. Rev gastroenterol Perú. 2008;28(2):140-9. [ Links ]
27. Ingle SB, Hinge Ingle CR. Eosinophilic gastroenteritis: an unusual type of gastroenteritis. World J Gastroenterol. 21 de agosto de 2013;19(31):5061-6. [ Links ]
28. Huppmann AR, Orenstein JM. Opportunistic disorders of the gastrointestinal tract in the age of highly active antiretroviral therapy. Hum Pathol. diciembre de 2010;41(12):1777-87. [ Links ]
