










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.33 no.3 Bogotá July/Sept. 2018
https://doi.org/10.22516/25007440.282
Case report
Extra nodal follicular non-Hodgkin B lymphoma affecting the colon, on the basis of a case
1Médico, Cirujano General, Gastroenterólogo Clínico Quirúrgico. Coordinador, Programa de Gastroenterología Clínico-Quirúrgica, Universidad de Caldas, Manizales, Colombia
2Médico, Cirujano General, Gastroenterólogo Clínico-Quirúrgico. Docente, Programa de Gastroenterología Clínico-Quirúrgica, Universidad de Caldas, Manizales, Colombia
3Médico, Cirujano General, Gastroenterólogo Clínico-Quirúrgico, Universidad de Caldas, Manizales, Colombia
4Médico, Cirujano General, Residente de Gastroenterología Clínico-Quirúrgica, Universidad de Caldas, Manizales, Colombia
5Estudiante de Medicina, Universidad de los Andes, Bogotá, Colombia
Introduction:
Non-Hodgkin’s lymphoma (NHL) is a malignant disease that presents in an extranodal form. It affects the gastrointestinal tract in up to 50% of cases with the colon being the least frequently compromised portion. In the few cases in which it is affected, the cecum is most often compromised due to its large lymphoid content. The colon of the patient presented here was compromised by a mass in the cecum. Biopsies showed grade II follicular NHL with follicular and diffuse patterns. This histological type has the highest prevalence and has shown the best results with chemotherapy (R-CHOP scheme) alone and in conjunction with radiation therapy and occasionally with surgery. The patient received treatment followed by adequate evolution. Combination therapy has been shown to result in longer survival times, although there are studies which have reported good results with monotherapy as in this case.
Clinical Case:
The patient was a 38-year-old woman. A colonoscopy showed a tumor in the cecum. Its pathology was compatible with extra-follicular follicular NHL type B which was confirmed by immunohistochemistry. Imaging extension studies confirmed abdominal and thoracic adenopathies in conglomerates. The oncology department treated the patient with a chemotherapy with R-CHOP protocol with a good response.
Discussion and conclusions:
Since extranodal NHL rarely affects the colons, this case deserved to be reported. Management can be multidisciplinary, but the prognosis depends on individual characteristics in each case.
Keywords: Non-Hodgkin’s lymphoma; extranodal involvement; colon malignancy
Introducción:
el linfoma no Hodgkin (LNH) es una enfermedad maligna que presenta una forma extraganglionar que afecta al tracto gastrointestinal hasta en un 50 % de los casos; el colon es el órgano que con menor frecuencia se ve comprometido por este linfoma. En los pocos casos que presentan afección, el compromiso es principalmente del ciego, por su gran contenido linfoide. Este caso es el de una paciente con compromiso del colon por masa en el ciego. Las biopsias reportan LNH folicular grado II, patrones folicular y difuso, siendo este tipo histológico el de mayor prevalencia y el que ha mostrado los mejores resultados con el manejo con quimioterapia (esquema R-CHOP) sola o en conjunto con radioterapia; también, en ocasiones, con cirugía. La paciente recibió tratamiento con evolución adecuada. La terapia conjunta es la que ha demostrado mayor sobrevida, aunque hay estudios en los que se han reportados buenos resultados con monoterapia, como el caso en cuestión.
Caso clínico:
mujer de 38 años, en quien se realiza una colonoscopia que muestra una lesión tumoral en el ciego, con patología compatible con LNH tipo B folicular extranodal, confirmado por inmunohistoquímica. Los estudios de extensión imagenológicos confirman la presencia de adenopatías abdominales y torácicas en conglomerados. Oncología inicia el manejo con quimioterapia con protocolo R-CHOP, con buena respuesta.
Discusión y conclusiones:
el LNH extranodal afecta muy rara vez al colon, razón por la que este caso es reportado. El manejo puede ser multidisciplinario y su pronóstico depende de las características individuales en cada caso.
Palabras clave: Linfoma no Hodgkin; compromiso extranodal; malignidad de colon
Introduction
Non-Hodgkin’s lymphoma (NHL) is a malignant entity and the sixth cause of death in the United States. The extranodal form occurs in 10% to 33% of the population. The gastrointestinal tract is the most common site of appearance accounting for 50% of cases. In the West, the stomach predominates as the most frequently affected site (10% of malignant gastric neoplasms), followed by the small intestine (25% of cases) and the colon, which is the least affected (4% for extranodal forms and 0% and 0.2% to 0.4% for primary colonic neoplasms). (1,2
The vast majority of patients consult a physician late because of nonspecific symptoms such as asthenia, adynamia and weight loss.
Clinical case
The patient was a 38 year old woman who had had asthenia and adynamia for several months. During the physical examination, cervical lymphadenopathies and mild pain on palpation in the right iliac fossa were observed. Because of these symptoms, upper digestive endoscopy and colonoscopy were requested.
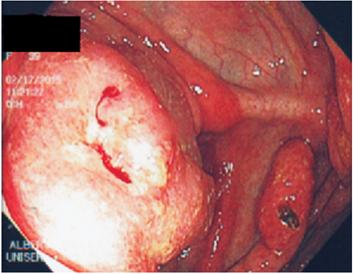
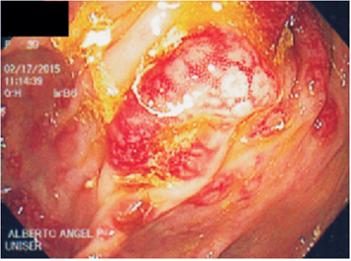
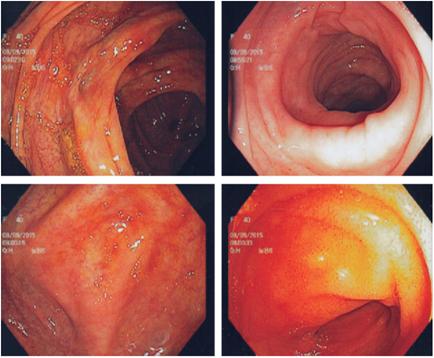
The colonoscopy showed a large polyp in the cecum (approximately 5 cm in diameter) which included a appendicular, stony orifice, from which biopsies are taken. In addition, The colonoscopy showed multiple hypervascularized sessile polyps 3 to 15 mm in diameter with conserved elasticity which gave a granular appearance to the mucosa throughout the colon including the rectum. Biopsies were taken. A diagnostic impression of the giant polyp was made in the cecum in order to rule out cancer and multiple polyposis of the colon (Figures 1, 2, 3 and 4).

The pathology department report indicated lymphoproliferative disease compatible with lymphoma. Immunohistochemistry found tumor cells with diffuse and strong positivity for CD20, CD10 and BCL2, local positivity for BCL6 and negativity in tumor cells for MUM 1, cyclin D1, CD3 and CD5. There were moderate amounts of positive markers in the accompanying T lymphoid population. The Ki 67 proliferation index was 95%.
The immunological and immunophenotypic profiles could not be classified but were intermediate between diffuse large B-cell lymphoma and Burkitt’s lymphoma. In the histological sections of the other polyps, grade II follicular B-cell NHL was found with follicular and diffuse patterns.
It is considered extranodal intestinal follicular B-cell NHL that had transformed to high grade lymphoma in the cecum extending to the rest of the colon (The majority of cases of intestinal involvement due to follicular lymphoma correspond to secondary involvement by follicular nodal NHL).
Computed tomography (CT) of the abdomen showed adenopathies in the abdominal cavity, including the retroperitoneal and peritoneal spaces, with involvement of the mesentery root. In the retroperitoneum the aortocaval, retrocaval and para-aortic spaces were all compromised. There were also adenopathies in the common iliac chains and in the inguinal regions, with loss of fatty hilum. Thickening of the walls of the colon from the rectum to the cecum (pancolitis) measured up to 13 mm in the most affected segments, but without compromising the stomach or small intestine. This was related to lymphoproliferative disease. The chest CT showed bilateral axillary adenopathies, predominantly left, one in a retropectoral location adjacent to the axillary vessels.
The patient was assessed by the oncology department which started treatment with the R-CHOP protocol (rituximab plus cyclophosphamide, hydroxydaunorubicin, vincristine [Oncovin®] and prednisone) because of the extent of the lesions. Progress has been excellent to date with complete resolution after treatment (Figure 5).
Discussion
The gastrointestinal tract is the most common site for extranodal NHL, and it can occur in up to 50% of cases. It can appear in any location from the oral cavity to the anus. In some cases several segments of the intestine such as the stomach, small intestine and rectum have been reported to be compromised, but with differences in presentation according to the clinical, histological and immunohistochemical points of view. Clinical presentation varies, but gastric with superficial proliferation and a lower grade histological type is the most common in elderly people. Intestinal lymphomas appear in younger groups, with deeper infiltration and generally at high grades. Some groups have reported better survival with surgical treatment than with medical treatment alone. 3
Colorectal involvement usually occurs in patients by the fourth or fifth decade of life, as in the case reported here. Difficult locating abdominal pain precisely is one of its most common symptoms. Pain may be accompanied by changes in bowel movements and sometimes by hemorrhaging. Upon physical examination, the most frequent finding is a palpable mass which is found in 30% to 88% of cases. Endoscopy sometimes finds diffuse thickening which, in principle, can appear to be adenocarcinoma. 4,5,6,7,8
The incidence in the general population continues to be low (0.02 per 100,000). Associated risk factors such as immunosuppression states of transplant patients, people with human immunodeficiency virus and people suffering from malnutrition have been identified. The male/female ratio of those affected is 2:1. When the colon is affected, the most frequent location is the cecum (from 74% to 86%). This may be related to the large amount of lymphoid tissue present in this area of the gastrointestinal tract. There is involvement of the sigmoid in 2.5% to 14.2% of cases. The prognosis of all cases that affect the intestine is related to the stage of the lymphoma as well as to its histological subtype. The World Health Organization (WHO) classification is the most frequently used system for these cases. It divides lymphomas into 40 subtypes with diffuse large cell lymphoma (31%) and follicular lymphoma (22%) being the most common followed by small lymphocytic lymphoma (6%), mantle cell lymphoma (6%), peripheral T-cell lymphoma (6%) and MALT lymphoma (5%). The most commonly reported surgery is right hemicolectomy since the vast majority of lesions are located only in the cecum. NHL is a multimodal systemic disease for which surgical management is used in cases that are considered to be prone to complications such as obstructions or perforations. 5
The best success rates with chemotherapy are achieved for tumors that are considered to be rapidly proliferative due to their histology. Of these, diffuse large cell lymphoma is the most sensitive to the CHOP chemotherapy regimen (cyclophosphamide, hydroxydaunorubicin, vincristine [Oncovin®] and prednisone). With this scheme, it is expected that there will be complete responses in up to 50% of patients and partial responses in up to 30% of patients. Although the prognosis may vary according to the stage of the tumor, regional radiation therapy with doses of 30 to 50 Gy has also achieved good responses for local control of lesions smaller than 3 cm. For larger tumors, reductions can reach up to 60% or 70%. 6,7
The best therapeutic modality has not yet been elucidated. The results of monotherapy with chemotherapy in gastric lymphoma have been extrapolated to other organs of the gastrointestinal tract. There are reports of systematic reviews that conclude that chemotherapy without surgery or radiotherapy is the best management modality and that it is associated with longer periods of disease-free survival than is surgical management with or without adjuvant therapy. 9) Currently, management modalities are still considered to be controversial. Given that the majority of authors support surgical management, it is accepted as a primary treatment strategy. Nevertheless, survival with chemotherapy alone was 92% at ten years and exceeded any other approach alone or in combination, and this makes it the optimal management. 10
Other studies show that the modality of combining chemotherapy with a surgical procedure is superior to the surgical procedure alone. The exceptions to this are patients with perforations or bleeding for whom survival changes drastically. In general terms, patients with grade I lymphomas have five-year survival rates of 60% to 80%; stage II patients have five-year survival rates from 40% to 60%, and stage III and IV patients have five-year survival rates of only 10% to 20%. These data encompass the entire population of lymphomas that occur in the intestine which makes it difficult to establish the prognosis of patients whose cancer compromises just the colon or one of its segments.
This patient initially developed typical symptoms of lymphoma, and the principal location was in the cecum. This is the most frequent location in the rare cases in which the colon is affected according to the literature. Management was initiated with the R-CHOP scheme and, according to the histological findings, the percentage of survival at five years may be between 40% and 60%.
Conclusion
Non-Hodgkin’s lymphoma (NHL) is a systemic disease that affects the gastrointestinal tract in up to 50% of cases.. The colon is the site with the lowest incidence. When the colon is affected, the cecum is the most frequently compromised area due to its large amount of lymphoid tissue. Management must be multidisciplinary and the combination of chemotherapy, radiotherapy and surgery must be individualized according to the histology of the tumor and the patient’s clinical state. Possible complications that may occur within the cancers natural history including perforation and bleeding that are associated with high risk of mortality must be weighed. Monotherapy is also effective in selected cases when there is adequate response. These variables must be taken into account, as they have an impact on survival.
Referencias
1. She WH, Day W, Lau PY, Mak KL, Yip AW. Primary colorectal lymphoma: case series and literature review. Asian J Surg. 2011;34(3):111-4. doi:10.1016/j.asjsur.2011.08.004. [ Links ]
2. Garza-Sánchez J, Hernández-Ramírez DA, Rocha-Ramírez JL, Rojas-Illanes M, Parrado-Montaño W, Cancino-López JA, et al. Non Hodgkin lymphoma of the sigmoid colon: case report. Rev Gastroenterol Mex. 2009;74(2):127-31. [ Links ]
3. Tevlin R, Larkin JO, Hyland JM, O’Connell PR, Winter DC. Primary colorectal lymphoma. A single centre experience. Surgeon. 2014;13(3):1-5. doi: 10.1016/j.surge.2014.01.002. [ Links ]
4. Beaton C, Davies M, Beynon J. The management of primary small bowel and colon lymphoma--a review. Int J Colorectal Dis. 2012;27(5):555-63. doi:10.1007/s00384-011-1309-2. [ Links ]
5. Lai YL, Lin JK, Liang WY, Huang YC, Chang SC. Surgical resection combined with chemotherapy can help achieve better outcomes in patients with primary colonic lymphoma. J Surg Oncol. 2011;104(3):265-8. doi: 10.1002/jso.21927. [ Links ]
6. Inaba K, Kushima R, Murakami N, Kuroda Y, Harada K, Kitaguchi M, et al. Increased risk of gastric adenocarcinoma after treatment of primary gastric diffuse large B-cell lymphoma. BMC Cancer. 2013;13:499. doi: 10.1186/1471-2407-13-499. [ Links ]
7. Lin HH, Jiang JK, Lin JK. Collision tumor of low-grade B-cell lymphoma and adenocarcinoma with tuberculosis in the colon: a case report and literature review. World J Surg Oncol. 2014;12:147. doi: 10.1186/1477-7819-12-147. [ Links ]
8. Iwamuro M, Okada H, Takata K, Takenaka R, Inaba T, Mizuno M, et al. Colorectal Manifestation of Follicular Lymphoma. Intern Med. 2016;55(1):1-8. doi: 10.2169/internalmedicine.55.5393. [ Links ]
9. Lightner A, Shannon E, Gibbons M, Russell M. Primary Gastrointestinal Non-Hodgkin’s Lymphoma of the Small and Large Intestines: a Systematic Review. J Gastrointest Surg. 2016;20(4):827-39. Doi: 10.1007/s11605-015-3052-4. [ Links ]
10. Ding D, Pei W, Chen W, Zuo Y, Ren S. Analysis of clinical characteristics, diagnosis, treatment and prognosis of 46 patients with primary gastrointestinal. Mol Clin Oncol. 2014;2(2):259-64. Doi: 10.3892/mco.2013.224. [ Links ]
Received: August 14, 2017; Accepted: November 10, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
