










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.33 no.4 Bogotá Oct./Dec. 2018
https://doi.org/10.22516/25007440.212
Original articles
Characteristics of dysphagia in patients of a gastroenterology center in Bogotá D.C., Colombia
1Centro médico Endocentro Limitada. Unidad de gastroenterología y endoscopia digestiva. Bogotá D. C., Colombia
2Centro médico Endocentro Limitada. Unidad de gastroenterología y endoscopia digestiva. Universidad Nacional de Colombia, sede Bogotá, Facultad de Medicina, Departamento de Medicina Interna. Bogotá D. C., Colombia
Introduction:
The epidemiology of dysphagia is poorly defined. It is a symptom that is associated with aging but is still a matter of uncertainty in young populations. Also, it is is not always reported by patients and is poorly understood in the general population.
Objective:
The objective of this study was to describe the clinical and epidemiological characteristics of dysphagia in a sample of adult patients referred to a center specializing in Gastroenterology.
Methodology:
This is an observational, descriptive and retrospective study carried out in a specialized gastroenterology center in Bogotá DC in 2016. We reviewed 3,148 clinical histories of patients to identify those whose reason for consultation was dysphagia or who were referred to the clinic with dysphagia as an associated symptom and whose diagnoses had been confirmed by complementary tests.
Results:
Of the 3,148 medical records, 85 (2.7%) presented dysphagia as the main reason for consultation or as an associated symptom. The majority were women (70.5%). The largest proportion of those affected were between 70 and 79 years old. Gastroesophageal reflux disease was the most frequent diagnosis.
Conclusion:
The prevalence of dysphagia found is similar to that reported in the literature. Gastroesophageal reflux disease is a frequent cause of dysphagia. Dysphagia continues to be a problem especially among the elderly.
Keywords (DeCS): Swallowing disorders; prevalence; epidemiology; adult; endoscopy
Introducción:
la epidemiología de la disfagia está pobremente definida. Es un síntoma que se asocia con el envejecimiento, y en poblaciones jóvenes sigue siendo tema de incertidumbre. También es un problema que no siempre informan los pacientes y es poco comprendido en la población general.
Objetivo:
describir las características clínicas y epidemiológicas de la disfagia a partir de una muestra de pacientes adultos remitidos a un centro especializado en gastroenterología.
Metodología:
estudio observacional, descriptivo y retrospectivo, realizado en un centro especializado en gastroenterología en Bogotá D. C. durante 2016, en el cual se revisaron 3148 historias clínicas y se recopilaron aquellas de pacientes cuyo motivo de consulta fuera disfagia o la refirieran como síntoma asociado, y cuyo diagnóstico se confirmara con pruebas complementarias.
Resultados:
de 3148 historias clínicas, 85 (2,7 %) presentaron disfagia como motivo de consulta principal o síntoma asociado. La mayoría correspondió a mujeres (70,5 %). El grupo de edad más afectado fue entre 70 y 79 años. La enfermedad por reflujo gastroesofágico (ERGE) representó el diagnóstico más frecuente.
Conclusión:
la prevalencia de disfagia encontrada es similar a la reportada en la literatura. La ERGE es causa frecuente de disfagia. La disfagia continúa siendo un problema predominantemente de adultos mayores.
Palabras clave: Trastornos de deglución; prevalencia; epidemiología; endoscopia; adulto
Introduction
Dysphagia is difficulty in the initial stages of swallowing, or the sensation of obstruction of the passage of food and/or liquids from the mouth to the stomach. 1 It can be classified as oropharyngeal or esophageal based on its location.2,3 Oropharyngeal dysphagia affects the mouth, pharynx or proximal esophagus and is almost always associated with neurological disorders such as cerebrovascular events, Parkinson’s disease and amyotrophic lateral sclerosis. It can also be related to anatomical changes such as Zenker’s diverticulum or cricopharyngeal bars.2 Esophageal dysphagia affects the esophageal body and esophagogastric junction and may be due to esophageal motility disorders such as primary esophageal motor disorder and scleroderma, to mucosal inflammation such as eosinophilic esophagitis and radiation esophagitis, or to structural abnormalities such as tumors, peptic stenosis, esophageal rings or extrinsic compression. 3
The epidemiology of dysphagia in Colombia is poorly defined. On one hand, the prevalence of most diseases that can cause dysphagia tends to differ among regions and continents. On the other hand, prevalence rates vary depend on the instrument or method with which the dysphagia is diagnosed. In addition, pathologies associated with dysphagia in groups of young people differ from those that occur in older adults. 3,4 Several previous studies have included other age groups, but their conclusions are always the same: dysphagia appears at older ages. Nevertheless, results have varied with estimations of prevalence ranging from 8% to 22% in patients older than 50 years of age. 4,5,6,7 Studies performed exclusively with patients from nursing homes have come to consider the prevalence of dysphagia at around 60%. 8,9 Epidemiology in younger populations remains a matter of uncertainty. 1
In contrast, perception of the problem among younger patients for whom it is associated with diseases such as gastroesophageal reflux has been improving. 10 Dysphagia represents a problem that is largely not reported and is poorly understood by the general population which leads to underdiagnosis. Therefore, only approximations of the frequency and etiology of dysphagia in the general adult population in Colombia is possible.
This descriptive study has determined the clinical and epidemiological characteristics of dysphagia from a sample of adult patients referred to a specialized gastroenterology center.
Materials and methods
This is a retrospective observational and descriptive study performed at the Centro Médico Endocentro Limitada located in in Bogotá D.C. The center specializes in gastroenterology services.
The medical records of 3,148 patients were reviewed to identify those who had come to the clinic as outpatients because of dysphagia or an associated symptoms from January 2 to December 31, 2016. Patients older than 16 who had diagnoses of dysphagia confirmed by complementary diagnostic tests such as esophagogastroduodenoscopy (EGD), functional tests or radiographic studies were included.
Data collected included age, type of food with which dysphagia manifested and results of complementary tests used to confirm diagnoses and associated comorbidities including clinical, endoscopic and paraclinical findings. All results were recorded in a Microsoft Office Excel® 2010 database for later analyses.
Confidentiality of patients’ information was guaranteed, and no record contained sensitive information about the identity of the patients. Informed consent was requested, and the study was approved by the research committee of the institution.
Results
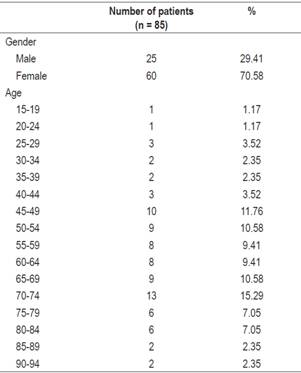
Of a total of 3,148 medical records reviewed, dysphagia or associated symptoms was identified as the main reason for consultation for 85 patients (2.7%). Sixty of these patients were women (70.5%), and the average age was 60.6 years (age range from 19 to 92 years). The distribution by sex and age is illustrated in Table 1.
Table 1 Sex and age distribution of patients whose dysphagia or associated symptoms was the main reason for consultation
According to the presence of signs suggestive of aspiration or penetration, 67.05% of the 85 patients presented dysphagia with solid foods, 3.5% with liquids and 29.41% with both consistencies. Associated comorbidities found were sequelae of cerebrovascular diseases (CVD) or other neurological disease in 7 patients (8.24%), rheumatological diseases that compromised gastrointestinal motility in 6 patients (7.05%), and histories of surgeries of the upper gastrointestinal tract in 5 patients (5.88%). No identifiable comorbidities were found in 27 patients (31.76%) at the time of the consultation. Figure 1 shows the main comorbidities found.

Figure 1 Principal comorbidities found in patients with dysphagia (n = 85). CVA: cardiovascular accident; COPD: chronic obstructive pulmonary disease.
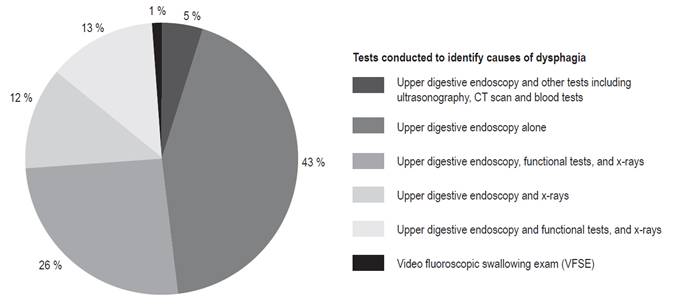
Eighty-four patients (99%) underwent EGD (with biopsies), and EGD was not required in only one case (1%) in which the diagnosis was made radiologically. Of the 84 patients, 37 (43.52%) required no other diagnostic tests, and 47 (55.29%) required other tests which included functional tests such as pH impedance monitoring, esophageal manometry and radiological examinations including esophagography and pharyngography. It is also worth mentioning that in 4 cases (4.7%) the cause was identified by EGD plus tests such as CT scans, ultrasound and or specific blood tests. Figure 2 shows the tests that were required over time to determine the cause of dysphagia.
The causes found for dysphagia are shown in Table 2. The most frequent causes of dysphagia were associated with ineffective esophageal motility. These included gastroesophageal reflux disease (GERD) (30.58%) and primary esophageal motor disorder (24.7%). Structural abnormalities such as tumors, peptic stenosis, esophageal rings and extrinsic compression accounted for 28.23% of cases (24 of 85 patients). Within this category, tumors were most frequent, accounting for 33.33% of the group (8 of 24 identified patients). Secondary associations with inflammatory causes of eosinophilic esophagitis or radiation esophagitis were identified in four patients (4.7%).
Table 2 Causes of dysphagia identified in patients who had dysphagia or associated symptoms as the main reason for consultation
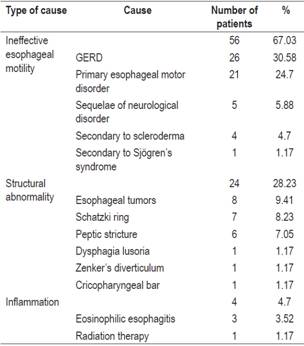
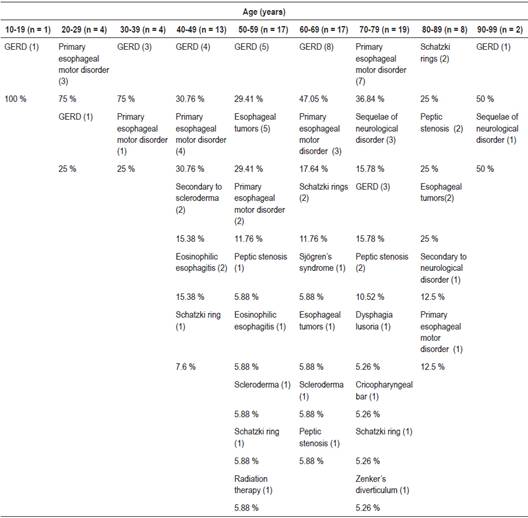
Table 3 shows the causes of dysphagia according to age groups. GERD was the main cause of dysphagia in most groups. Similarly, primary esophageal motor disorder, eosinophilic esophagitis and tumors predominated among patients under 60 years old while sequelae of neurological disorders, peptic stenosis and Schatzki’s rings predominated among older patients.
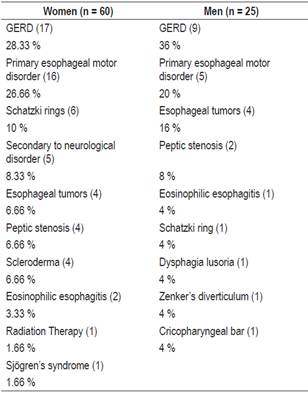
Finally, a comparison of the causes of dysphagia among women with those among men (Table 4) found that dysphagia related to autoimmune disorders and mucosal inflammation predominated among women while unusual causes of dysphagia were found such as dysphagia lusoria, Zenker’s diverticulum and cricopharyngeal rod were found among men.
Discussion
This study adds to our knowledge of the epidemiology of dysphagia in the adult population at the local level and indicates that its prevalence among patients who were not hospitalized but who consulted a center that specializes in gastroenterology is 2.7%. Despite methodological limitations, the information obtained included groups of younger patients and is relevant to for outpatient settings. Some sources have reported that prevalence of dysphagia in the general population can be as high as 6% to 9%. 11,12 Nevertheless, most studies have only included patients over 50 years of age. A study by Eslick et al. of 672 subjects over the age of 18 years found that 16% had presented dysphagia and that peak presentation occurred between 40 and 49 years of age. 7
This study found lower prevalence and a peak age of presentation between 70-79 years of age.
For the largest group of subjects in this study (30.58% of the patients), GERD was identified as a cause related to dysphagia. Associations between GERD and dysphagia have been described previously. In a study by Cho et al. that evaluated 7,640 patients, the prevalence of dysphagia of was found to be 3%, and GERD was associated with 30% of these cases. 1 Another study by Hoy et al. found that the mean age of presentation was 62 years and that 27% of the patients presented GERD. 13 That study assessed 100 patients with dysphagia at an outpatient care center specializing in swallowing disorders over a 15 month period of time.
A comparative study by Bollschweiler et al. showed that 28% of a group of patients with reflux suffered from dysphagia while only 3% of the control group did. They explained this association as the result of inadequate peristalsis induced by gastric acid. 14 Vakil et al. found that 37% of 11,945 patients with erosive esophagitis reported dysphagia. 15
Our finding that tumors caused a significant portion of dysphagia cases is consistent with the literature according to different age groups. 16. Similarly, a higher prevalence of dysphagia was found in adults over 60 years old, although it is known that some medical conditions such as neurological disorders may predispose to dysphagia. 17 Although this study only looked at the patient population of a gastroenterological center, lower proportions of GERD and primary esophageal motor disorder were found.
A large proportion of the patients with dysphagia in this study were women (70.5% of the cases). This may be partly attributable to the greater likelihood of women to request medical attention, to follow recommendations for diagnostic tests and to adhere to treatment. 18 Some studies have concluded that there is no biological explanation for different prevalences between the sexes and that women are more likely to report gastrointestinal symptoms.18,19 This study corroborates the fact that women are more likely to report problems of swallowing than are men. Further research is needed to clarify this association.
Finally, the tests required to identify the cause of dysphagia should be mentioned. A patient’s medical history and physical assessment can lead to appropriate testing or referral. 20 Because this was a study of patients at a gastroenterology center, at the moment of referral, the predominant symptoms of the majority of patients may have been suggestive of mechanical obstruction, so that the preferred test was digestive endoscopy. Other diagnostic methods such as functional and radiographic tests were found to have been initially chosen for a smaller proportion of patients. This is related to the fact that the majority of patients identified presented diagnoses of esophageal motility disorders. This is a limitation of this study which suggests that future studies should assess clinical characteristics of dysphagia including information from other specialties such as otorhinolaryngology, audiology and speech therapy, head and neck surgery, and neurology.
Conclusions
The prevalence of dysphagia in outpatient care at our institution is similar to that reported in the literature. Disorders due to ineffective esophageal motility accounted for the most frequent diagnoses corroborating the association of GERD with dysphagia. When younger groups are included, dysphagia continues to be a problem predominantly of those over 65 years of age. At the same time, it represents a problem whose approach should be multidisciplinary and which should include specialties other than just gastroenterology. Additional efforts are required to characterize the epidemiology of dysphagia throughout Colombia.
REFERENCES
1. Cho SY, Choung RS, Saito YA, Schleck CD, Zinsmeister AR, Locke GR 3rd, et al. Prevalence and risk factors for dysphagia: a USA community study. Neurogastroenterol Motil. 2015;27(2):212-9. doi: 10.1111/nmo.12467. [ Links ]
2. Achem SR, Devault KR. Dysphagia in aging. J Clin Gastroenterol. 2005;39(5):357-71. [ Links ]
3. Lawal A, Shaker R. Esophageal dysphagia. Phys Med Rehabil Clin N Am. 2008;19(4):729-45, viii. doi: 10.1016/j.pmr.2008.07.003. [ Links ]
4. Mann G, Hankey GJ, Cameron D. Swallowing function after stroke: prognosis and prognostic factors at 6 months. Stroke. 1999;30(4):744-8. [ Links ]
5. Lindgren S, Janzon L. Prevalence of swallowing complaints and clinical findings among 50-79-year-old men and women in an urban population. Dysphagia. 1991;6(4):187-92. [ Links ]
6. Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Thompson WG, et al. U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci. 1993;38(9):1569-80. [ Links ]
7. Eslick GD, Talley NJ. Dysphagia: epidemiology, risk factors and impact on quality of life--a population-based study. Aliment Pharmacol Ther. 2008;27(10):971-9. doi: 10.1111/j.1365-2036.2008.03664.x. [ Links ]
8. Shanley C, O’Loughlin G. Dysphagia among nursing home residents: an assessment and management protocol. J Gerontol Nurs. 2000;26(8):35-48. [ Links ]
9. Park YH, Han HR, Oh BM, Lee J, Park JA, Yu SJ, et al. Prevalence and associated factors of dysphagia in nursing home residents. Geriatr Nurs. 2013;34(3):212-7. doi: 10.1016/j.gerinurse.2013.02.014. [ Links ]
10. Tsukamoto M, Manabe N, Kamada T, Hirai T, Hata J, Haruma K, et al. Number of Gastrointestinal Symptoms is a Useful Means of Identifying Patients with Cancer for Dysphagia. Dysphagia. 2016;31(4):547-54. doi: 10.1007/s00455-016-9712-z. [ Links ]
11. Lind CD. Dysphagia: evaluation and treatment. Gastroenterol Clin North Am. 2003;32(2):553-75. [ Links ]
12. Brett A. Screening test for stroke-related dysphagia. J Watch Gen Med. 2009;29:166-7. [ Links ]
13. Hoy M, Domer A, Plowman EK, Loch R, Belafsky P. Causes of dysphagia in a tertiary-care swallowing center. Ann Otol Rhinol Laryngol. 2013;122(5):335-8. doi: 10.1177/000348941312200508. [ Links ]
14. Bollschweiler E, Knoppe K, Wolfgarten E, Hölscher AH. Prevalence of dysphagia in patients with gastroesophageal reflux in Germany. Dysphagia. 2008;23(2):172-6. doi: 10.1007/s00455-007-9120-5. [ Links ]
15. Vakil NB, Traxler B, Levine D. Dysphagia in patients with erosive esophagitis: prevalence, severity, and response to proton pump inhibitor treatment. Clin Gastroenterol Hepatol. 2004;2(8):665-8. [ Links ]
16. Roden DF, Altman KW. Causes of dysphagia among different age groups: a systematic review of the literature. Otolaryngol Clin North Am. 2013;46(6):965-87. doi: 10.1016/j.otc.2013.08.008. [ Links ]
17. Marik PE, Kaplan D. Aspiration pneumonia and dysphagia in the elderly. Chest. 2003;124(1):328-36. [ Links ]
18. Wilkins T, Gillies RA, Thomas AM, Wagner PJ. The prevalence of dysphagia in primary care patients: a HamesNet Research Network study. J Am Board Fam Med. 2007;20(2):144-50. doi: 10.3122/jabfm.2007.02.060045. [ Links ]
19. Heitkemper M, Jarrett M, Bond EF, Chang L. Impact of sex and gender on irritable bowel syndrome. Biol Res Nurs. 2003;5(1):56-65. doi: 10.1177/1099800403005001006. [ Links ]
20. Spieker MR. Evaluating dysphagia. Am Fam Physician. 2000;61(12):3639-48. [ Links ]
Received: February 13, 2018; Accepted: July 30, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
