










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.33 no.1 Bogotá Jan./Mar. 2018
https://doi.org/10.22516/25007440.231
Review articles
Literature Review of Management of Colorectal Foreign Bodies
1Coloproctólogo del Hospital Militar Central. Bogotá D. C., Colombia.
2Fellow de coloproctología de la Universidad Militar Nueva Granada. Bogotá D. C., Colombia.
3Residente de cirugía general, Universidad Nacional de Colombia. Bogotá D. C., Colombia.
4Fellow de cirugía gastrointestinal y endoscopia digestiva del Instituto Nacional de Cancerología. Bogotá D. C., Colombia.
Patients with foreign bodies in their rectums are not uncommon, but statistics on the epidemiology of this entity are scarce. Most of the literature published consists of case reports or case series. Foreign rectal bodies, whether inserted intentionally or unintentionally, constitute a diagnostic and therapeutic challenge for physicians who need skill and knowledge to extract objects of different shapes and sizes.
Foreign rectal bodies are generally observed in the adult population in relation to erotic stimulation or sexual assault. Occasionally, foreign bodies are ingested and pass through the gastrointestinal tract to lodge in the rectum. Although this situation is the least common, it does occur, especially in patients with mental illnesses, visual disorders, or alcoholism and among users of dental prostheses. The purpose of this review is to establish management guidelines and to present an algorithm for the approach to colorectal foreign bodies.
Keywords: Diseases of the rectum; colon; foreign body
La presentación de pacientes con cuerpos extraños a nivel rectal no es poco frecuente; sin embargo, hay pocas estadísticas sobre la epidemiología de esta entidad. La mayor parte de la literatura publicada hace mención a reporte de casos o series de casos. Los cuerpos extraños rectales son insertados de forma intencional o no intencional, y constituyen un reto diagnóstico y terapéutico para el médico; por lo que el médico a cargo requiere de la habilidad y conocimiento para extraer objetos de diferentes formas y tamaños. Los cuerpos extraños rectales son generalmente observados en la población adulta; en relación con la estimulación erótica o asalto sexual. Adicionalmente, algunos cuerpos extraños pueden ser ingeridos ocasionalmente, pasando a través del tracto gastrointestinal y alojándose en el recto, aunque esta situación es la menos común; en especial en pacientes con enfermedades mentales, trastornos visuales, alcohólicos o usuarios de prótesis dentales. La finalidad de esta revisión es establecer unas pautas de manejo y dar a conocer un algoritmo para el enfoque de los cuerpos extraños colorrectales.
Palabras clave: Enfermedades del recto; colon; cuerpo extraño
Literature and history of colorectal foreign bodies
An article by Haft and Benjamin 1 about the psychosocial aspects of rectal foreign bodies says that the oldest cases date from Ancient Greece and Ancient Egypt, but the oldest case reported in a medical journal was published in 1919 by Smiley. Some articles about proctology in medical books, such as that published by Gant in 1902, give reasons for the literature about foreign bodies while others like the one published by Poulet in 1881 are surgical treatises. The number of articles describing foreign bodies have increased over time, from less than 30 articles published in the literature before 1950 to 66 articles from 2000 to 2015. The current incidence of foreign bodies is unknown. Traditionally, a greater incidence has been described among men than among women, but there is no relationship of sexual orientation with rectal foreign bodies despite uncritical and arbitrary information from the 1970s to the 1990s which associated rectal foreign bodies with the homosexual population. 2. The greatest lapse of time between insertion of a foreign body and diagnosis documented in the literature is 5 years. 3
Epidemiology and etiology
There is a clear preponderance of the male sex, with a relationship that can reach 28 men to each woman, and the predominance of cases occurs in the age group between 20 and 40 years. 4 Most rectally retained foreign bodies are those that have been inserted for the purpose of erotic stimulation and gratification. This accounts for as many as 75% of cases while sexual assault accounts for another 12.5% of cases. There are some isolated reports of cases of rectal foreign body retention in elderly patients (60 to 80 years old) resulting from self-treatment of fecal impaction or prostatic massage. Other cases involve patients institutionalized as prisoners or psychiatric patients who lodge knives, illicit drugs or weapons in their rectums in order to injure their caregivers, guards, or other patients or prisoners. 5 Foreign bodies are rare in children and are usually related to sexual abuse, so they should be investigated. Almost any object can be found including sex toys, bottles, light bulbs, metal and wooden objects, fruit, vegetables, batteries, aerosols, and caps.
A retrospective study which included 648 patients from 431 hospitals in Japan from 2007 to 2010 found that 15 patients had more than one hospital admission for this cause (2.3%) with a maximum of 4 readmissions. . The number of male patients was 526 (81.1%), with a male-female ratio of 4.3 to 1. Male patients’ age range was 60 to 69, and female patients were between 80 and 89 years of age. There was an association of major mental pathology in women with respect to men (8.2% versus 2.7% in men).
The overall mortality rate was 1.2%. Of the 44 patients with perforations and peritonitis, one of the cases was iatrogenic. For the female group, 4.8% died, 12.8% had perforations and/or peritonitis and 4% developed sepsis. Male patients were more likely to have foreign bodies extracted anally than abdominally. About 73% of the patients received general or regional anesthesia. 6
A multivariate logistic regression analysis found that female patients have twice the chance of poor outcomes such as anal or rectal abscesses, perforations, sepsis and peritonitis as do men. Perforations due to ingestion of foreign bodies can account for as much as 25% of the objects found in the rectum or the anus. 7
Similarly, there is an unclear relationship between foreign bodies found in the rectal area and human immunodeficiency virus (HIV) infections. In Japan, the prevalence of HIV infections in the general population is 0.018%, but the study found a prevalence of 1.1% which indicates the importance of HIV blood tests for this population group, taking into account that they are currently only performed in 10% of this subpopulation. 6
Classification and types
Foreign bodies can be classified in different ways. Depending on their location, they can be found in the upper gastrointestinal tract, defined as the small intestine, where they are usually ingested and impact in the anatomically narrowest areas. When these bodies manage to pass to the colon, they are classified as from the lower gastrointestinal tract and can be retained either in the colon or the rectum. For bodies introduced through the rectum, several anatomical characteristics must be considered including the internal and external anal sphincters which contract tonically. Foreign bodies may produce edema in these sphincters after insertion. Also, the natural curvature at the rectosigmoid junction can cause difficulty for spontaneous passage and elimination. 8 For practical management purposes, it has been proposed that the location of the foreign body be designated above or below this junction.
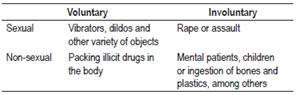
Foreign bodies are also described as either voluntary or involuntary and as sexual versus or non-sexual (Table 1). 9 This is important because it gives an orientation about the type of trauma the patient may have suffered which is intimately related to the object. The great variety of sizes and shapes broadens the spectrum of injuries as well as possible extraction techniques. 10 The literature includes reports of vibrators, dildos, cucumbers, apples, light bulbs, glass bottles, plastic bottles, bones and assorted other objects.
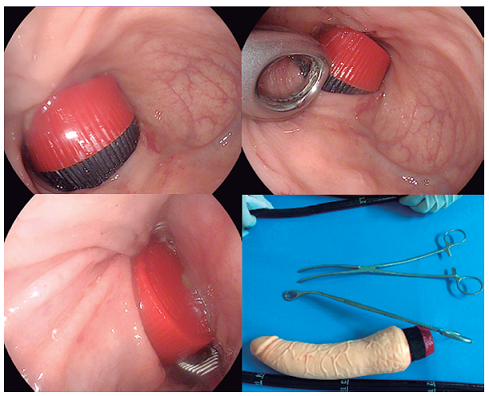
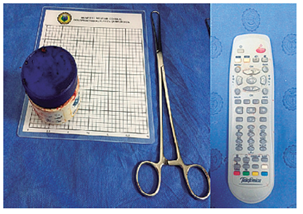
One characteristic that can be used to classify foreign bodies is whether or not they are easy to grip. Easy-to-grip objects include small sharp items like bones as well as phallic elements such as dildos, vibrators, candles, vegetables and fruit (Figure 1). On the other hand, difficult-to-grip objects include containers, bottles, jars, spheres, and light bulbs (Figure 2).
It is also important to classify rectal trauma using the rectal organ injury scale of the American Association for Trauma Surgery (AAST) to define management.
Clinical picture
Diagnosis can be difficult due to patient embarrassment which can lead them to visit the emergency services late. 1,11,12 It is important to obtain accurate information about the item introduced, although it may be difficult for the patient to provide this information.
In the clinical history, the cardinal symptom is anal pain or constipation. Other symptoms include bleeding, inability to urinate, abdominal pain in the lower quadrants, anal incontinence, diarrhea, multiple unsuccessful attempts to remove the foreign body, and sepsis in cases of perforation (hypotension, tachycardia and peritoneal irritation). In addition, cardiovascular collapse sometimes occurs in patients who are used for trafficking psychoactive substances which rupture inside of the patient. Information will also be difficult to obtain from this type of patient. 12,13
The length of time the object has been retained in the anorectal region is directly related to the risk of rupture and injury of the mucosa.
Physical examination
The physician must maintain the patient’s privacy, completely avoid comical and/or discriminatory comments, and protect the privacy of the patient from curious care personnel who are unrelated to the case. 10
The main objective of the initial evaluation is to identify the type, number, size, shape and location of the foreign body or bodies. 10 The importance of a detailed description of the object is fundamental for establishing the best management option. Nevertheless, a good approach by the examining physician is required to achieve this description. In addition to avoiding judgment, the medical staff must be respectful and gentle in order to establish an appropriate relationship based on trust. It is essential to give a clear explanation to achieve accurate communication and convince the patience that providing the relevant information about the mechanism and type of object is important for the patient him/herself. 14
A careful, detailed examination must be performed including abdominal auscultation to determine if peristalsis is present, absent, decreased, or increased. One of the purposes of this evaluation is to rule out peritoneal irritation. In some cases, foreign bodies can be felt and in the perineal area. Findings such as lacerations, bruises, perforations, bleeding, bad odors, discharges of mucous and bloody secretions should be clearly described. If there is any outflow of mucous with a fetid chocolate appearance, it suggests necrosis, perforation or sepsis. 15
When a digital rectal examination is performed, care must be taken when the finger is inserted since some objects may be sharp or pointed which poses the danger of biological accident to the examining physician. The state of the anal sphincter including tone must be detailed, and an evaluation must be done before and after the removal of the foreign body. Involuntary spasms may occur during an extraction attempt. This information is highly relevant and should be clearly stated in the clinical history.
In patients whose sphincters are not injured, the tone should be tighter as a result of muscle spasm secondary to the object. The foreign body can be directly palpated. If the object is not palpated, findings such as leakage of blood or loss of sphincter tone can suggest the presence of a foreign body. 9,16 If a perforation occurs above the superior rectus, the patient may have clinical signs of peritonitis.
When findings from digital rectal examination are negative, and when visualization is needed, anoscopy can be used. Its limitation lies in its diameter, but it allows identification of the exact nature and position of the object.
In case of any doubt regarding the integrity of the anorectal mucosa, it should be directly evaluated.
Diagnostic studies
Abdominal radiographs (Rx) are the first examinations to be done. They allow location of the object, estimation of its size and determination of the quantity of objects. Anteroposterior and lateral radiography is required for more exact location of an object as shown in Figures 3 and 4. Objects such as metal or gravel are denser than the surrounding tissues and can be seen well in x-rays, but organic materials that have a density similar to human tissues may not be observed. 9. Failure to observe a foreign body in an x-ray does not rule out the its presence.


A standing chest X-ray should be taken of all patients for whom peritoneal perforation is suspected.
If an object cannot be seen in an x-ray, colonoscopy, CT scans of the abdomen and pelvis, and contrast x-rays using water-soluble medium can be used, taking care that hydrostatic pressure does not increase enough to perforate the wall.
Blood tests for inflammatory parameters such as C-reactive protein (CRP) and the erythrocyte sedimentation rate are not routine initial examinations, but they can be used when perforation is suspected. The use of arterial gases to determine acidosis in septic patients has been described. In cases of suspected poisoning, toxicological screening should be performed. 10
Endoscopic ultrasonography has been described as a diagnostic method for impacted foreign bodies that generate lesions similar to subepithelial ones. Granulomas with a foreign body inside have been document ed. 17
Contrast tomography of the abdomen and pelvis is indicated when perforation is suspected below peritoneal reflection. When extraperitoneal perforation of the rectum is suspected, thinning of the rectal wall, mesorectal air, perirectal fluid and striation of mesorectal fat can be seen.
Endoscopy provides excellent visualization of the segments evaluated and allows diagnosis and extraction of objects. It requires insufflation to block valve phenomenon produced when the object is attached to the mucosa. It is necessary to perform flexible rectosigmoidoscopy after extraction to rule out lesions of the colon or rectum, and to determine whether the patient has introduced any additional objects. 8,10
Techniques
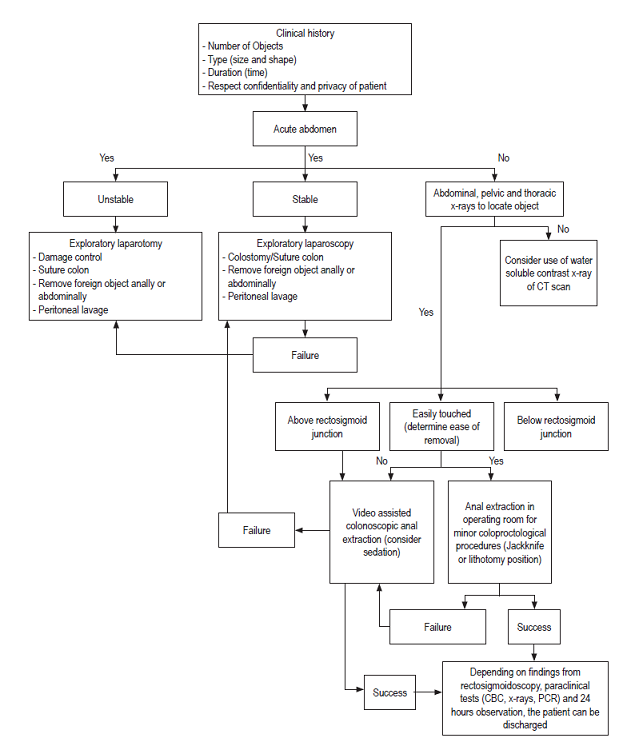
In patients with acute abdomen in whom perforation is suspected, vigorous parenteral hydration, initiation of broad-spectrum antibiotics, bladder catheter, and decompressing nasogastric tube are indicated together with exploratory laparotomy.
One important issue to take into account prior to extraction is patient relaxation. If your patient is calm and relaxed, you can attempt the procedure without anesthesia. Otherwise, it can be performed with local anesthesia, but this produces blockage of the perianal nerves. This leads to conscious sedation, spinal anesthesia and ultimately to general anesthesia to achieve relaxation, elimination of sphincter spasm and improvement of visualization and exposure.
For local anesthesia, lidocaine with 1% epinephrine or 0.5% or with a mixture of both at a one to one ratio may be used. An initial superficial block is made, then an intersynthetic circumferential block is made, and then the pudendal nerve is blocked. This is achieved by infiltrating the deep tissues in the bilateral posterolateral area at 1 cm medial of the ischial tuberosity. Once this has been done, digital dilation should proceed gently.
It is not recommended to blindly remove objects that may have high risks of injuring the rectum, causing a rupture or fragmentation. Examples include any object with sharp edge, light bulbs and crystal glasses.
Extraction with the patient in the same bed in which the evaluation is done reportedly has had success rates between 60% and 75%, but a high failure rate has been reported for anal extractions as well as for pushing objects towards the rectosigmoid region.
The procedure begins in the emergency service with initial evaluation during which small objects can be grasped and removed. For patients who do not have peritoneal irritation, the finger should be properly lubricated with lidocaine jelly, and abdominal pressure should be applied to achieve distal mobilization of the object. Pushing the object towards the proximal rectum must be avoided.
Factors that indicate likely failure of extraction include objects that are more than 10 cm long, hard objects, sharp objects, objects that migrate and objects that have been retained for two or more days. 12
Anoscopy performed for easily grasped objects should follow these recommendations:
Object(s) should be removed with either a Kelly or Rochester clamp.
Procedure can be done without anesthesia or with local anesthesia.
Patient should be in the Kraske (pocketknife) position
Avoid lacerations of the mucosa.
Anoscopy performed for difficult-to-grasp objects should follow these recommendations:
Object(s) should be removed with either a Foerster clamp or foreign body clamp.
Procedure should be done with local or regional anesthesia.
An anoscope, Pratt anal separator and/or rigid rectoscope should be used with colonoscopy to view the object.
Patient should be in the lithotomy or lateral position
Abdominal pressure on hypogastrium.
Care should be taken with non-cooperative or anxious patients for whom pain is associated with anal sphincter spasm. This can limit attempts to with draw an object in the emergency services.
In case anal extraction fails, there are two minimally invasive approaches before an abdominal examination: flexible sigmoidoscopy and minimally invasive transanal surgery. The latter has three advantages: many surgeons can use it because they are accustomed to the use of laparoscopy, the magnified image of the object helps define the state of the mucosa, and specialized instruments are not required. 18,19
When digital extraction fails, an anoscope or a vaginal speculum can be used to visualize the object, and a Foerster clamp can be used for extraction. On some occasions, the mucous can adhere so firmly to the object that a vacuum is created that prevents the object from being extracted. A Foley catheter can be passed behind the object with insufflation of air in order to release the vacuum, and this can be followed with balloon insufflation to allow removal of the object with subtle traction. 20
A key advantage of spinal blocks and general anesthesia is that they reduce anal sphincter tone and inhibit spasming which improves visualization of the object and substantially increases the possibility of anal removal. 21
Various techniques for extracting foreign bodies have been proposed in the literature, and they use a variety of different instruments including polypectomy forceps, Foley catheters, obstetric forceps, vacuum extractors, dilatation balloons, plastic cylinders and vaginal spatulas.
When manual extraction, extraction under anesthesia, minimally invasive transanal surgery and flexible sigmoidoscopy fail, surgical intervention becomes necessary. The laparoscopic approach is considered to be the first option. Instruments of minimally invasive surgery can be manipulated transmurally to push the object distally. Open surgery is reserved for cases of low rectal perforations, severe contamination of the peritoneal cavity, and when there is no experience with laparoscopy.
When there are mucosal lacerations, edema or erosions, the patient should be kept in the hospital for observation (Figure 5).
Complications
The most important and relevant complications are those listed below, some of which have been mentioned above:
Acute, subacute and chronic perforations occur especially in cases of sharp objects. Narrow zones, sharp angles, flange zones, and cul-de-sacs are the places where the greatest number of perforations occur: 75% are in the ileocecal area. 22
Intramural, intrahepatic, subphrenic and abdominal abscesses.
Gastrointestinal, urinary tract and enterocutaneous fistulas.
Migration of the object to neighboring organs. 23
Intestinal obstructions due to impaction occur in areas such as the ileocecal valve, cecum, appendix and anus. 24
Digestive hemorrhaging due to erosion of the digestive tract wall.
Poisoning due to absorption of degraded material.
Sepsis.
Multiple organic dysfunction syndrome.
Psychological disorders in cases of sexual aggression.
Death secondary to sepsis and multiple organ dysfunction. (9,25)
REFERENCES
1. Ayantunde AA, Oke T. A review of gastrointestinal foreign bodies. Int J Clin Pract. 2006;60(6):735-9. https://doi.org/10.1111/j.1368-5031.2006.00709.x. [ Links ]
2. Desai B. Visual diagnosis: Rectal foreign body: A primer for emergency physicians. Int J Emerg Med. 2011;4:73. https://doi.org/10.1186/1865-1380-4-73. [ Links ]
3. Ozbilgin M, Arslan B, Yakut MC, et al. Five years with a rectal foreign body: A case report. Int J Surg Case Rep. 2015;6C:210-3. https://doi.org/10.1016/j.ijscr.2014.11.053. [ Links ]
4. Clarke DL, Buccimazza I, Anderson FA, et al. Colorectal foreign bodies. Colorectal Dis. 2005;7(1):98-103. https://doi.org/10.1111/j.1463-1318.2004.00699.x. [ Links ]
5. Stack LB, Munter DW. Foreign bodies in the gastrointestinal tract. Emerg Med Clin North Am. 1996;14(3):493-521. https://doi.org/10.1016/S0733-8627(05)70264-9. [ Links ]
6. Odagiri H, Yasunaga H, Matsui H, et al. Difference in outcomes of rectal foreign bodies between males and females: a retrospective analysis of a national inpatient database in Japan. Digestion. 2015;92(3):165-70. https://doi.org/10.1159/000439125. [ Links ]
7. Rodríguez-Hermosa JI, Codina-Cazador A, Sirvent JM, et al. Surgically treated perforations of the gastrointestinal tract caused by ingested foreign bodies. Colorectal Dis. 2008;10(7):701-7. https://doi.org/10.1111/j.1463-1318.2007.01401.x. [ Links ]
8. Smith MT, Wong RK. Foreign bodies. Gastrointest Endosc Clin N Am. 2007;17(2):361-82, vii. https://doi.org/10.1016/j.giec.2007.03.002. [ Links ]
9. Goldberg JE, Steele SR. Rectal foreign bodies. Surg Clin North Am. 2010;90(1):173-84. https://doi.org/10.1016/j.suc.2009.10.004. [ Links ]
10. Ayantunde AA. Approach to the diagnosis and management of retained rectal foreign bodies: clinical update. Tech Coloproctol. 2013;17(1):13-20. https://doi.org/10.1007/s10151-012-0899-1. [ Links ]
11. Cohen JS, Sackier JM. Management of colorectal foreign bodies. J R Coll Surg Edinb. 1996;41(5):312-5. [ Links ]
12. Lake JP, Essani R, Petrone P, et al. Management of retained colorectal foreign bodies: predictors of operative intervention. Dis Colon Rectum. 2004;47(10):1694-8. https://doi.org/10.1007/s10350-004-0676-4. [ Links ]
13. Huang WC, Jiang JK, Wang HS, et al. Retained rectal foreign bodies. J Chin Med Assoc. 2003;66(10):607-12. [ Links ]
14. Cawich SO, Thomas DA, Mohammed F, et al. A management algorithm for retained rectal foreign bodies. Am J Mens Health. 2017;11(3):684-692. https://doi.org/10.1177/1557988316680929. [ Links ]
15. Fry RD. Anorectal trauma and foreign bodies. Surg Clin North Am. 1994;74(6):1491-505. https://doi.org/10.1016/S0039-6109(16)46494-7. [ Links ]
16. Tatar C, Karşıdağ T, Hut A. Successful endoscopic removal of a foreign body in the rectum. Turk J Gastroenterol. 2014;25(4):442-3. https://doi.org/10.5152/tjg.2014.5136. [ Links ]
17. Rodrigues FG, Campos JB, Silva GD, et al. Endoscopic ultrasound in the diagnosis of foreign bodies of the colon and rectum. Rev Assoc Med Bras (1992). 2016;62(9):818-21. https://doi.org/10.1590/1806-9282.62.09.818. [ Links ]
18. Bak Y, Merriam M, Neff M, et al. Novel approach to rectal foreign body extraction. JSLS. 2013;17(2):342-5. https://doi.org/10.4293/108680813X13654754534233. [ Links ]
19. Cawich SO, Mohammed F, Spence R, et al. Colonic foreign body retrieval using a modified TAMIS technique with standard instruments and trocars. Case Rep Emerg Med. 2015;2015:815616. https://doi.org/10.1155/2015/815616. [ Links ]
20. Ayantunde AA, Unluer Z. Increasing trend in retained rectal foreign bodies. World J Gastrointest Surg. 2016;8(10):679-84. https://doi.org/10.4240/wjgs.v8.i10.679. [ Links ]
21. Cirocco WC. Anesthesia facilitates the extraction of rectal foreign bodies. Gastrointest Endosc. 2000;52(3):452-3. https://doi.org/10.1067/mge.2000.108045. [ Links ]
22. Flint LM, Vitale GC, Richardson JD, et al. The injured colon: relationships of management to complications. Ann Surg. 1981;193(5):619-23. https://doi.org/10.1097/00000658-198105000-00012. [ Links ]
23. Chiu WK, Hsiao CW, Kang JC, et al. Intrapelvic migration with long-term retention of a rectal thermometer: a case report. Clin Pediatr (Phila). 2007;46(7):636-8. https://doi.org/10.1177/0009922807300701. [ Links ]
24. Hoare D, Akbar F, Maw A. Comment on ‘Colorectal foreign bodies: a systematic review’. Colorectal Dis. 2011;13(1):108. https://doi.org/10.1111/j.1463-1318.2010.02503.x. [ Links ]
25. Kurer MA, Davey C, Khan S, et al. Colorectal foreign bodies: a systematic review. Colorectal Dis. 2010;12(9):851-61. https://doi.org/10.1111/j.1463-1318.2009.02109.x. [ Links ]
Received: July 08, 2017; Accepted: January 22, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
