










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957
Rev Col Gastroenterol vol.34 no.1 Bogotá Jan./Mar. 2019
https://doi.org/10.22516/25007440.355
Review articles
Emerging Concepts: Herb-Induced Liver Injury (HILI)
1 Médica de la Universidad Libre, epidemióloga clínica de la Fundación Universitaria de Ciencias de la Salud (FUCS), Residente de ginecología y obstetricia, FUCS. Bogotá D. C., Colombia
2 Internista, especialista en gastroenterología, Universidad Nacional de Colombia, Hospital Universitario Nacional de Colombia. Bogotá D. C., Colombia.
3 Profesor Titular de Medicina, Unidad de Gastroenterología, Universidad Nacional de Colombia, Hospital Universitario Nacional de Colombia. Gastroenterólogo Clínica Fundadores, Bogotá D. C., Colombia
Alternative therapies are considered to be a group of interventions that include the use of herbal and dietary supplements under the false premise that they offer great benefits to patients’ health without having adverse effects since they are “natural” products. In Colombia, naturopathic remedies are common, but their frequency of use is still unknown. Throughout the world there is great concern about these alternatives since hepatic injuries derived from their use have been clearly established. This has led to a new concept in medicine called HILI, an English language acronym for herb-induced liver injury.
Keywords: Natural remedies; hepatotoxicity; oxidative stress; homeopathy; HILI
Las terapias consideradas alternativas son un grupo de intervenciones que incluyen el uso de suplementos herbarios y dietéticos bajo la falsa premisa de ofrecer un gran beneficio sobre la salud del paciente sin tener que someterse al riesgo de presentar efectos adversos, ya que se tratan de productos naturales. En Colombia, los remedios naturistas son una práctica común, pero la frecuencia de uso todavía es desconocida. A nivel mundial existe una gran preocupación al respecto, ya que se ha establecido con claridad la asociación existente con injuria hepática debido a su uso, lo cual ha motivado a introducir un concepto nuevo en medicina denominado injuria hepática inducida por productos herbales (HILI).
Palabras clave: Remedios naturales; hepatotoxicidad; estrés oxidativo; homeopatía; HILI
Introduction
Herbal preparations have been used since the time of ancient Egypt,and their formulations have been maintained for centuries in empirical and oral tradition. 1 Herbal products are available in various forms including roots, seeds, leaves, teas, powders, oils, creams, capsules and even injectables. 2 In the last two decades, their use has increased exponentially all around the world. Currently, more than 60 million people are estimated to use them at costs that exceed 30 billion dollars. 3 This impressive market is fundamentally due to the fact that doctors and patients consider that natural remedies are completely free of side effects just because they are natural.
Patients are often told that, although gasoline comes from petroleum, a natural product, it must be extracted and go through complex purification processes before it can be used in motor vehicles. Similarly, beneficial substances in the components of the plants must be extracted and purified to separate them from other toxic substances that may also be present.
It is very worrisome when the hepatotoxic potential of these substances, either direct or due to interaction with other substances or with medications, is ignored. 4 More than 1,000 naturopathic products have been associated with hepatotoxicity, and the list continues to grow. Due to the magnitude of this problem, the term hepatic injury induced by herbal products (HILI) has been introduced. HILI is different from drug-induced hepatic injury (DILI). 5 The Drug-Induced Liver Injury Network of the United States has found that approximately 15% to 20% of reported cases of drug-induced liver injury are actually cases of damage due to the use of natural products. 5,6 Global data reveal that HILI increased from 7% to 20% between 2004 and 2013, 7 but there are no precise data on the frequency of HILI because patients do not report use, they self-medicate, and they are prescribed by people without training. 8 For these reasons, hepatotoxicity associated with the use of these remedies is often not suspected, is unknown and often goes unnoticed. 9
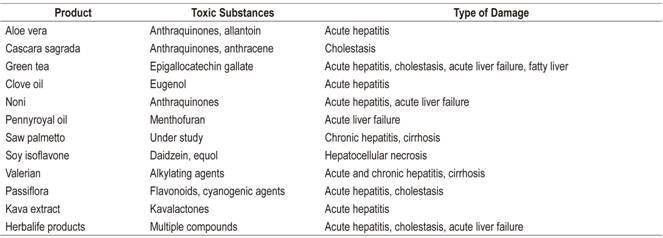
Due to concern about the great danger of these substances, the National Health Institutes of the United States has created the LiverTox website, a continuously updated database of these substances and their dangers which is available online at http://www.livertox.nih.gov/
Table 1 shows some of the most popular products that are on that list.
Epidemiology
The true incidence of liver damage induced by naturopathic medications and dietary supplements is unknown, and the data found probably underestimate the reality. 10 The United States Fod and Drug Administration (FDA), the USA’s pharmacovigilance agency, has determined that the annual incidence in that country is 2.7 cases per 100,000 adults. 11 A Korean study that included 371 cases reported by 17 hospitals between 2005 and 2007 found the incidence of HILI among patients who required hospitalization was 5.8 patients per year. 12 Reliable data from Iceland show that HILI’s incidence there is three cases per 100,000 people. 13 In the Spanish registry, lower but increasing numbers of HILI have been reported, ranging from 2% in 1998 to 6% in 2016. 14
In Germany, a study that included 51 hospitals in Berlin between 2002 and 2011 revealed that 10 of the 198 cases of hepatotoxicity (5%) were attributable to natural products. 15 A review from China that included 21,789 patients found that natural remedies ranked second as a cause of liver damage to tuberculous drugs. 16 In Latin America, preliminary data from the LATIN DILI Network show that 10% of cases of acute liver damage are attributable to naturopathic products. In other words, this constitutes a worldwide public health problem. 17
Risk factors for hepatotoxicity
Unlike conventional medicines, herbal preparations contain unknown concentrations of various ingredients. 18 The unusual increase in their consumption can be attributed to factors including patient dissatisfaction with medical treatment and its adverse effects, easy access, low cost, absence of any requirements for prescriptions. 19
The liver is the main target organ affected by toxicity due to naturopathic remedies because of the metabolic processes that occur there. 20 Live damage occurs insidiously. and outcomes vary and are nonspecific. Several reported cases have required liver transplantation and others have died. 5
Contrary to beliefs in the general population and in some sectors of pseudoscientific societies, plants have toxic active ingredients and/or produce secondary metabolites that are toxic. 21 The risk is even greater when preparations mix several natural products. 22 Other variables involved in the development of injury and subsequent liver damage are excessive consumption and consumption of substances whose composition is not listed on the label. 23 Less than 10% of the products based on naturopathic compounds have truly standardized active components. 24 In addition to all of these factors, there is a belief within many companies that manufacture naturopathic remedies that heavy metals such as lead, mercury, cadmium or arsenic improve the effectiveness of their products so they are frequently used as ingredients. 25
Pathogenesis and classification
Hepatotoxicity, the most frequent adverse reaction to naturopathic remedies, occurs in susceptible individuals and are usually transient and self-limiting, although cases of chronic liver disease and acute liver failure have been described.26,27 Clinically, hepatotoxicity is similar to that produced by medications. 28 Both categories of liver damage are caused by chemical substances from natural or synthetic products which are foreign to the organism and which require metabolization to eliminate them. 29 Many of these preparations contain two key biological components, alkaloids and flavonoids, that are associated with liver damage. 30 Their interactions with isoforms of cytochrome P-450 trigger inflammation and oxidation which are the main pathways to liver damage. 31
There are two types of HILI: idiosyncratic and intrinsic. The first is unpredictable, long-term and dose-dependent while the second consists of predictable reactions to therapeutic doses or to overdoses with short periods of latency and high incidences among consumers of natural products. 32
HILI can also be chronic or acute depending on whether the alteration or liver damage lasts more or less than 6 months. 33 From the biochemical point of view, damage may be predominantly hepatocellular as indicated by high levels of aminotransferases, cholestatic as indicated by high levels of alkaline phosphatase), or it can be mixed. 34
An important consideration for managing HILI is that the possibility and percentage of individuals who develop chronic HILI are higher than for DILI. 35
Clinical manifestations
The disease’s spectrum varies. Although its clinical presentation is nonspecific, its predominant symptoms are gastrointestinal and include nausea, vomiting and abdominal pain. Asymptomatic alterations of the hepatic profile can occur, and severe cases can feature acute hepatic damage, fulminant hepatic insufficiency and complications derived from advanced liver disease or cirrhosis. 36,37 When patients stop using the product producing the damage, clinical signs begin to decrease, with subsequent normalization of the liver profile. 38 A series of 27 cases of HILI due to naturopathic drugs found the following distribution of liver damage patterns: 82% hepatocellular, 11% cholestatic, and 7% mixed. 39
Diagnosis
HILI is diagnosed through exclusion which implies a high degree of clinical suspicion. Evaluation of the liver profile is necessary to establish the type of lesion. 19 HILI’s clinical and histopathological manifestations are similar to those for other causes of acute or chronic liver disease (Table 2), 40 and these must be ruled out depending on the characteristics of the patient.
Table 2 Causes of acute and chronic liver disease
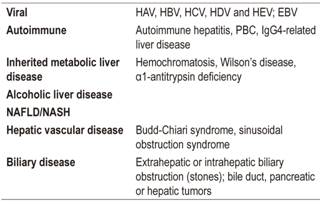
PBC: primary biliary cholangitis; NAFLD: non-alcoholic fatty liver disease; NASH: non-alcoholic steatohepatitis; EBV: Epstein-Barr virus; HAV: hepatitis A virus; HBV: hepatitis B virus; HCV: hepatitis C virus; HDV: hepatitis D virus; HEV: hepatitis E virus
Characteristics that suggest hepatotoxicity induced by homeopathic remedies include absence of disease prior to use of the naturopathic medicine, development of the disease or the biochemical alterations after beginning its use, and improvement that occurs after the product is withdrawn. 41 There is no gold standard, nor are there any specific tests or serum biomarkers to confirm a diagnosis of liver injury induced by naturopathic remedies. Several diagnostic tools have been validated, but it is still difficult to prove that causality is related to a specific drug, so care should be taken to rule out other causes of liver disease. 20
It is imperative patients be asked specifically about consumption of such substances, since patients do not recognize them as medicines and usually consider them so harmless that it is unnecessary to mention them. In addition, it is not uncommon for patients to take multiple preparations which makes it impossible to identify a single causative toxin. 42 In addition, it has been found that self-medicating patients increase doses to help treat new symptoms when damage becomes acute. 43
Several scales that attempt to codify the causality of drug toxicity with objective criteria have been developed. The best known are Naranjo (Table 3) and the Roussel Uclaf Causality Assessment Method (RUCAM) which is available at http://www.rccc.eu/scores/RUCAM.html. Studies that have compared these models suggest that the RUCAM scale may have better discriminatory capacity. Although these scales have not been validated in the field of herbal medicines, they are often used as clinical aids. 44
Table 3 Causality Scale for Adverse Reactions
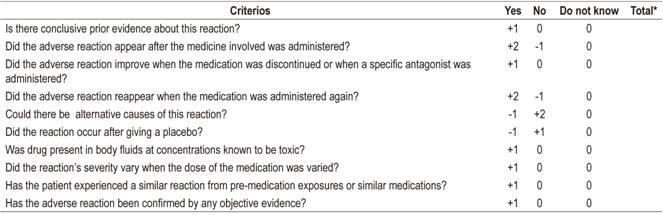
* The causality of an adverse reaction is determined by the total score which can be between 4 and 13. A score over 9 is considered to prove causality, scores of 5 to 8 indicate probable causality, scores from 1 to 4 indicate possible causality, and scores of zero or less indicate doubtful causality. Taken from: Naranjo CA, du Souich P, Busto UE. Methods in clinical pharmacology. PAHO; 1992
Liver biopsies
A series of HILI cases has reported detailed histological descriptions of the most frequent pathological findings including hepatitis, necrosis, eosinophil infiltrates, fibrosis and cholestasis. 45 Nevertheless, liver biopsies are not considered to be routinely useful because they do not provide information relevant to the management of patients and may cause additional complications. 46,47 It is not recommended that liver biopsies not be taken routinely to evaluate cases of HILI but should be reserved only for cases of atypical clinical presentation. 48
Treatment
The mainstay of treatment is removal of any and all toxins being administered while monitoring the patient closely until symptoms resolve. 49 Early identification is essential since it can modify the prognosis and evolution of the disease. 50 Most patients recover after the product is discontinued. Recommended medical management addresses symptoms. 51
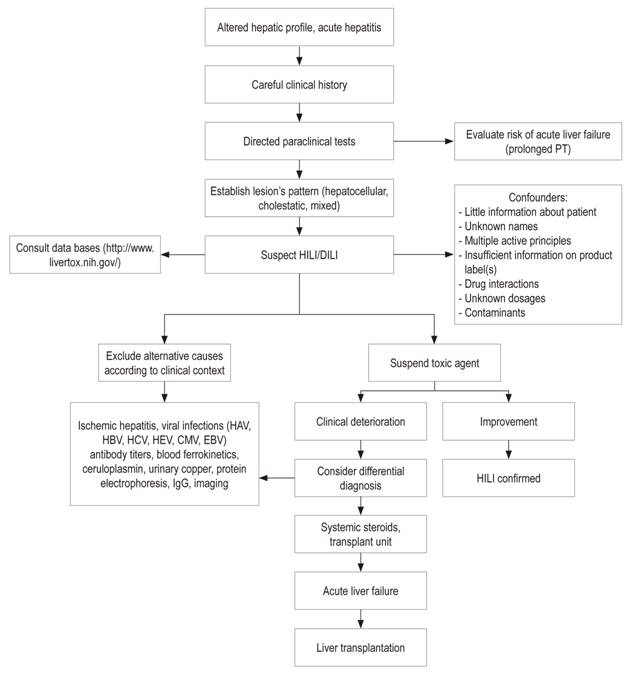
Although systemic steroids are frequently used, they have no proven benefit for most forms of hepatotoxicity. Nevertheless, they may be useful for treating patients with hypersensitivity reactions. 52 Severe cases of fulminant hepatic failure require management by liver transplant units since mortality rates without transplantation are close to 80%. 53 Alterations in the hepatic profile that point towards the possibility of progressing to acute liver failure in the context of HILI are total bilirubin twice the normal upper limit in association with aminotransferases three times the upper limit of normal. These findings require hospitalization to ensure close monitoring. 54,55 Figure 1 shows an algorithm of suggestions for patient management.
Conclusion
The non-medical public traditionally considers herbal products to be safe because they are natural. However, this belief is absolutely wrong since such substances, or naturopathic remedies, can produce serious and even fatal adverse reactions. Regrettably, they are distributed in the market without the support of controlled clinical trials that demonstrate their efficacy and safety. More seriously, unlike for conventional allopathic medicines, there is no rigorous supervision by regulatory bodies that have the scientific capacity to understand the problem and which have sufficient knowledge to understand the chemical characteristics of the active ingredients of these substances and how they are metabolized.
The composition and quality of these substances vary, so evaluation of causality is a true diagnostic challenge. Products that contain multiple ingredients can cause more severe liver damage than those with a single ingredient. National registries and multicenter research networks have been created to overcome limitations such as a broad spectrum of phenotypes, severity, idiosyncratic reactions and individual susceptibility.
Although the efficacy and safety of herbal products remain uncertain until now, their clinical repercussions can be serious and even lethal. The liver is the primary main organ involved.
Many clinical studies are needed to determine effectiveness of these substances, clarify their mechanisms of action, and ascertain risks derived from their use. Our recommendation is that the sale, prescription and use of these compounds be immediately suspended. Permits for their use and prescription must await the results of rigorous clinical trials that demonstrate their therapeutic potential. Also, physicians should be motivated to report and record patients with hepatotoxicity secondary to HILI that they often identify. All adverse reactions to these substances should be documented and reported to regulators
Referencias
1. Schuppan D, Jia JD, Brinkhaus B, Hahn EG. Herbal products for liver diseases: a therapeutic challenge for the new millennium. Hepatology. 1999;30(4):1099-104. doi: 10.1002/hep.510300437. [ Links ]
2. Lindstrom A, Ooyen C, Lynch ME, Blumenthal M, Kawa K. Sales of herbal dietary supplements increase by 7.9% in 2013, marking a decade of rising sales: Tumeric supplements climb to top ranking in natural channel. Herbal Gram. 2014;103:52-6. [ Links ]
3. Tindle HA, Davis RB, Phillips RS, Eisenberg DM. Trends in use of complementary and alternative medicine by US adults: 1997-2002. Altern Ther Health Med. 2005;11(1):42-9. [ Links ]
4. Larrey D. Hepatotoxicity of herbal remedies. J Hepatol. 1997;26 Suppl 1:47-51. [ Links ]
5. Eisenberg DM, Kessler RC, Van Rompay MI, Kaptchuk TJ, Wilkey SA, Appel S, et al. Perceptions about complementary therapies relative to conventional therapies among adults who use both: results from a national survey. Ann Intern Med. 2001;135(5):344-51. [ Links ]
6. Nahin RL, Barnes PM, Stussman BJ. Expenditures on Complementary Health Approaches: United States, 2012. Natl Health Stat Report. 2016;(95):1-11. [ Links ]
7. Navarro VJ, Barnhart H, Bonkovsky HL, Davern T, Fontana RJ, Grant L, et al. Liver injury from herbals and dietary supplements in the U.S. Drug-Induced Liver Injury Network. Hepatology . 2014 ;60(4):1399-408. doi: 10.1002/hep.27317. [ Links ]
8. Bunchorntavakul C, Reddy KR. Review article: herbal and dietary supplement hepatotoxicity. Aliment Pharmacol Ther. 2013;37(1):3-17. doi: 10.1111/apt.12109. [ Links ]
9. Navarro VJ. Herbal and dietary supplement hepatotoxicity. Semin Liver Dis. 2009;29(4):373-82. doi: 10.1055/s-0029-1240006. [ Links ]
10. Vega M, Verma M, Beswick D, Bey S, Hossack J, Merriman N, et al. The Incidence of Drug- and Herbal and Dietary Supplement-Induced Liver Injury: Preliminary Findings from Gastroenterologist-Based Surveillance in the Population of the State of Delaware. Drug Saf. 2017;40(9):783-787. doi: 10.1007/s40264-017-0547-9. [ Links ]
11. Suk KT, Kim DJ, Kim CH, Park SH, Yoon JH, Kim YS, et al. A prospective nationwide study of drug-induced liver injury in Korea. Am J Gastroenterol. 2012;107(9):1380-7. doi: 10.1038/ajg.2012.138. [ Links ]
12. Cho JH, Oh DS, Hong SH, Ko H, Lee NH, Park SE, et al. A nationwide study of the incidence rate of herb-induced liver injury in Korea. Arch Toxicol. 2017;91(12):4009-15. doi: 10.1007/s00204-017-2007-9. [ Links ]
13. Björnsson ES, Bergmann OM, Björnsson HK, Kvaran RB, Olafsson S. Incidence, presentation, and outcomes in patients with drug-induced liver injury in the general population of Iceland. Gastroenterology. 2013;144(7):1419-25, 1425.e1-3. doi: 10.1053/j.gastro.2013.02.006. [ Links ]
14. Medina-Caliz I, Garcia-Cortes M, Gonzalez-Jimenez A, Cabello MR, Robles-Diaz M, Sanabria-Cabrera J, et al. Herbal and Dietary Supplement-Induced Liver Injuries in the Spanish DILI Registry. Clin Gastroenterol Hepatol. 2018;16(9):1495-1502. doi: 10.1016/j.cgh.2017.12.051. [ Links ]
15. Douros A, Bronder E, Andersohn F, Klimpel A, Kreutz R, Garbe E, et al. Herb-Induced Liver Injury in the Berlin Case-Control Surveillance Study. Int J Mol Sci. 2016;17(1). pii: E114. doi: 10.3390/ijms17010114. [ Links ]
16. Reuben A, Koch DG, Lee WM; Acute Liver Failure Study Group. Drug-induced acute liver failure: results of a U.S. multicenter, prospective study. Hepatology . 2010;52(6):2065-76. doi: 10.1002/hep.23937. [ Links ]
17. Bessone F, Hernández N, Sanchez-Ciceron A, Di Pace M, Gualano G, Arrese M, et al. A comparative analysis of the Spanish and Latin-American prospective drug-induced liver injury (DILI) networks. Hepatology . 2015;62(Suppl 1):504. [ Links ]
18. Tomlinson B, Chan TY, Chan JC, Critchley JA, But PP. Toxicity of complementary therapies: an eastern perspective. J Clin Pharmacol. 2000;40(5):451-6. [ Links ]
19. Kennedy J. Herb and supplement use in the US adult population. Clin Ther. 2005;27(11):1847-58. doi: 10.1016/j.clinthera.2005.11.004. [ Links ]
20. Seeff LB, Lindsay KL, Bacon BR, Kresina TF, Hoofnagle JH. Complementary and alternative medicine in chronic liver disease. Hepatology . 2001;34(3):595-603. doi: 10.1053/jhep.2001.27445. [ Links ]
21. Medina-Caliz I, Gonzalez-Jimenez A, Bessone F, Hernández N, Sánchez A, Di Pace M, et al. Variations in drug-induced liver injury (DILI) between different prospective DILI registries. Clin Ther. 2013;35(8):Se24. doi: 10.1016/j.clinthera.2013.07.057. [ Links ]
22. Teschke R, Eickhoff A. Herbal hepatotoxicity in traditional and modern medicine: actual key issues and new encouraging steps. Front Pharmacol. 2015;6:72. doi: 10.3389/fphar.2015.00072. [ Links ]
23. Viganó M, Lampertico P, Colombo M. Acute hepatitis following assumption of a herbal remedy. Eur J Gastroenterol Hepatol. 2008;20(4):364-5. doi: 10.1097/MEG.0b013e3282f2bbe5. [ Links ]
24. Ifeoma O, Oluwakanyinsola S. Screening of herbal medicines for potential toxicities. Intech Open [internet] 2013 [acceso el 24 de marzo de 2018]. doi: 10.5772/54493. Disponible en: Disponible en: https://www.intechopen.com/books/new-insights-into-toxicity-and-drug-testing/screening-of-herbal-medicines-for-potential-toxicities . [ Links ]
25. Espinoza EO, Mann MJ, Bleasdell B. Arsenic and mercury in traditional Chinese herbal balls. N Engl J Med. 1995;333(12):803-4. doi: 10.1056/NEJM199509213331217. [ Links ]
26. Pantano F, Mannocchi G, Marinelli E, Gentili S, Graziano S, Busardò FP, et al. Hepatotoxicity induced by greater celandine (Chelidonium majus L.): a review of the literature. Eur Rev Med Pharmacol Sci. 2017;21(1 Suppl):46-52. [ Links ]
27. Zhu Y, Niu M, Chen J, Zou ZS, Ma ZJ, Liu SH, et al. Hepatobiliary and pancreatic: Comparison between Chinese herbal medicine and Western medicine-induced liver injury of 1985 patients. J Gastroenterol Hepatol. 2016;31(8):1476-82. doi: 10.1111/jgh.13323. [ Links ]
28. Amadi CN, Orisakwe OE. Herb-Induced Liver Injuries in Developing Nations: An Update. Toxics. 2018;6(2). pii: E24. doi: 10.3390/toxics6020024. [ Links ]
29. Frenzel C, Teschke R. Herbal Hepatotoxicity: Clinical Characteristics and Listing Compilation. Int J Mol Sci . 2016;17(5). pii: E588. doi: 10.3390/ijms17050588. [ Links ]
30. Kwon H, Lee SH, Kim SE, Lee JH, Jee YK, Kang HR, et al. Spontaneously reported hepatic adverse drug events in Korea: multicenter study. J Korean Med Sci. 2012;27(3):268-73. doi: 10.3346/jkms.2012.27.3.268. [ Links ]
31. Li B, Wang Z, Fang JJ, Xu CY, Chen WX. Evaluation of prognostic markers in severe drug-induced liver disease. World J Gastroenterol. 2007;13(4):628-32. [ Links ]
32. Chalasani NP, Hayashi PH, Bonkovsky HL, Navarro VJ, Lee WM, Fontana RJ; et al. ACG Clinical Guideline: the diagnosis and management of idiosyncratic drug-induced liver injury. Am J Gastroenterol. 2014 ;109(7):950-66. doi: 10.1038/ajg.2014.131. [ Links ]
33. Chinese Medical Association, Xu JM. Cooperative Group of Hepatobiliary Disease of Digestive Disease Branch of Chinese Medical Association: A multicenter survey on hospital inpatients with drug-induced acute liver injury in China. Chin J Dig (Chin). 2007;27:439-42. [ Links ]
34. Wu XN, You H, Jia JD. Clinical features of drug-induced liver injury: a review of Chinese literature 2003-2007. Chin Hepat (Chin) 2008;13(8):463-6. [ Links ]
35. Chalasani N, Fontana RJ, Bonkovsky HL, Watkins PB, Davern T, Serrano J, et al. Causes, clinical features, and outcomes from a prospective study of drug-induced liver injury in the United States. Gastroenterology. 2008;135(6):1924-1934.e1-4. doi: 10.1053/j.gastro.2008.09.011. [ Links ]
36. Koff RS. Herbal hepatotoxicity. Revisiting a dangerous alternative. JAMA. 1995;273(6):502. [ Links ]
37. Hu YY, Huang F. Chinese herb and drug-induced liver injury. Zhonghua Gan Zang Bing Za Zhi. 2012;20(3):173-5. [ Links ]
38. Lin G, Wang JY, Li N, Li M, Gao H, Ji Y, et al. Hepatic sinusoidal obstruction syndrome associated with consumption of Gynura segetum. J Hepatol. 2011;54(4):666-73. doi: 10.1016/j.jhep.2010.07.031. [ Links ]
39. Zhu Y, Li YG, Wang Y, Wang LP, Wang JB, Wang RL, et al. Analysis of Clinical Characteristics in 595 Patients with Herb-induced Liver Injury. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2016;36(1):44-8. [ Links ]
40. Kales SN, Christophi CA, Saper RB. Hematopoietic toxicity from lead-containing Ayurvedic medications. Med Sci Monit. 2007;13(7):CR295-8. [ Links ]
41. Strader DB, Seeff LB. Zakim and Boyer hepatology. En: Boyer TD, Wrigth TL, Manns MP (editores). Hepatotoxicity of herbal preparations. Filadelfia: Elsevier; 2006. p. 551-60. [ Links ]
42. Zimmerman HJ, Ishak KG. General aspects of drug-induced liver disease. Gastroenterol Clin North Am. 1995;24(4):739-57. [ Links ]
43. Lucena MI, Camargo R, Andrade RJ, Perez-Sanchez CJ, Sanchez De La Cuesta F. Comparison of two clinical scales for causality assessment in hepatotoxicity. Hepatology . 2001;33(1):123-30. doi: 10.1053/jhep.2001.20645. [ Links ]
44. Chinese Society of Hepatology , CMA. Guidelines for the management of drug-induced liver injury. Lin Chuang Gan Dan Bing Za Zhi. 2015;31(11):1752-69. doi: 10.3969/j.issn.1001-5256.2015.11.002. [ Links ]
45. Barritt AS 4th, Lee J, Hayashi PH. Detective work in drug-induced liver injury: sometimes it is all about interviewing the right witness. Clin Gastroenterol Hepatol. 2010;8(7):635-7. doi: 10.1016/j.cgh.2010.03.020. [ Links ]
46. Ernst E. Adulteration of Chinese herbal medicines with synthetic drugs: a systematic review. J Intern Med. 2002;252(2):107-13. [ Links ]
47. Rochon J, Protiva P, Seeff LB, Fontana RJ, Liangpunsakul S, Watkins PB, et al. Reliability of the Roussel Uclaf Causality Assessment Method for assessing causality in drug-induced liver injury. Hepatology . 2008;48(4):1175-83. doi: 10.1002/hep.22442. [ Links ]
48. Wang JB, Zhu Y, Bai ZF, Wang FS, Li XH, Xiao XH; et al. Guidelines for the Diagnosis and Management of Herb-Induced Liver Injury. Chin J Integr Med. 2018;24(9):696-706. doi: 10.1007/s11655-018-3000-8. [ Links ]
49. O’Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology. 1989;97(2):439-45. [ Links ]
50. Björnsson E. Drug-induced liver injury: Hy’s rule revisited. Clin Pharmacol Ther. 2006;79(6):521-8. doi: 10.1016/j.clpt.2006.02.012. [ Links ]
51. Reuben A. Hy’s law. Hepatology . 2004;39(2):574-8. doi: 10.1002/hep.20081. [ Links ]
52. Shaw D, Leon C, Kolev S, Murray V. Traditional remedies and food supplements. A 5-year toxicological study (1991-1995). Drug Saf. 1997;17(5):342-56. doi: 10.2165/00002018-199717050-00006. [ Links ]
53. He TT, Wang JB, Bai ZF, Guo YM, Niu M, Zhu Y, et al. Guidelines for clinical diagnosis and treatment of herb-induced liver injury. Zhongguo Zhong Yao Za Zhi. 2017;42(24):4893-4897. doi: 10.19540/j.cnki.cjcmm.20170919.001. [ Links ]
54. Neff GW, Reddy KR, Durazo FA, Meyer D, Marrero R, Kaplowitz N. Severe hepatotoxicity associated with the use of weight loss diet supplements containing ma huang or usnic acid. J Hepatol. 2004;41(6):1062-4. doi: 10.1016/j.jhep.2004.06.028. [ Links ]
55. Woolf GM, Petrovic LM, Rojter SE, Wainwright S, Villamil FG, Katkov WN, et al. Acute hepatitis associated with the Chinese herbal product jin bu huan. Ann Intern Med. 1994;121(10):729-35. [ Links ]
Received: May 07, 2018; Accepted: September 15, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
