










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.31 no.4 Bogotá Oct./Dec. 2016
Prevalence of Gastro-Esophageal Reflux Symptoms and Associated Factors: A Population Survey in the Principal Cities Of Colombia
David B. Páramo-Hernández MD (1), Rosario Albis MD MSc (1), María T. Galiano MD (1), Belén de Molano MD (1), Reynaldo Rincón MD (1) Luis F. Pineda-Ovalle MD (1), Alberto Rodríguez MD (1), William Otero Regino MD (1), Albis Hani MD (1), Luis Carlos Sabbagh MD (1), Carolina Sandoval-Salinas MSc (1), Ricardo Sánchez-Pedraza MD MSc (1)
(1) Research Committee of the Colombian Association of Gastroenterology in Bogotá, Colombia
Received:Â Â Â 29-02-16Â Â Accepted:Â Â Â 01-11-16
Abstract
Problem: Gastroesophageal reflux is a physiological process that can become pathological in some people. It can cause discomfort and esophageal and extra-esophageal injuries and can affect the quality of life of anyone affected by it. Currently there are no statistics on the frequency of this condition in Colombia. Objective: The objective of this study was to use the GerdQ questionnaire to quantify the prevalence of gastroesophageal reflux disease in adults in four major cities of Colombia and to explore the association of sociodemographic and anthropometric variables with this disease.
Methodology: This was a cross-sectional population-based study of 6,842 people between the ages of 18 years and 80 in Bogotá, Cali, Medellín and Barranquilla. The sample was selected by stratified random sampling. A telephone survey was conducted that included the GERD Q questionnaire for the identification of reflux symptoms within the week prior to an interview. The prevalence of reflux by socioeconomic strata was calculated using a cut-off point of 8 or more points. Comparisons were made among strata using the Ï2 test. Associations of sociodemographic and anthropometric variables were explored through bivariate analysis and logistic regression models.
Results: We obtained 6,842 surveys. The overall estimated prevalence of reflux was 11.98% (95% CI = 11.05%-12.97%). The city of Barranquilla presented the highest frequency of 16.22% (95% CI = 14.58%-18.01%) while Bogotá had the lowest of 10.75% (95% CI = 9.30%-12.38%). For symptoms evaluated with GERD-Q, the estimated prevalences were: heartburn 13.6% (95% CI = 12.50% - 14.60%), regurgitation 16.9% (95% CI = 15, 74% - 17.99%), epigastralgia 16.67% (95% CI = 15.54% -17.80%), nausea 11.4% (95% CI = 10.46% - 12.35%), difficulty sleeping due to heartburn or regurgitation 8.17% (95% CI = 7.36% -8.97%) and consumption of medications additional to those formulated by the physician 6.68% (95% CI = 6, 01% - 7.35%). Women living in Barranquilla or Medellín, had statistically significant levels of comorbidities associated with reflux.
Conclusion: The prevalence of reflux in four important Colombian cities measured with the GerdQ questionnaire was 11.98% (95% CI = 11.05-12.97) which is similar to prevalences reported in other Latin American countries. Comorbidities (particularly hypertension) are the factor that was most frequently associated with this condition in all strata of the study.
Keywords
Prevalence, symptoms, gastroesophageal reflux, Gerd Q, associated factors.
Introduction
Worldwide, gastroesophageal reflux disease (GERD) affects a large number of people and is a major burden on health care systems because of the high number of consultations it generates, the costs of medicines, the reduction of quality of life, (1, 2) and its impact on labor productivity. (3-7) In North America and Europe, the prevalence of reflux in adults varies from 10% to 20% (8) in population studies that measure weekly occurrence of symptoms. A similar figure has been observed in Latin America, where the estimated prevalence of symptoms such as heartburn and regurgitation, experienced at least weekly, has been reported at between 11.9% and 31.3%. (9) In Asia the prevalence described ranges from 2.5% to 6.7%. (10) In Western countries, it has been estimated that gastroesophageal reflux care is the reason for 5% of primary care consultation. (5) In Brazil, the probability of a medical consultation for people with weekly symptoms of reflux is twice as high as those with less frequently occurring symptoms. (1)
In many parts of the world studies at the population and hospital levels have been carried out to determine the frequency of GERD. Studies have looked at GERD's association with sociodemographic, environmental, genetic and other factors as well as the possibility that it is a risk factor for development of diseases such as esophageal adenocarcinoma, cardiac carcinoma and squamous cell carcinoma of the esophagus. (1, 11-29) However, comparisons of studies are difficult because they are very heterogeneous, define the disease in different ways, have different methodologies, and use a diversity of instruments for diagnosis. These include standardized questionnaires such as GERDQ, questionnaires created by the investigators (some of which are not validated), much more specific tests such as endoscopy, pH measurements, and esophageal manometry. These are difficult to use in population studies given their operational complexity and high costs. GERDQ allows identification of typical symptoms of reflux and has a sensitivity of 65% and a specificity of 71% which is in the range of diagnosis by gastroenterologists. (11) GERDQ has been validated in our population and has been observed to have an 89% correlation with diagnoses performed by gastroenterologists when the score obtained is greater than 8 points. (30)
Although GERD is a frequent reason for primary and specialist medical consultation in Colombia, we do not have sufficient information to suggest its prevalence or associations. Knowing the population prevalence of gastroesophageal reflux in our country would be useful for proposal and direction of activities to control this disease, as well as for promoting educational activities related to diagnosis and treatment of this pathology in Colombia. The objectives of this study are to quantify the prevalence of GERD symptoms in adults in four cities of Colombia using the GERDQ questionnaire and to explore associations with sociodemographic and anthropometric variables.
Methodology
This observational, cross-sectional, population-based study was conducted in four of Colombia's major cities: Barranquilla, Bogotá, Cali and Medellín, from February to July 2014. The study used a stratified random sampling design.
Calculation of Sample Size
Based on the 2005 census, DANE (Departamento Administrativo Nacional de Estadística - the National Administrative Department of Statistics) projected that there were 38,196,000 people living in Colombia in 2013. Of these, 27,501,120 people (72%) live in urban areas. From this population, a sample size of 1,537 individuals per city was calculated for an expected 20% prevalence of reflux symptoms with absolute accuracy of 2% around the estimator and a 95% confidence level. Considering a non-response effect of a telephone strategy of 1.3, the calculation was adjusted to 1,998 people per city, for a total of 7,992 individuals. Taking into account that it is not necessary to increase the sample size to maintain the parameters of precision, accuracy and confidence for populations of finite size larger than 500,000 inhabitants, and that for each city in this study the population is over 500,000 (Bogotá: 5,382,729; Medellín: 1,811,680; Cali: 1,621,057; Barranquilla: 821,907), the sample size for each city (stratum) was set at the same magnitude of 1,998 people.
If obesity is considered to be a variable that can skew the overall stratum estimator (the presence of obesity is associated with a higher frequency of reflux symptoms), this sample size allows maintenance of an accuracy of 5% around the symptom estimator of reflux for the subgroup of non-obese individuals, assuming a prevalence of obesity of 20%.
Sample size was calculated with PASS 12® software.
The selection of strata took into account the need to incorporate capital cities representing different social and cultural groups within the country.
Men and women between the ages of 18 and 79 who were residents of one of these four cities and who agreed to participate in the study were included. Pregnant women, people with current digestive neoplasia, and people who had undergone upper digestive tract surgery were excluded because these conditions may result in gastrointestinal symptoms which could lead to overestimation of the prevalence of GERD. In addition, people who are citizens of countries other than Colombia were excluded.
All the people who agreed to participate were surveyed by telephone. The survey included sociodemographic and anthropometric variables and the GERDQ questionnaire which has been validated for Colombia. (30) This tool has four positive GERD predictors: retrosternal burning (heartburn), regurgitation, sleep disturbances due to these two symptoms, and use of additional medications to relieve these symptoms. It also has two negative predictors of GERD: epigastric pain and nausea. (11)
Procedures
A preliminary design of the instrument used for the telephone survey was tested in a pilot study to adjust the content and sequence of the questions and to standardize the method of application. This study was carried out with 20 adult volunteers from each of the cities that formed the strata of the study.
Once a definitive version of the measuring instrument was obtained, one of the researchers hired and trained professional health technicians who used a call center to conduct the telephone survey of selected households. The selection criteria proposed in this study were applied to the person who answered the phone call. In case that person did not meet the criteria, the caller checked to find out if another member of the household might met the criteria and participate in the study. Survey results for variables described above showed that for anthropometric variables of weight and height there was an intraclass correlation coefficient between self-reporting and direct measurement of 0.956 for weight (95% CI: 0.95-0.97) and 0.953 for height (95% CI: 0.91-0.97) which is why the degree of error in the data provided by the participants in the telephone survey is considered tolerable.
To control quality, 10% of the people initially surveyed were called to verify the information they had given in the first interview.
The information was collected in a physical electronic format which allowed for capture of information and was then recorded in a database in Access. Recording was done weekly in batches of 500 forms, in duplicate, by independent data entry clerks. Once the recording of all forms was completed, a comparison was made between the records from each data entry clerk. Inconsistencies were adjusted by checking the respective formats. Once a definitive clean base was obtained, data was exported to Stata program where the required statistical analysis was performed.
Ethical Issues
This study adheres to the principles for human research set out in the Helsinki Declaration of the World Medical Association, the ethical guidelines provided by the Council of International Organizations of Medical Sciences (CIOMS) and the Belmont Report, and the legal and ethical guidelines described in Resolution 8430 of 1993 of the Ministry of Health of Colombia and other Colombian regulations.
Since this was an observational study which only used telephone surveys and which did not include any intentional intervention or modification of the biological, physiological, psychological or social variables of the individuals who participated in the study, Colombian Ministry of Health Resolution 8430 of 1993 classifies it as research without risk. For this reason, written informed consent was not considered necessary. However, the protocol was submitted for evaluation to the Research Ethics Committee of Santa Clara Hospital which approved the protocol in March 2014. The record is in the offices of the Colombian Association of Gastroenterology.
The confidentiality of the participants was ensured by restricting access to identification data only to people conducting the surveys and to the study coordinator. An assigned identification code was registered on data collection forms so that identities of individuals included in the study could not be revealed.
The results of this study will be published in academic and scientific journals and will be presented in the form of general data rather than information about particular participants.
People who decided to participate in this study who were identified as having reflux were advised to consult a physician for treatment of their illness.
Statistical analysis
Descriptive analysis of the population was performed by estimating absolute and relative frequencies for the qualitative variables and measures of central tendency and dispersion for the quantitative variables. The prevalence of GERD was estimated along with its corresponding 95% confidence interval from the GERDQ questionnaire. This established a cut-off point of eight points or more for the diagnosis of reflux. The prevalence of GERD symptoms in the week prior to the survey was also established with this tool.
For analyses of associations between reflux and socio-demographic and anthropometric variables, bivariate analyses were initially performed using ANOVA tests for continuous variables and Chi2 for categorical variables. For all hypothesis tests, significance values ââof 5% and two-tailed tests were considered. Later, models of association were developed to evaluate and quantify the relationship between anthropometric and sociodemographic variables and the presence of reflux. Binary and ordinal logistic regression models were used in which the odds ratios (OR) corresponding to the transformed regression coefficients were taken as estimators.
Analyses were performed in Stata 13® software and the effect of the sample design was incorporated into the calculation.
Results
We called 9,222 people of which 6,842 were included in the analysis. Individuals called were excluded if they decided not to participate (1,645 individuals), did not meet the age criterion, had had surgery of the esophagus or stomach (195 individuals), had been diagnosed with cancer (9 individuals), were not Colombians (35 individuals), or were pregnant (36 individuals).
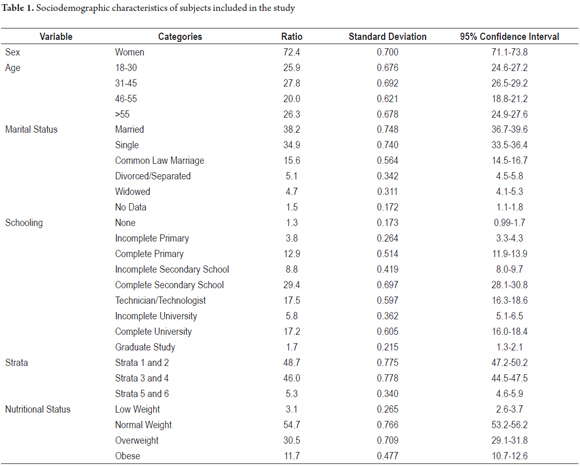
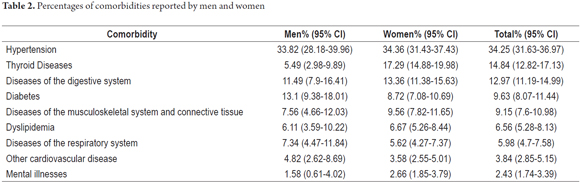
Table 1 shows characteristics of the subjects included in the study. The average age was 44.07 years (95% CI: 43.58-44.56), the majority were women, the most frequently found level of schooling was completion of secondary education, the most frequent marital status was married, and the majority of the population lived in socioeconomic strata 2 and 3 (Translator's note: Colombia has 6 legally defined income and geography based strata used for purposes of taxation and subsidies). It was observed that the majority of the population had normal weights, although a 30.5% were overweight (95% CI: 29.1-31.8). Cigarette smokers made up 9.5% (95% CI: 8.6-10.4) of the respondents, and 15.8% (95% CI: 14.7-16.9) reported having consumed liquor in the week prior to the survey. Comorbidities were reported by 27.1% (95% CI: 25.8-28.5). Hypertension, diabetes and digestive tract diseases were most frequent among men while hypertension, thyroid pathologies (hyperthyroidism or hypothyroidism), and digestive tract diseases were most frequent among women (Table 2).
The overall prevalence of reflux symptoms for the population according to the GERDQ questionnaire was as follows:
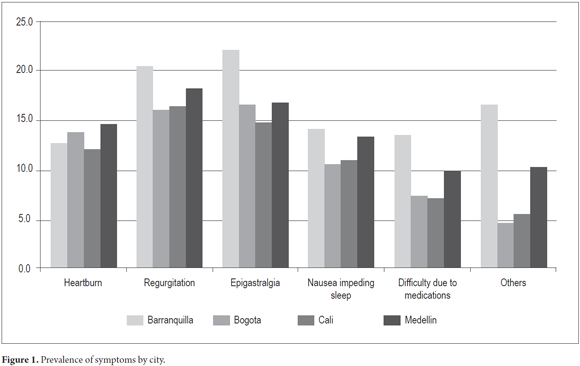
Heartburn, 13.6% (95% CI: 12.50-14.60); Regurgitation, 16.9% (95% CI: 15.74-17.99); Epigastralgia, 16.67 (95% CI: 15.54-17.80); Nausea, 11.4% (95% CI: 10.46-12.35); Difficulty sleeping due to heartburn or regurgitation, 8.17% (95% CI: 7.36-8.97); Consumption of medications other than those formulated by a physician, 6.68% (95% CI: 6.01-7.35). The prevalence of reflux symptoms by cities is presented in Figure 1 where it can be seen that, except for heartburn, all symptoms were most frequent in Barranquilla. Heartburn was most frequent in Medellín (14.6%; 95% CI: 12.93-16.29).
The prevalence of reflux symptoms for the entire population was 11.98% (95% CI: 11.05-12.97). Barranquilla had the highest figure (16.22%, 95% CI: 14.58-18.01), followed by Medellin (14.06%, 95% CI: 12.49-15.79), Cali (11.6%, 95% CI: 10.17-13.19) and Bogota (10.75%, 95% CI: 9.30-12.38).
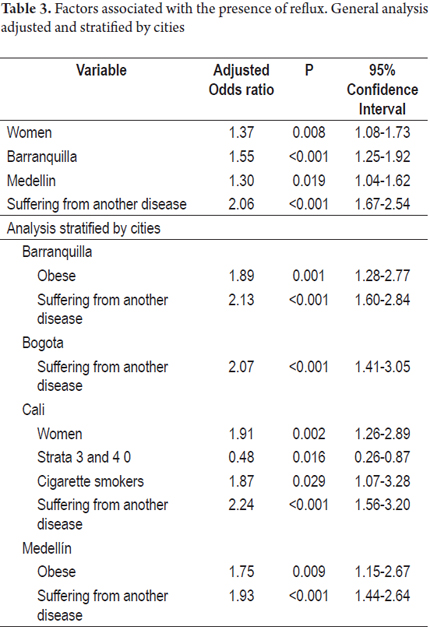
The multivariate analysis showed that being female, living in Barranquilla or Medellín (rather than Bogota) and having a comorbidity were factors that are statistically associated with the presence of reflux in the general population. Multivariate analysis by city showed that in addition to comorbidity, which is a risk factor for reflux in all cities, in Barranquilla and Medellín obese people had higher risks of GERD than did people whose weights were normal or low. The Odds Ratio for obese people was 1.89 (95% CI: 1.28-2.77) while the OR for people with normal weight was 1.75 (95% CI: 1.15-2.67). In Cali, women had higher risks than men (OR: 1.91, 95% CI: 1.26-2.89), and smokers had higher risks than non-smokers (OR: 1.87, 95% CI: 1.07-3.28). It was also found that living in strata 3 and 4 is a protective factor compared to living in strata 5 and 6 (OR: 0.48; 95% CI: 0.26-0.87) (Table 3).
Discussion
GERD results from the retrograde flow of gastric contents in the esophagus or organs adjacent to it. This produces a variable spectrum of esophageal and/or extraesophageal signs and symptoms and may damage tissue. The Montreal consensus of 2006 defined GERD as a condition that develops when reflux of gastric contents causes annoying symptoms or complications. (31)
GERD is a clinical entity that has a varied spectrum of presentations and symptoms which may not correlate with endoscopic findings. (31-33) Patients may present a combination of manifestations:
- Typical symptoms of reflux with endoscopic findings of esophageal mucosal damage
- Typical symptoms of reflux with normal endoscopy
- No typical reflux symptoms, but endoscopic evidence of mucosal damage
- Atypical symptoms such as dyspepsia, coughing and asthma. (31, 32)
The symptoms considered typical of GERD are heartburn and regurgitation: a sensitivity of 78% and a specificity of 60% for the presence of GERD were originally estimated for these symptoms. (31, 34)
GERD-related symptoms are classified as annoying when they adversely affect the patient's quality of life in relation to their health. Symptoms that are not considered annoying by the patient should not be diagnosed as GERD. In population studies, mild symptoms experienced for two or more days per week were considered to be annoying, moderate or even severe when experienced at least one day per week. Nevertheless, symptom frequency thresholds used to define GERD vary widely among epidemiological studies aimed at assessing the prevalence of this disease. (9, 31)
This study used the GERDQ questionnaire, a diagnostic tool based on symptoms, to assess the prevalence of the disease. This instrument was validated in Colombia, (11, 30) and uses a cut-off score of eight which means that those with a score greater than or equal to eight have a high probability of having GERD and that those with a lower score have a low probability of having GERD. A cutoff point of eight has the highest specificity (71.4%) and sensitivity (64.6%), and several studies have shown that the GERDQ questionnaire achieves diagnostic accuracy similar to that of gastroenterology. (11, 35-37)
Diagnosis of the prevalence of reflux in four principal cities of Colombia using the GERDQ questionnaire had results that are similar to those reported in several other Latin American countries although it is one of the lowest in this region. (9, 12, 38) Discordance with countries such as Venezuela, Brazil and Mexico, where the reported GERD frequency is higher, can be explained by methodological differences with these studies in terms of the test used to diagnose the disease, the type of population, the data collection methodology and time evaluation of symptoms which were not always the same as those in our study. (1, 19, 22, 39, 40) However, a person-to-person survey conducted by Moraes-Filho et al. using a significant population sample (n = 13,959) in an urban Brazilian population found a weekly prevalence of heartburn that is close to ours. (41)
The results of the analysis of the relationships between reflux frequency and sociodemographic and anthropometric variables in the four cities included in the study showed a pattern that is typical of our population and which coincides with some of the risk factors found in other countries in the region. An example of this is the association of reflux with women which has been documented in other studies in Latin America, (19, 21, 22, 24, 39-42) but which differs from the results of studies performed in populations in the United States and China where reflux is more frequent among men than among women. (14, 16-18, 25-28) When GERD symptoms are assessed, the prevalence by gender varies in different countries. However, when GERD complications are assessed (more specific variables), data consistently indicate that the disease is more common in men. One possibility that would explain the higher prevalence in women in this study is that functional esophageal symptoms are more frequent among women than among men. Various studies have shown that entities such as functional heartburn, globus pharyngis and non-cardiogenic chest pain are more prevalent in women. (43-47)
In this study, the comorbidities most commonly associated with reflux were cardiovascular and thyroid diseases predominated. This is a contrast to other studies in which gastrointestinal comorbidities such as irritable bowel syndrome, peptic ulcers, dysphagia and dyspepsia have been observed at higher frequencies with reflux symptoms. (17, 43) Statistical associations with other non-digestive diseases such as coughing, gallbladder disease, sinusitis, chest pain and even mental illnesses such as depression and anxiety have also been demonstrated. (15, 43)
Associations of nutritional status, cigarette smoking and alcohol consumption with GERD have previously been reported by a number of authors but were all insignificant in our study. This could be explained by variability in the measurement of these variables. (1, 16-18, 21, 24-26, 42-45)
The data generated in this study provide a reliable estimate of the prevalence of reflux in the four cities in which the survey was conducted. This is attested to by the large sample size and the use of a tool that has a high correlation with the diagnosis performed by a gastroenterologist and that has been validated in several countries including Colombia. (11, 20, 30) In addition, the data allow differentiation of specific symptoms of reflux and the degree of severity of this disease. (11) Another strength of this study is the inclusion of different sociocultural groups of the country in representative cities which allows an approximation of the prevalence of reflux in Colombia. However, there are methodological weaknesses such as the limitation of phone calls only to landlines which excluded a part of the population, especially in rural areas. We must also consider that there were obvious selection biases in the predominance of the female gender in the sample and the important prevalence of cardiovascular comorbidity of close to 40%, possibly accompanied by polymedication which could modify the prevalence of GERD symptoms.
From the point of view of public health, this contribution to our knowledge of the epidemiology of GERD in our country allows us to quantify and plan resources for care of this type of pathologies and also for assessment of explanatory variables and risk factors that could be the basis of preventive medical care. On the other hand, in clinical practice the use of questionnaires such as the GERDQ that have been validated and have satisfactory pretest probability is recommended because it rationalizes use of diagnostic resources, particularly in primary care. (30, 46) The development of additional prevalence studies using validated instruments will allow for monitoring and surveillance of gastroesophageal reflux, especially efforts to modify risk factors.
Conflicts of Interest
This study was carried out by the Research Committee of the Colombian Association of Gastroenterology with funds from the following pharmaceutical companies: Bussié, Galeno, Grupo Farma, Reckitt Benckiser, Takeda and Tecnoquímicas-MK. The GERDQ form was provided by AstraZeneca Laboratories.
References
1. Pereira-Lima J, Blaya C, Rynkowski CB, et al. Population-based study on the prevalence of gastroesophageal reflux disease in Porto Alegre, Rio Grande do Sul. GED Gastroenterol Endosc Dig. 2014;19(2):73-8. [ Links ]
2. Wiklund I. Review of the quality of life and burden of illness in gastroesophageal reflux disease. Dig Dis. 2004;22(2):108-14. [ Links ]
3. Enck P, Dubois D, Marquis P. Quality of life in patients with upper gastrointestinal symptoms: results from the Domestic/International Gastroenterology Surveillance Study (DIGEST). Scand J Gastroenterol. 1999;34(231):48-54. [ Links ]
4. Haycox A, Einarson T, Eggleston A. The health economic impact of upper gastrointestinal symptoms in the general population: results from the Domestic/International Gastroenterology Surveillance Study (DIGEST). Scand J Gastroenterol. 1999;34(231):38-47. [ Links ]
5. Liker H, Hungin P, Wiklund I. Managing gastroesophageal reflux disease in primary care: the patient perspective. J Am Board Fam Pract. 2005;18(5):393-400. [ Links ]
6. Wahlqvist P, Reilly MC, Barkun A. Systematic review: the impact of gastro-oesophageal reflux disease on work productivity. Aliment Pharmacol Ther. 2006;24(2):259-72. [ Links ]
7. Mason J, Hungin AP. Review article: gastro-oesophageal reflux disease--the health economic implications. Aliment Pharmacol Ther. 2005;22 Suppl 1:20-31. [ Links ]
8. Dent J, El-Serag HB, Wallander M, et al. Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2005;54(5):710-7. [ Links ]
9. Salis G. Revisión sistemática: epidemiología de la enfermedad por reflujo gastroesofágico en Latinoamérica. Acta Gastroenterol Latinoam. 2011;41(1):60-9. [ Links ]
10. Wong BCY, Kinoshita Y. Systematic review on epidemiology of gastroesophageal reflux disease in Asia. Clin Gastroenterol Hepatol. 2006;4(4):398-407. [ Links ]
11. Jones R, Junghard O, Dent J, et al. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Aliment Pharmacol Ther. 2009;30(10):1030-8. [ Links ]
12. Dacoll C, Umpierre V, Villa-Gómez M, et al. Prevalencia de la enfermedad por reflujo gastroesofágico en. Uruguay Gastroenterol Hepatol. 2012;35(7):460-7. [ Links ]
13. Eggleston A, Farup C, Meier R. The Domestic/International Gastroenterology Surveillance Study (DIGEST): design, subjects and methods. Scand J Gastroenterol Suppl. 1999;34(231):9-14. [ Links ]
14. Guozong P, Guoming X, Meiyun K, et al. Epidemiological study of symptomatic gastroesophageal reflux disease in China: Beijing and Shanghai. Chin J Dig Dis. 2000;1(1):2-8. [ Links ]
15. Hu WHC, Wong W-M, Lam CLK, et al. Anxiety but not depression determines health care-seeking behaviour in Chinese patients with dyspepsia and irritable bowel syndrome: a population-based study. Aliment Pharmacol Ther. 2002;16(12):2081-8. [ Links ]
16. Isolauri J, Laippala P. Prevalence of symptoms suggestive of gastro-oesophageal reflux disease in an adult population. Ann Med. 1995;27(1):67-70. [ Links ]
17. Locke GR, Talley NJ, Fett SL, et al. Risk factors associated with symptoms of gastroesophageal reflux. Am J Med. 1999;106(6):642-9. [ Links ]
18. Mohammed I, Cherkas LF, Riley SA, et al. Genetic influences in gastro-oesophageal reflux disease: a twin study. Gut. 2003;52(8):1085-9. [ Links ]
19. Moraes-Filho JPP, Chinzon D, Eisig JN, et al. Prevalence of heartburn and gastroesophageal reflux disease in the urban Brazilian population. Arq Gastroenterol. 2014;42(2):122-7. [ Links ]
20. Mungan Z. Prevalence and demographic determinants of gastroesophageal reflux disease (GERD) in the Turkish general population: a population-based cross-sectional study. Turk J Gastroenterol. 2012;23(4):323-32. [ Links ]
21. Nader F, da Costa JSD, Nader GA, et al. Prevalence of heartburn in Pelotas, RS, Brasil: population-based study. Arq Gastroenterol. 2003;40(1):31-4. [ Links ]
22. Peralta-Pedrero ML, Lagunes-Espinosa AL, Cruz-Avelar A, et al. Frequency of gastroesophageal reflux disease in elderly patients attending a family medicine clinic. Rev Med Inst Mex Seguro Soc. 2007;45(5):447-52. [ Links ]
23. Ponce J, Vegazo O, Beltrán B, et al. Prevalence of gastro-oesophageal reflux disease in Spain and associated factors. Aliment Pharmacol Ther. 2006;23(1):175-84. [ Links ]
24. Veitía G, Sandoval C, Paredes R, et al. Prevalencia de enfermedad por reflujo gastroesofágico en población adulta del área metropolitana de Caracas, Venezuela. Rev Gastroenterol Nac GEN. 2008;62(2):109-13. [ Links ]
25. Wong WM, Lai KC, Lam KF, et al. Prevalence, clinical spectrum and health care utilization of gastro-oesophageal reflux disease in a Chinese population: a population-based study. Aliment Pharmacol Ther. 2003;18(6):595-604. [ Links ]
26. Kotzan J, Wade W, Yu HH. Assessing NSAID prescription use as a predisposing factor for gastroesophageal reflux disease in a Medicaid population. Pharm Res. 2001;18(9):1367-72. [ Links ]
27. Locke GR, Talley NJ, Fett SL, et al. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112(5):1448-56. [ Links ]
28. Nouraie M, Razjouyan H, Assady M, et al. Epidemiology of gastroesophageal reflux symptoms in Teheran, Iran: a population- based telephone survey. Arch Iran Med. 2007;10(3):289-94. [ Links ]
29. Lagergren J, Bergstrom R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340(11):825-31. [ Links ]
30. Santa María M, Jaramillo M, Otero Regino W, et al. Validación del cuestionario de reflujo gastroesofágico "GERDQ" en una población colombiana. Rev Col Gastroenterol. 2013;28(3):199-206. [ Links ]
31. Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Z Gastroenterol. 2006;45(11):1125-40. [ Links ]
32. Bredenoord AJ. Mechanisms of reflux perception in gastroesophageal reflux disease: a review. Am J Gastroenterol. 2012;107(1):8-15. [ Links ]
33. Vakil N, Malfertheiner, Salis G, et al. An international primary care survey of GERD terminology and guidelines. Dig Dis. 2008;26(3): 231-6. [ Links ]
34. Klauser AG, Schindlbeck NE, Müller-Lissner SA. Symptoms in gastrooesophageal reflux disease. Lancet. 1990;335(8683):205-8. [ Links ]
35. Tytgat GN, McColl K, Tack J, et al. New algorithm for the treatment of gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2008;27(3):249-56. [ Links ]
36. Jones R, Coyne K, Wiklund I. The gastro-oesophageal reflux disease impact scale: a patient management tool for primary care. Aliment Pharmacol Ther. 2007;25(12):1451-9. [ Links ]
37. Hambleton R. Adaptación de tests para uso en diferentes idiomas y culturas: fuentes de error, posibles soluciones y directrices prácticas. En: Muñiz J. Psicometría. Madrid: Editorial Universitas; 1996. p. 207-238. [ Links ]
38. Chiocca JC, Olmos JA, Salis GB, et al. Prevalence, clinical spectrum and atypical symptoms of gastro-oesophageal reflux in Argentina: a nationwide population-based study. Aliment Pharmacol Ther. 2005;22(4):331-42. [ Links ]
39. De Oliveira SS, dos Santos Ida S, da Silva JFP, et al. Gastroesophageal reflux disease: prevalence and associated factors. Arq Gastroenterol. 2005;42(2):116-21. [ Links ]
40. Schmulson M, Ortíz O, Santiago-Lomeli M, et al. Frequency of functional bowel disorders among healthy volunteers in Mexico City. Dig Dis. 2006;24(3-4):342-7. [ Links ]
41. Moraes-Filho JP, Chinzon D, Eisig JN, et al. Prevalence of heartburn and gastroesophageal reflux disease in the urban Brazilian population. Arq Gastroenterol. 2005;42(2):122-7. [ Links ]
42. Manterola C, Bustos L, Vial M. Prevalencia de enfermedad por reflujo gastroesofágico en población general urbana adulta. Rev Chil Cir. 2005;57(6):476-82. [ Links ]
43. Ruigómez A, García Rodríguez LA, Wallander M-A, et al. Natural history of gastro-oesophageal reflux disease diagnosed in general practice. Aliment Pharmacol Ther. 2004;20(7):751-60. [ Links ]
44. Watanabe Y, Fujiwara Y, Shiba M, et al. Cigarette smoking and alcohol consumption associated with gastro-oesophageal reflux disease in Japanese men. Scand J Gastroenterol. 2003;38(8):807-11. [ Links ]
45. El-Serag HB, Petersen NJ, Carter J, et al. Gastroesophageal reflux among different racial groups in the United States. Gastroenterology. 2004;126(7):1692-9. [ Links ]
46. Salis G. Revisión sistemática: epidemiología de la enfermedad por reflujo gastroesofágico en Latinoamérica. Acta Gastroenterol Latinoam. 2011;41(1):7-8. [ Links ]
47. Oh JH, Choi MG, Park JM, et al. The clinical characteristics of gastroesophageal reflux disease in patients with laryngeal symptoms who are referred to gastroenterology. Dis Esophagus. 2013;26(5):465-9. [ Links ]

