










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Español (pdf)
Español (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957
Rev Col Gastroenterol vol.32 no.1 Bogotá ene./mar. 2017
https://doi.org/https://doi.org/10.22516/25007440.134
The Cost Of Ignoring Carnett's Sign: A Case Report and Literature Review
William Otero Regino MD (1), Erika Martínez Rodríguez MD (2), Â Adán Lúquez Mindiola MD. (3)
(1) Professor of Medicine and Coordinator of Gastroenterology at the National University of Colombia and the National University Hospital of Colombia in Bogotá, Colombia. Mail: waoteror@gmail.com
(2) Internal Medicine Resident at the National University of Colombia and the National University Hospital of Colombia in Bogotá, Colombia.
(3) Internist and Gastroenterology Fellow at the National University of Colombia and the National University Hospital of Colombia in Bogotá, Colombia.
Received:Â Â Â 18-07-16Â Â Accepted:Â Â Â 16-12-16
Abstract
Chronic abdominal pain is a frequent cause of outpatient and emergency visits. Doctors traditionally consider that its origin is in intra-abdominal structures, including the gastrointestinal tract. They rarely take into account the abdominal wall as a cause of discomfort and subject patients to numerous and endless diagnostic procedures, including laparoscopy and surgery. At least 50% of these patients have abdominal wall pain due to injuries to the anterior cutaneous vein the diagnosis of which is made by identifying Carnett's sign. A typical case of this pathology is here. The initial approach illustrates the errors and high costs that can be involved in the approach to this pathology.
Key words
Chronic abdominal pain, anterior cutaneous nerve, Carnett's sign, costs.
INTRODUCTION
Chronic abdominal pain has multiple causes and is a challenge for primary care physicians, specialists and professionals at referral hospitals. (1-3). In gastroenterology, 50% of patients have idiopathic pain, and it has been observed that in 10% to 90% of these cases the pain originates in the structures of the abdominal wall. Among these cases, a lesion or compression affecting the anterior cutaneous nerve is the most frequent etiology. (2-5) However, physicians usually consider that the cause is located in the abdominal viscera and rarely think about the possibility of studying the abdominal wall. (1, 3, 5) After investigating visceral causes, patients end up diagnosed with psychosomatic illnesses, irritable bowel syndrome (IBS), gastritis and other disorders and are treated with analgesics, anxiolytics, antidepressants or benzodiazepines. It is not uncommon for them to be referred to psychiatry. In this article, we report a typical case of how this symptom is addressed by primary care physicians and referral centers.
Clinical Case
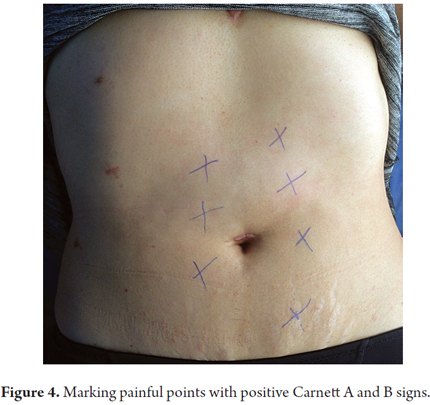
The patient was a 58-year-old man who had come to the emergency department numerous times during the previous year because of abdominal pain located in the hypochondriac and left flank. He had no other associated symptoms, nor did he have any signs of organic compromise. The patient had a history of dyslipidemia and an uncle who had had colon cancer. After being hospitalized for the second time due to persistent abdominal pain, blood chemistry tests, urinalysis, abdominal ultrasound and a CT scan were all normal. The general surgery service had ruled out acute abdomen and referred the patient for upper digestive endoscopy which resulted in chronic gastritis. Due to persistent abdominal pain, they requested ultrasound of the abdominal wall, which was normal. They continued the study with colonoscopy, which was also normal. On the fourth day, they asked for a gastroenterological assessment. Upon physical examination, the Carnett's Signs A and B (indicative of abdominal wall pain) were evident. The gastroenterological physical examination of the abdomen found no other abnormalities. The painful sites were infiltrated with lidocaine and the pain disappeared immediately. Three hours later, the patient was discharged.
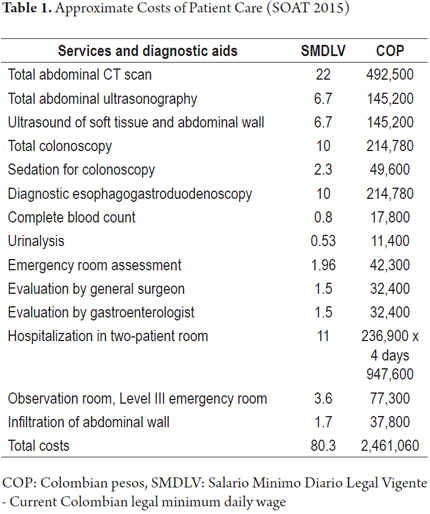
The approximate costs of this patient's last visit to the emergency department are shown in Table 1. Costs are based on the SOAT rates of 2015 (Ministry of Social Protection of Colombia, SOAT Tariff Manual, Decree 2423 of 2006 - updated in 2015) and do not include medicines.
DISCUSSION
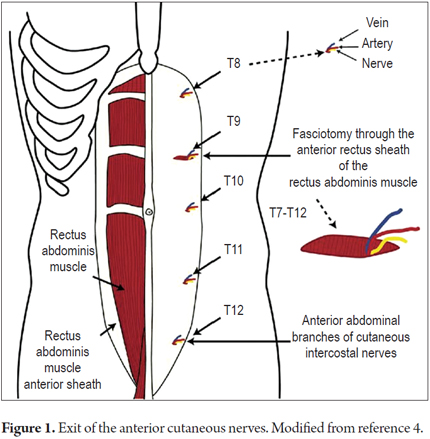
With the advent of increasingly modern and efficient diagnostic equipment and tests, interest in physical examination of patients in various clinical medicine settings has gradually been lost. This inattention is producing excessive increases in requests for diagnostic aid that, as in this case, would have been unnecessary if an adequate physical examination had been done. Chronic abdominal pain may originate in structures of the abdominal wall, including the skin, subcutaneous cellular tissue, parietal peritoneum, muscles and anterior cutaneous nerves from the dorsal roots of T7 to T12 which is the most frequent cause of this pain. (4, 5)
Cutaneous sensory nerves emerge from the T7-T12 nerve roots. They angle 90 degrees as they pass through the fibrous ring of the lateral border of the anterior rectus muscles and have similar angulation as they reach the skin. (2, 4) These angulations make them particularly vulnerable to trauma or entrapment.
In 1977, Thompson and colleagues concluded that identification of Carnett's sign can differentiate between irritation of the visceral peritoneum and pain caused by compression or entrapment of the anterior cutaneous nerve which is the main cause of chronic abdominal wall pain (CAWP). (1, 2) Unnecessary and costly examinations, invasive procedures and other items that economically impact health care services can be avoided with this brief physical examination. (1, 2) Abdominal pain is one of the three most common reasons for frequent emergency and outpatient consultations and has an incidence of approximately 8% in the studies in the literature. (3) Of these, 30% correspond to chronic abdominal wall pain. (3, 4) In our environment, another study by one of the authors, William Otero, and a group of colleagues found that almost 50% of patients with chronic abdominal pain lasting more than four weeks had CAWP identified through Carnett's sign. (2) These patients had also undergone multiple examinations, taken several medications, and had even undergone surgery and had been hospitalized. A third of them had been diagnosed with IBS.
After discarding a surgical cause of abdominal pain, there are multiple etiological possibilities. Recently, it has been found that applying a very simple questionnaire identifies chronic abdominal wall pain in a large number of patients who had previously been diagnosed with IBS. (5) A five-year study by Constanza et al. of patients with recurrent chronic abdominal pain found IBS in 16.3% and CAWP in 7.8%. (6)
Carnett's sign was described in 1927 by J.B. Carnett, an English obstetrician. (7, 8) Immediately after he recognized its importance, he and his colleagues began to use it to diagnose what they called intercostal neuralgia. The name referred to radicular irritation of the last seven dorsal roots and/or the first lumbar root where the innervation of the anterior abdominal wall begins. This causes abdominal pain capable of simulating diseases such as appendicitis, renal or gallbladder alterations and alterations of the uterus and its annexes, but which actually corresponds to hypersensitivity of the abdominal wall. In the vast majority of cases it can be resolved by infiltration of the pain site with local anesthetics. (8, 9)
Colombian and international publications have shown that failure to identify this sign delays diagnosis and significantly increases costs due to requests for unnecessary examinations, and surgery that is not really indicated. (2, 5, 6, 9, 10)
Multiple examinations including abdominal ultrasound and CT scans are routinely performed on patients with this clinical picture and unnecessary surgical procedures such as appendectomies, cholecystectomies and diagnostic laparoscopy are all too often performed as well. All of these procedures represent unnecessary expenses for the health care system since they do not arrive at a correct diagnosis and the patient's quality of life continues to deteriorate. (1, 3, 5). Thompson et al. compared the average cost of evaluating patients with chronic abdominal pain, in whom abdominal wall pain was a diagnosis of exclusion, and found costs in excess of $6,000 per patient. These patients finally achieved remarkable improvement after infiltrating the abdominal wall with local anesthetics. (11) Also, Constanza et al. documented that the annual cost of each patient with chronic abdominal pain was approximately $11,000, compared to $540 per year when a diagnosis of chronic abdominal wall pain (CAWP) was made using Carnett's sign. (6)
The study mentioned above by Otero and colleagues reported a total of 1,168 pre-diagnosis consultations for CAWP, 278 procedures and 14 hospitalizations in a group of 91 patients. The total estimated cost was $18,000 (54 million COP) based on Colombian Social Security rates for 2001 with an average cost of $200 dollars (COP 594,500) per patient not including medications, laboratory tests, or lost work time. (2) Another study found that only 4% of physicians surveyed considered the abdominal wall as a source of chronic abdominal pain. (6)
In this article we reported the case of a patient who had suffered from CAWP for approximately two years before he was hospitalized during his most recent abdominal pain evaluation. The cost of hospitalization was approximately $ 1,000 (COP 3,000,000) which is equivalent to 80 days of salary of a worker with the minimum monthly income allowed by Colombian legislation. The pain was resolved with a procedure that took less than 10 minutes and cost no more than $15.00!
When physicians learn to identify this important sign and become familiar with it, the benefits are evident. (2, 6, 10)
The following steps can be used to identify Carnett's sign:
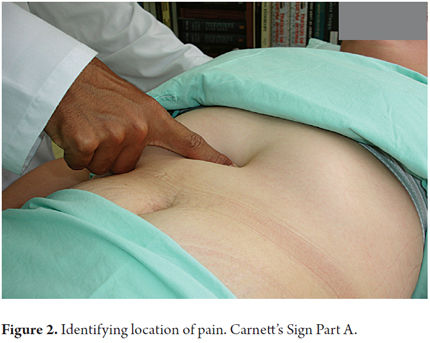
1. With the patient in the dorsal decubitus position press various points are along the outer edge of the anterior rectus muscles in search of a painful point.
2. The area of pain should not be greater than 1.5 cm2 (Figures 1 and 2).
3. Occasionally, there will be allodynia (Abnormal painful sensation when touched. Touch is a stimulus that normally does not produce pain). (1, 2, 8)
4. Once the site of pain has been identified, pressure is maintained with the finger (we prefer to do it with the thumb of the right hand).
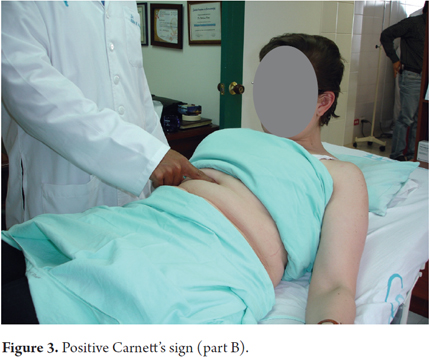
5. The patient is then asked to sit down slowly, which will tighten the abdominal muscles. When the abdominal muscles tighten the pain will remain unchanged or its intensity will increase.
6. This is the second part of Carnett's sign which indicates that the pain originates in the anterior cutaneous nerve (Figure 3).
7. If the pain disappears when the patient sits, it is considered to originate in the visceral structures.
The mechanism that causes pain originating in the wall to increase upon finger pressure at the site of pain is a contraction of the anterior rectus muscles. If the pain originates in visceral structures, the contracted muscle protects them from the finger pressure, and the pain disappears. (2, 8) Other ways to tighten the abdominal muscles are for the patient to raise her or his lower limbs or to cough. In either case, the finger should be kept on the site of pain. This last method is a modification that we have made to the original description.
Positive identification of the pain point with the characteristics mentioned has a sensitivity of 88% and a specificity of 97%. (12)
In our service, the infiltration protocol is as follows:
1. Initially the pain site is identified.
2. Once found, it is marked by a cross with a spheroid (Figure 4). (2)
3. It is then cleansed with alcohol and infiltrated with 1-2 mL of 2% lidocaine without epinephrine. (2)
4. The needle used depends on the thickness of the panniculus adiposus, an insulin needle (half inch 27-gauge) is chosen for thin persons, and a 1-inch 23-gauge needle or a 1.5-inch 21-gauge needle (conventional needle supplied with syringes) for other people.
5. The needles mentioned are mounted in a 5-10 mL syringe (Figures 5, 6 and 7).

Several points can be infiltrated in a single session. Our recommendation is that not more than 10 mL should be infiltrated in one session, given the risk of adverse cardiovascular events. The patient must always sign a specific informed consent form for this procedure. If the patient is a minor, consent must be signed by either one of the parents or by a legal representative. The goal of infiltration is to reach the anterior cutaneous nerve or its vicinity. (2) After one injection, the pain disappears in more than 80% of patients. With two or more injections, pain disappears in up to 91% of patients. (2) Ineffectiveness of treatment with local anesthetic may be due to several factors such as difficulty in reaching the site of pain, obesity, short needles, poor technique or incorrect diagnosis. (1)
In the presence of a painful condition with the characteristics mentioned, no other confirmation tests are necessary. A recent clinical trial has shown that lidocaine infiltration of the pain site is more efficacious than saline infiltration used as a placebo (p = 0.007). (11)
It has also been documented that for patients with chronic pelvic pain who have Carnett's sign, weekly infiltration of the abdominal wall with 1% lidocaine + epinephrine for 5 to 6 weeks leads to the disappearance of pain in 77% of patients and improvement in 93% of patients. (13) These results highlight the importance of detecting Carnett's sign in this type of patients and that infiltration of the pain site can be an effective procedure in gynecology and obstetrics. (11) This pathology has also been found in children and this treatment has been shown to be effective for them as well. (10)
Despite proven improvement of pain following infiltration with lidocaine, it has been found that chronic stress, psychological alterations and concomitant psychiatric diseases may predict less favorable responses to treatment even when the patient has Carnett's sign. (14, 15) These specific cases are influenced by somatization syndromes or by psychosomatic problems that require a multidisciplinary approach. (14, 15)
Traditionally, Carnett's sign has been used in the evaluation of patients with chronic abdominal pain; However, it has also proven useful in patients with acute abdominal pain. (16, 17) In the Thomson study, only one out of 24 patients with Carnett's sign had a visceral cause of acute pain, and Gray et al. found appendicitis in five of 158 (3.1%) patients with the sign. (17) When there is acute abdomen and peritonitis, this sign has no utility. (18)
In cases of intractable pain due to nerve entrapment, local surgery has been the treatment of choice. (19) In such cases, anterior neurectomy of a section of the cutaneous nerve is performed with ligation of the accompanying vascular package. Other pathologies, such as herniated dorsal vertebrae (75% below T7), may be causes of chronic abdominal wall pain, but the prevalence is considered to be low. However, a study by Lara et al. found a prevalence of thoracic disc hernia in up to 30% of a small group of patients with chronic abdominal pain and Carnett's sign. Nevertheless, almost 90% of the patients in this study reported constant abdominal pain associated with back pain, which was exacerbated with exertion. The most common location was towards the flanks, which could help guide those cases of chronic abdominal pain that do not improve with infiltration of anesthetics and that may require a study with dorsal spine MRI. (13)
The origin of alterations of the anterior cutaneous nerve can often not be determined. However, various circumstances of everyday life can cause damage. Events such as chronic coughing, abdominal trauma, tight clothing, recurrent vomiting, abdominal distension, or repetitive movements that cause increased abdominal pressure may lead to injury of the anterior cutaneous nerve and will result in chronic abdominal pain. (13) Other causes are entrapment of the anterior cutaneous nerve of the abdomen (ACNES), caused by increased abdominal pressure (2, 8, 10), surgical scarring, hematomas of the rectus sheath or incisional hernias. (18, 19)
CONCLUSION
As in all medical situations, a detailed medical history and a complete physical examination are essential for patients with chronic abdominal pain. You cannot replace them with technology since exploration of clinical signs such as Carnett's sign is fundamental for ruling out a large number of differential diagnoses and for avoiding many cumbersome and unsuccessful additional procedures that waste the funds of the health care system without identifying or resolving the illness. (1, 2, 6, 11, 20, 21)
Financing
The costs of this study were assumed entirely by the authors.
Conflicts of interests
Dr. Otero has lectured and received fees from Abbott-Lafrancol, Tecnofarma, La-Santé laboratories, Procaps and Takeda laboratories. Dr. Erika Martínez and Dr. Adán Lúquez had no conflicts of interests.
Acknowledgements
The authors thank Alejandra Figueroa, assistant nurse, and Liliana Oino, biomedical engineer, for their interest in the follow-up and assignment of appointments of patients with this pathology in the Gastroenterology Unit of Clínica Fundadores.
REFERENCES
1. Koop H, Koprdova S, Schürman C. Chronic abdominal wall pain. Dtsch Arztebl Int. 2016;113(4):51-7. [ Links ]
2. Otero W, Ruiz X, Otero E, et al. Dolor de la pared abdominal: una entidad olvidada con gran impacto en la práctica médica. Rev Col Gastroenterol. 2007;22:261-71. [ Links ]
3. Tolba R, Shroll J, Kanu A, et al. The epidemiology of chronic abdominal pain. En: Kapural L. Chronic abdominal pain. An evidence-based, comprehensive guide to clinical management. New York: Springer Science-Business Media; 2015. p. 13-24. [ Links ]
4. Lidsetmo RO, Stulberg J. Chronic abdominal wall painA diagnostic challenge for the surgeon. Am J Surg. 2009;198:129-34. [ Links ]
5. Van Assen T, de Jager-Kievit JW, Scheltinga MR, et al. Chronic abdominal wall pain misdiagnosed as functional abdominal pain. J Am Board Fam Med. 2014;26(6):738-44. [ Links ]
6. Constanza CD, Longstreth GF, Liu AL. Chronic abdominal wall pain: clinical feature, health care costs and long term outcome. Clin Gastroenterol Hepatol. 2004;2(5):395-99. [ Links ]
7. Carnett JB. Intercostal neuralgia as a cause of abdominal pain and tenderness. Surg Gynecol Obstet. 1926;42:625-32. [ Links ]
8. Carnett JB, Bates W. The treatment of intercostal neuralgia of the abdominal wall. Ann Surg. 1933;98(5):820-9. [ Links ]
9. Thomson WHF, Dawes RFH, Carter SSC. Abdominal wall tenderness: a useful sign in chronic abdominal pain. Br J Sur. 1991;78(2):223-5. [ Links ]
10. Akhnikh S, De Korte N, De Winter P. Anterior cutaneous nerve entrapment syndrome (ACNES): The forgotten diagnosis. Eur J Pediatrics. 2014;173:445-9. [ Links ]
11. Thomson C, Goodman R, Rowe WA, et al. Abdominal wall syndrome: a costly diagnosis of exclusion. Gastroenterology. 2001;120(5):637A. [ Links ]
12. Takada T, Ikusaka M, Ohira Y, et al. Diagnostic usefulness of carnetts test in psychogenic abdominal pain. Int Med. 2011;50(3):213-7. [ Links ]
13. Boelens OBA, Scheltinga MF, Houterman S, et al. Randomized clinical trials on trigger point infiltration with lidocaine to diagnose anterior cutaneous nerve entrapment syndrome. Br J Surg. 2013;100:217-21. [ Links ]
14. Lara FJ, Berges AF, Quesada JQ, et al. Thoracic disk herniation, a not infrequent cause of chronic abdominal pain. Int Surg. 2012;97(1):27-33. [ Links ]
15. Feurle GE. Abdominal wall pain--classification, diagnosis and treatment suggestions. Wien Klin Wocht. 2007;119(21-22):633-8. [ Links ]
16. Thomson H, Francis DMA. Abdominal-wall tenderness: a useful sign in the acute abdomen. Lancet. 1977;310(8047):1053-4. [ Links ]
17. Gray DW, Seabrook G, Dixon JM, et al. Is abdominal wall tenderness a useful sign in the diagnosis of non-specific abdominal pain? Ann R Coll Surg Engl. 1988;70:233-4. [ Links ]
18. Rivero M, Moreira V, Riesco JM, et al. Dolor originado en la pared abdominal: una alternativa diagnóstica olvidada. Gastroenterol Hepatol. 2007;30(4):244-50. [ Links ]
19. van Assen T, Boelens OB, van Eerten PV. Long term success rate after an anterior neurectomy in patients with abdominal nerve entrapment syndrome. Surgery. 2015;157:137-43. [ Links ]
20. Alas A, Kim DS, Ogunyemi DAA. Do trigger point injections with buffered lidocaine improve pelvic pain of myofascial origin - a retrospective study. J Min Inv Gynecol. 2012;19(Suppl.1):S28-32. [ Links ]
21. Abdominal wall tenderness test: could Carnett cut costs? Lancet. 1991;337 (8750):1134. [ Links ]

