










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957
Rev Col Gastroenterol vol.33 no.3 Bogotá jul./set. 2018
https://doi.org/10.22516/25007440.201
Originals articles
Real-time shearwave elastography (SSWE) in a cohort of patients with cirrhosis at a medical center in Bogotá
1Centro de Enfermedades Hepáticas y Digestivas (CEHYD), Bogotá, Colombia.
2Hospital Universitario Nacional de Colombia, grupo Equidad en Salud, Facultad de Medicina, Universidad Nacional de Colombia, Bogotá
3Universidad Industrial de Santander, Bucaramanga, Colombia
Introduction:
Cirrhosis, understood as a dynamic and reversible process, is the final result of chronically progressive liver diseases of various etiologies. Non-invasive methods based on ultrasound have gradually become useful diagnostic tools for studying liver diseases. Real-time supersonic shearwave elastography (SSWE) study of these patients has recently been introduced to Colombia.
Objective:
The objective of this study was to evaluate real-time SSWE in patients with cirrhosis at a center for the treatment of liver and digestive diseases in Bogotá.
Materials and Methods:
This is a retrospective pilot study of a cohort of cirrhotic patients with diagnoses confirmed by liver biopsies, imaging, clinical indicators or a combination of these.
Results:
Sixty-five patients who had been diagnosed with cirrhosis were included in this study. The median age was 58 years, 61.5% were women, and 38.5% were men. We found that median hepatic stiffness was 16.6 kilopascals (kPs), the interquartile range was 13.9 -19.5, the minimum value was 12, and the maximum value was 30.5. There were no statistically significant differences between women and men, within groups and with and without biopsies (p = 0.64 and p = 0.26 respectively).
Conclusions:
Hepatic rigidity measurements for cirrhotic patients analyzed in this pilot study were within the ranges reported in initial international tests, so this non-invasive test should be considered for patients suspected of having cirrhosis as a way to avoid complications of liver biopsies.
Keywords: Real-time elastography; supersonic; liver fibrosis; cirrhosis
Introducción:
la cirrosis, entendida como un proceso dinámico y reversible, es el resultado final de las enfermedades hepáticas crónicamente progresivas de diferentes etiologías. Los métodos no invasivos basados en ecografía se han convertido paulatinamente en una herramienta diagnóstica útil en el estudio de las hepatopatías. Dentro de estos métodos, la elastografía en tiempo real, o Supersonic, de reciente introducción en nuestro medio, nos permite estudiar estos pacientes.
Objetivo:
evaluar el comportamiento de la elastografía en tiempo real en pacientes con cirrosis en un centro de atención de enfermedades hepáticas y digestivas en la ciudad de Bogotá.
Materiales y métodos:
estudio piloto retrospectivo de una cohorte con pacientes cirróticos con diagnóstico comprobado por biopsia hepática, imágenes, clínica o una combinación de estas.
Resultados:
se incluyeron 65 pacientes diagnosticados con cirrosis, la mediana de edad fue 58 años, 61,5% mujer y 38,5% hombre. Se encontró una mediana de rigidez hepática de 16,6 kilopascal (kPs) (RIQ de 13,9-19,5), con valor mínimo de 12 y un máximo de 30,5; sin una diferencia estadísticamente significativa entre mujeres y hombres dentro de los grupos con y sin biopsia (p = 0,64 y p = 0,26, respectivamente).
Conclusión:
los valores de la rigidez hepática de los pacientes cirróticos analizados en este estudio piloto se encontraron dentro de los reportados en los estudios iniciales de las pruebas a nivel internacional, por lo que se podría sugerir la realización de esta prueba no invasiva en pacientes con sospecha de cirrosis, evitando así las complicaciones de la biopsia hepática.
Palabras clave: Elastografía en tiempo real; Supersonic; fibrosis hepática; cirrosis
Introduction
Cirrhosis is the final result of chronic and progressive liver diseases of various etiologies. 1 Pathophysiologically, cirrhosis is the result of a process of continuous necrosis of hepatocytes with loss of liver parenchyma, inflammation, fibrogenesis, changes in cell regeneration and alterations of macrocirculation and microcirculation. This leads to distortion of the hepatic architecture and formation of regenerative nodules.2,3,4 Consequently, cirrhosis is understood as a dynamic process that is reversible at some points. In recent years, research to acquire new tools and information to guide proper diagnosis, management and approaches to this pathology has been encouraged.5,6,7
Classically, the definitive diagnosis of cirrhosis was established by the cirrhotic liver explant from liver transplantation surgery when observation of the surface of the liver from the biopsy clearly shows nodules of regeneration separated by fibrous septa. Recently non-invasive methods based on ultrasound, including real-time Supersonic Shear Wave Elastography (SSWE).1,8,9 SSWE is an elastography technique that can map and measure liver stiffness (LS) by using special software with an ultrasound system. The Aixplorer®, provides a two-dimensional, quantitative color image of liver tissue stiffness in real time. 10 On some occasions, SSWE can replace taking a liver biopsy and is useful for follow-up on the majority of patients with hepatopathy. 11,12,13,14
In Colombia, the test has been introduced recently, and studies of its behavior in patients diagnosed with cirrhosis are not known at this time. Therefore, the objective of this study was to evaluate the behavior of elastography in real time in patients with cirrhosis in a center for the treatment of liver and digestive diseases in the city of Bogotá.
Materials and methods
This is a retrospective pilot study of a cohort of patients with diagnoses of cirrhosis proven by liver biopsies, images, clinical examination or a combination of these. A review of patients’ clinical histories and use of SSWE were conducted at a center in Bogotá between June 1 and December 31, 2016. Verbal consent was obtained from subjects included. The inclusion criteria were:
Physical examination compatible with cirrhosis: stigmas of chronic liver disease, nevus of the skin or hard liver on palpation.
Images compatible with cirrhosis.
Liver biopsy compatible with cirrhosis or stage 4 report, according to the METAVIR scale.
All the participants included in the study were tested for elastography following the protocol recommended by the manufacturer and used in published pivotal studies, as follows:
The participants underwent SSWE on an empty stomach, and measurements were made of the right lobe of the liver through the intercostal spaces with the subject lying supine and with the right arm at maximum abduction.
The technique was used with a broadband convex probe (SC6-1). In the SSWE mode, shear waves are created in the tissue by acoustic force generated by ultrasound pulses. The speed of the shear wave was estimated by means of Doppler acquisition. (10) Shear wave velocity was used to calculate the rigidity of the tissues by applying the formula E = pc2, where E is the tissue elasticity in kilopascal (kPs), p is the density of the tissue (kg/m3), and c is the velocity of the shear wave (ms).
Elasticity data were color-coded by the software to create a two-dimensional map of tissue stiffness that is displayed in a box in the conventional B-mode image. A region of interest (ROI) was established in the box for measurement of liver stiffness. We used an average ROI of 2 cm and a box of 3.5 x 2.5 cm.
Measurements were classified as failed if there was no signal in the box, or if it was minimal in all acquisitions.
Statistical analysis
Statistical analyses were based on data obtained from at least 5 consecutive measurements which is equivalent to 15 SSWE measurements because the image in the box is the result of approximately three time-averaged images.
Information was analyzed descriptively by calculating measures of central tendency and dispersion for quantitative and categorical variables in absolute and relative frequencies for the total sample and by group according to biopsy. The assumption of normality for continuous data was validated by means of the Shapiro-Wilks test. Because the data did not present a normal distribution, the difference of the biopsy group was tested by the Wilcoxon rank-sum test. For the comparison between age groups, the Kruskal-Wallis test was used. All analyses were performed in STATA version 13.
In this study, there were no interventions or intentional modifications of the biological, physiological, psychological or social variables of the individuals. This study was conducted in accordance with the principles declared at the 1964 XVIII World Medical Assembly in Helsinki.
Results
We included 65 patients who had been diagnosed with cirrhosis. Their median age was 58 years (48-67), 40 were women (61.5%), and 25 were men (38.5%). All patients had been diagnosed with cirrhosis based on physical examination, laboratory tests, imaging and endoscopy. In addition, 32 patients had had previous liver biopsies compatible with stage F4 of the METAVIR scale. General patient and laboratory data are shown in Table 1.
Table 1 Patients diagnosed with cirrhosis by group (with or without biopsy)
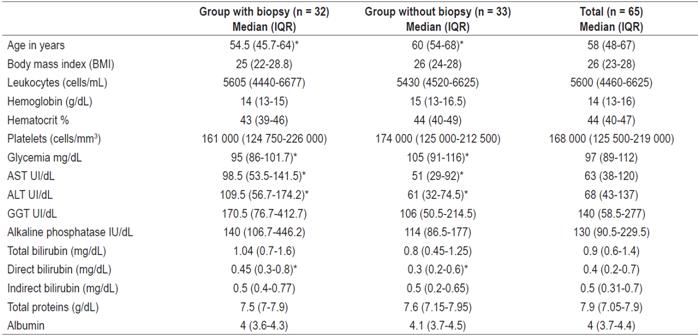
ALT: alanine aminotransferase; AST: aspartate aminotransferase; Cel: cells; GGT: gamma glutamyl transferase; IQR: interquartile range.
* Statistically significant differences between the two groups, p <0.05 (Wilcoxon Rank-sum test).
When the test was performed on 65 patients the median measurement was 16.6 kilopascal (kPs) with an interquartile range (IQR) of 13.9 to 19.5, a minimum measurement of 12 and a maximum measurement of 30.5 without any statistically significant difference between men and women (Figure 1). Neither were significant statistical differences of kP measurements found in a comparison of women with and without biopsies (p = 0.64). This same behavior was noticed in the group of men (p = 0.26). The comparison between men and women by biopsy group is detailed in Figure 2.
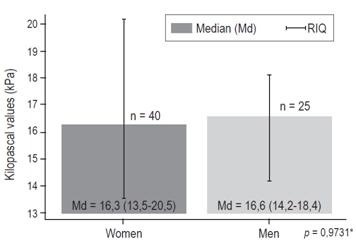
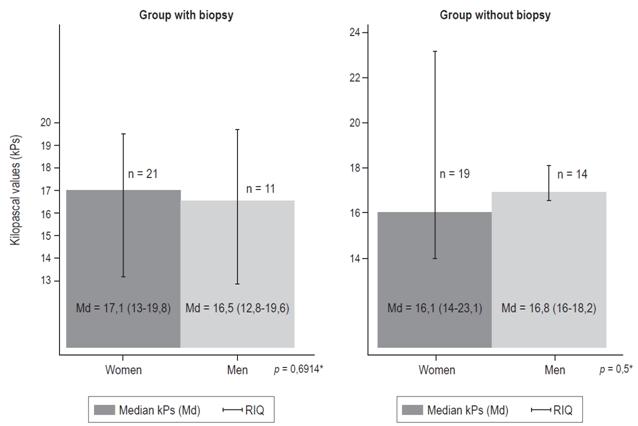
Figure 2 Hepatic stiffness according to sex. Groups with and without biopsy. IQR: interquartile range. * Wilcoxon rank-sum test.
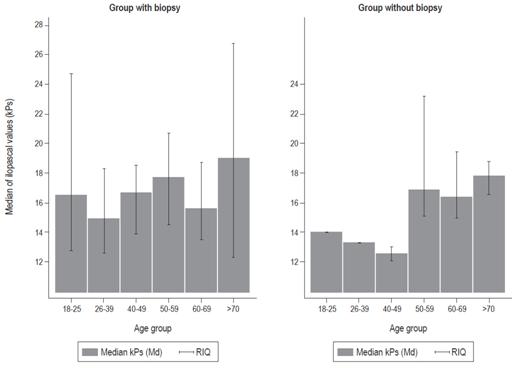
Table 2 and Figure 3 show stiffness according to age group and groups with biopsy and without biopsy. There were no statistically significant differences.
Table 2 Hepatic stiffness (kPs) by age group, with or without biopsy
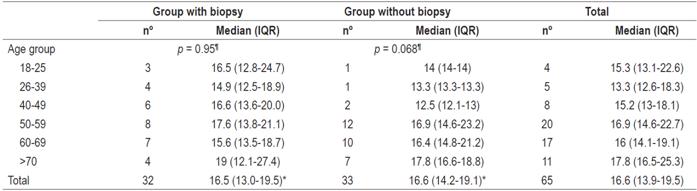
¶There were no significant differences between or among age groups with or without biopsy (Kruskal-Wallis test).
* p = 0.45 no significant differences between or among the groups (Wilcoxon rank-sum test).
Discussion
Measurement of the degree of liver fibrosis in a patient is essential for making decisions regarding treatment and prognosis of the disease. In cases of chronic hepatitis C, the detection of significant fibrosis is an indication for immediate antiviral treatment while the detection of cirrhosis is an indication for stricter monitoring of the patient to search for complications related to portal hypertension including hepatocellular carcinoma (HCC). Similarly, in cases of hepatitis B, advanced fibrosis or cirrhosis indicates treatment of the disease.15,16,17 In cases of fatty liver disease the same thing happens, although there are fewer studies.18,19
Classically, non-invasive ultrasound-based tests are excellent at the extremes of fibrosis due to the diagnostic validity of the technique with respect to a liver biopsy. 9 In relation to SSWE, the study by Leung and colleagues evaluated 226 carriers of chronic hepatitis B and showed that the METAVIR scores of fibrosis for stiffness measurements by SSWE (r = 0.81) were a better correlation than were the scores for transient elastography (r = 0.58). 20
The cutoff points calculated in that study were consistent with those found in a study by Ziol et al. of patients with chronic hepatitis C: 6.5 kPs (METAVIR F ≥1); 7.1 kPs (METAVIR F ≥2); 7.9 kPs (METAVIR F ≥3); and 10.1 kPs (METAVIR F4). 21 A study conducted in 2012 found very high performance for identification of severe fibrosis (greater than or equal to F3) and cirrhosis (F4). No significant differences were observed between the area under the receiver operating characteristic curve of TE and SWE in real time for severe fibrosis (0.96 and 0.98, respectively) or for cirrhosis (0.96 and 0.98, respectively), with cut-off points for SWE of 8.7 and 10.4, respectively. The median for cirrhosis was 15.6 with an IQR from 12.8 to 18.8 which is very similar to the one found in our study (16.6 kPs). 22 In the previously mentioned study, the data for cirrhosis were based on 24 patients with F4 by biopsy. The biopsy and the non-invasive tests were performed on the same day. This point to one of the main limitations in our study, because the time between the taking of biopsies and SSWE varied between one week and several years.
In the study by Herman et al., Etiologies of liver disease were categorized into chronic hepatitis C infections (HCV, n = 379) hepatitis B infections (HBV, n = 400), nonalcoholic fatty liver disease (NAFLD, n = 156) and a group of other liver diseases (n = 199). For diagnosis of severe fibrosis and cirrhosis, slightly lower cutoff points were found for patients infected with HBV (8.1 kPs and 11.5 kPs, respectively) than were found for all other patients (9.2 kPs and 13.4 kPs, respectively). In general, the diagnostic performance was better in patients with HBV and HCV than in patients without viral hepatitis. 23 In our study, although we knew the etiologies, we did not mention them because of the small number of patients. Future studies with an adequate sample size are necessary to perform these analyzes by type of etiology.
In summary, the cut-off points for cirrhosis in these three previous studies were between 10.1 and 13.4 kPs while in our study, the cut-off point was 12.0. Two important issues are raised: there was no significant difference between patients with biopsies and those without biopsies, and the median and IQR values are very similar to those found in the study by Ferraioli et al. 22
In between, our group’s previously published study on real time elastography in healthy patients found an average of 4.28 kPs with a standard deviation of 0.61. This combination of this second study with the previous one begin start to give more objective elements for normal and abnormal measurements in our patients. 24
Conclusion
Measurements of liver stiffness of the cirrhotic patients analyzed in this pilot study were within the range of those reported in initial studies of international tests. On this basis it can be suggested that this non-invasive test be performed in patients suspected of cirrhosis, thus avoiding the complications inherent in liver biopsies. SSWE could become a very useful test in clinical practice.
Acknowledgements
We thank our patients for agreeing to participate in this study
REFERENCES
1. Tsochatzis EA, Bosch J, Burroughs AK. Liver cirrhosis. Lancet. 2014;383(9930):1749-61. doi: 10.1016/S0140-6736(14)60121-5. [ Links ]
2. Garcia-Tsao G, Friedman S, Iredale J, Pinzani M. Now there are many (stages) where before there was one: in search of a pathophysiological classification of cirrhosis. Hepatology. 2010;51(4):1445-9. doi: http://doi.wiley.com/10.1002/hep.23478. [ Links ]
3. Lee UE, Friedman SL. Mechanisms of hepatic fibrogenesis. Best Pract Res Clin Gastroenterol. 2011;25(2):195-206. doi: https://doi.org/10.1016/j.bpg.2011.02.005. [ Links ]
4. Friedman SL. Mechanisms of hepatic fibrogenesis. Gastroenterology. 2008;134(6):1655-69. doi: https://doi.org/10.1053/j.gastro.2008.03.003. [ Links ]
5. Benvegnù L, Gios M, Boccato S, Alberti A. Natural history of compensated viral cirrhosis: a prospective study on the incidence and hierarchy of major complications. Gut. 2004;53(5):744-9. doi: https://doi.org/10.1136/gut.2003.020263. [ Links ]
6. Friedman SL, Bansal MB. Reversal of hepatic fibrosis - Fact or fantasy? Hepatology. 2006;43(S1):S82-8. doi: https://doi.org/10.1002/hep.20974. [ Links ]
7. Desmet VJ, Roskams T. Cirrhosis reversal: a duel between dogma and myth. J Hepatol. 2004;40(5):860-7. doi: https://doi.org/10.1016/j.jhep.2004.03.007. [ Links ]
8. Cassinotto C, Lapuyade B, Mouries A, Hiriart J-B, Vergniol J, Gaye D, et al. Non-invasive assessment of liver fibrosis with impulse elastography: comparison of Supersonic Shear Imaging with ARFI and FibroScan®. J Hepatol. 2014;61(3):550-7. doi: https://doi.org/10.1016/j.jhep.2014.04.044. [ Links ]
9. EASL-ALEH Clinical Practice Guidelines. Non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol. 2015;63(1):237-64. doi: https://doi.org/10.1016/j.jhep.2015.04.006. [ Links ]
10. Muller M, Gennisson JL, Deffieux T, Tanter M, Fink M. Quantitative viscoelasticity mapping of human liver using supersonic shear imaging: preliminary in vivo feasibility study. Ultrasound Med Biol. 2009;35(2):219-29. doi: https://doi.org/10.1016/j.ultrasmedbio.2008.08.018. [ Links ]
11. Samir AE, Dhyani M, Vij A, Bhan AK, Halpern EF, Méndez-Navarro J, et al. Shear-wave elastography for the estimation of liver fibrosis in chronic liver disease: determining accuracy and ideal site for measurement. Radiology. 2015;274(3):888-96. doi: https://doi.org/10.1148/radiol.14140839. [ Links ]
12. Tada T, Kumada T, Toyoda H, Ito T, Sone Y, Okuda S, et al. Utility of real-time shear wave elastography for assessing liver fibrosis in patients with chronic hepatitis C infection without cirrhosis: comparison of liver fibrosis indices. Hepatol Res. 2015;45(10):E122-9. doi: https://doi.org/10.1111/hepr.12476. [ Links ]
13. Yoneda M, Thomas E, Sclair SN, Grant TT, Schiff ER. Supersonic shear imaging and transient elastography with the XL probe accurately detect fibrosis in overweight or obese patients with chronic liver disease. Clin Gastroenterol Hepatol. 2015;13(8):1502-9. doi: https://doi.org/10.1016/j.cgh.2015.03.014. [ Links ]
14. Procopet B, Berzigotti A, Abraldes JG, Turon F, Hernandez-Gea V, García-Pagán JC, et al. Real-time shear-wave elastography: applicability, reliability and accuracy for clinically significant portal hypertension. J Hepatol. 2015;62(5):1068-75. doi: https://doi.org/10.1016/j.jhep.2014.12.007. [ Links ]
15. Ghany MG, Strader DB, Thomas DL, Seeff LB. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009;49(4):1335-74. doi: https://doi.org/10.1002/hep.22759. [ Links ]
16. European Association for the Study of the Liver. Recommendations on treatment of hepatitis C 2016. J Hepatol. 2018;66(1):153-94. doi: https://doi.org/10.1016/j.jhep.2016.09.001. [ Links ]
17. Sundaram V, Kowdley K. Management of chronic hepatitis B infection. BMJ. 2015;351(3):h4263. doi: https://doi.org/10.1136/bmj.h4263. [ Links ]
18. Haga Y, Kanda T, Sasaki R, Nakamura M, Nakamoto S, Yokosuka O. Nonalcoholic fatty liver disease and hepatic cirrhosis: comparison with viral hepatitis-associated steatosis. World J Gastroenterol. 2015;21(46):12989. doi: https://doi.org/10.3748/wjg.v21.i46.12989. [ Links ]
19. Farrell GC, Larter CZ. Nonalcoholic fatty liver disease: from steatosis to cirrhosis. Hepatology. 2006;43(S1):S99-112. doi: https://doi.org/10.1002/hep.20973. [ Links ]
20. Leung VY, Shen J, Wong VW, Abrigo J, Wong GL, Chim AM, et al. Quantitative elastography of liver fibrosis and spleen stiffness in chronic hepatitis b carriers: comparison of shear-wave elastography and transient elastography with liver biopsy correlation. Radiology. 2013;269(3):910-8. doi: https://doi.org/10.1148/radiol.13130128. [ Links ]
21. Ziol M, Handra-Luca A, Kettaneh A, Christidis C, Mal F, Kazemi F, et al. Noninvasive assessment of liver fibrosis by measurement of stiffness in patients with chronic hepatitis C. Hepatology. 2005;41(1):48-54. doi: https://doi.org/10.1002/hep.20506. [ Links ]
22. Ferraioli G, Tinelli C, Dal Bello B, Zicchetti M, Filice G, Filice C. Accuracy of real-time shear wave elastography for assessing liver fibrosis in chronic hepatitis C: a pilot study. Hepatology. 2012;56(6):2125-33. doi: https://doi.org/10.1002/hep.25936. [ Links ]
23. Herrmann E, de Lédinghen V, Cassinotto C, Chu WC, Leung VY, Ferraioli G, et al. Assessment of biopsy-proven liver fibrosis by two-dimensional shear wave elastography: an individual patient data-based meta-analysis. Hepatology. 2018;67(1):260-72. doi: https://doi.org/10.1002/hep.29179. [ Links ]
24. Prieto Ortíz JE, Sánchez Pardo S, Prieto Ortíz RG, Garzón-Orjuela N, Eslava-Schmalbach J. Elastografía en tiempo real (supersonic): comportamiento de la prueba en sujetos sanos de Bogotá. Rev Colomb Gastroenterol. 2017;32(4):332. [ Links ]
Received: January 15, 2018; Accepted: April 02, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
