










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista colombiana de Gastroenterología
versión impresa ISSN 0120-9957versión On-line ISSN 2500-7440
Rev. colomb. Gastroenterol. vol.35 no.2 Bogotá abr./jun. 2020
https://doi.org/10.22516/25007440.416
Articles
Anxiety status and trait in Colombian schoolchildren and adolescents with and without functional gastrointestinal disorders

1 Pediatra, gastroenterólogo y nutriólogo, profesor titular del Departamento de Pediatría, Universidad del Valle. Cali, Colombia.
2 Pediatra. Hospital Regional María Inmaculada, Florencia, Colombia.
3 Estudiante de Medicina. Pontificia Universidad Javeriana. Cali, Colombia.
Introduction:
The pathophysiology of functional gastrointestinal disorders includes alteration of the gut-brain axis.
Objective:
This study measures prevalence and of functional gastrointestinal disorders and discusses possible associations with anxiety in children with these conditions.
Methodology:
This is a prevalence study of children between 8 and 18 years of age diagnosed with functional gastrointestinal disorders as defined by the Rome III Criteria and anxiety as defined by the State-Trait Anxiety Inventory for Children in several Colombian cities. Sociodemographic and family variables were included. Statistical analyses included measures of central tendency, univariate and multivariate analysis, and logistic regression, with p <0.05 established as significant.
Results:
The study included 1,496 children of whom 50.5% were girls. The boys average age was 12.7 ± 2.1 years, 79.9% had suffered transitory anxiety, and 51.5% had tendencies to experience states of anxiety. State/anxiety predominated in male adolescents while trait/anxiety predominated in female adolescents with functional gastrointestinal disorders. Possible risk factors for state/anxiety were age and sex. Possible risk factors for trait/anxiety were age, sex, and functional gastrointestinal disorders.
Conclusions:
About half of the children tended to states of anxiety. Female adolescents predominated with risk factors of age, sex, and some functional gastrointestinal disorders.
Keywords: Anxiety; diseases of the digestive system; children
Introducción:
la fisiopatología de los desórdenes gastrointestinales funcionales (DGF) incluye un eje intestino-cerebro alterado.
Metodología:
estudio de prevalencia realizado en ciudades colombianas en niños entre 8 y 18 años a quienes se les identificaron DGF según los Criterios de Roma III y ansiedad por medio del State Trait Anxiety Inventory for Children. Se incluyeron variables sociodemográficas y familiares. El análisis estadístico incluyó medidas de tendencia central, análisis uni- y multivariados, y regresión logística, teniendo en cuenta una p < 0,05 como significativa.
Resultados:
se incluyeron 1496 niños, 12,7 ± 2,1 años, 50,5 % niñas, 79,9 % con ansiedad transitoria y 51,5 % con tendencia a experimentar estados de ansiedad. Hubo predominio para el estado-ansiedad en adolescentes masculinos y para el rasgo-ansiedad en adolescentes femeninas con algún DGF. Los posibles factores de riesgo fueron la edad y el sexo para estado-ansiedad, y la edad, el sexo y los DGF para el rasgo-ansiedad.
Conclusiones:
cerca de la mitad de los niños tuvo tendencia a presentar estados de ansiedad, con predominio de las adolescentes femeninas y con factores de riesgo como la edad, el sexo y tener algún DGF.
Palabras clave: Ansiedad; enfermedades del sistema digestivo; niños
Introduction
Functional gastrointestinal disorders (FGD) in schoolchildren and adolescents are defined as a diverse and variable combination of recurrent or chronic gastrointestinal symptoms that are not attributable to other medical conditions after adequate medical evaluation. 1 The Rome criteria provide symptom-based guidelines by which FGDs can be diagnosed in schoolchildren and adolescents. 1,2 The 2006 Rome III criteria emphasize that “there should be no evidence of organic disease”. This leads to diagnoses based on paraclinical testing. 2 The 2016 Rome IV criteria replaced the text “that there is no evidence of an inflammatory, anatomical, metabolic or neoplastic process that explains the child’s symptoms” with “after proper medical evaluation, symptoms cannot be attributed to another medical condition”. This change allows for performance of selective paraclinical tests but does not require them for diagnosis of FGDs. 1. The worldwide prevalence of FGDs is between 10.0% and 30.0%. 3,4
The Rome IV Criteria propose pathophysiological characteristics for FGDs in which the gut-brain axis is altered by severity of pain (visceral hypersensitivity), psychosocial stress (anxiety, depression, impulsivity and anger) and other factors. 1
The State-Trait Anxiety Inventory for Children 1 (STAIC-1) is designed to measure transitory states of anxiety (stressful situations) while STAIC-2 measures anxiety traits defined as relatively stable tendencies to experience states of anxiety (neurotic tendencies). 5
A number of studies of children have found comorbidity between recurrent abdominal pain (RAP) and anxiety. One study found this comorbidity in 67.7%, another in 79%, another in 81%, and a fourth study found it in 81.6% of those studied. 6,7,8,9 Given the close relation between RAP and anxiety, a greater understanding of both disorders is important for understanding the pathophysiology of RAP and proposing preventive and therapeutic measures for this functional digestive disorder.
The objective of this article is to determine the prevalence and possible risk factors for anxiety in Colombian schoolchildren and adolescents with FGDs.
Methodology
This is a descriptive, cross-sectional and observational study carried out in the third to eleventh grade in four public schools in four cities: La Unión in Nariño; Cartagena in Bolívar; Florencia in Caquetá; and Santander de Quilichao in Cauca. Schoolchildren’s ages ranged from 8 to 18 years. Between February 24 and November 18, 2014, they were diagnosed with FGD based on the Roma III Questionnaire for Pediatric Gastrointestinal Symptoms for Schoolchildren and Adolescents (QPGS-III). In previous studies it has demonstrated the validity of its content and construction. 10-13. The STAIC-1 and STAIC-2 questionnaires were used to determine state-anxiety and trait-anxiety. 5 Their internal consistency in children has a Cronbach’s alpha between 0.87 and 0.90. 14,15 Children between 8 and 10 years old did the QPGS-III in a guided manner with one of the principal investigators, and children between 11 and 18 years old self-reported.
Sociodemographic variables such as age and sex, separated/divorced parents, intrafamily FGD and whether subjects were only children were taken into account.
Following the Rome III Criteria, children were placed into the following groups: vomiting and aerophagia (cyclical vomiting syndrome and adolescent rumination syndrome); abdominal pain related to FGDs (functional dyspepsia, irritable bowel syndrome, abdominal migraine, functional abdominal pain [FAP] and functional abdominal pain syndrome [FAPS]); and constipation and incontinence (functional constipation [FC] and non-retentive fecal incontinence). 1
STAIC-1 and STAIC-2 were used to classify children according to whether they had transitory anxiety or a tendency to experience anxiety states when their total score according to their sex was above the 50% percentile score. 5
The total sample size was calculated to be 360 children based on the following factors:
Reported prevalence of anxiety in children with RAP is between 67.7% and 81.6%. 6-9
Children included were taken from the total population of the FINDERS database (n = 4394). 16
The z-value for the 95% confidence level (1-alpha) is 1.96 with an absolute precision of 0.05.
Fifteen percent was added to the sample size for non-response.
This left an oversample of 1,496 children (La Unión, Nariño = 442; Cartagena, Bolívar = 401, Florencia, Caquetá = 331 and Santander de Quilichao, Cauca = 322).
We reviewed 10% of the data to identify any possible transcription errors and to compare with the original forms. Statistical analysis included measures of central tendency (mean, standard deviation, percentage). To determine prevalence, the data were analyzed using a two-tailed Student’s T test, a chi squared (χ2) test and Fisher’s exact test. A regression analysis with a probability of 20% was used to check for possible associations. The odds ratios (OR) with their respective 95% confidence intervals (CI) setting significance at a p <0.05 (Stata 10 software; StataCorp, College Station, Texas) were recorded.
Results
General Characteristics
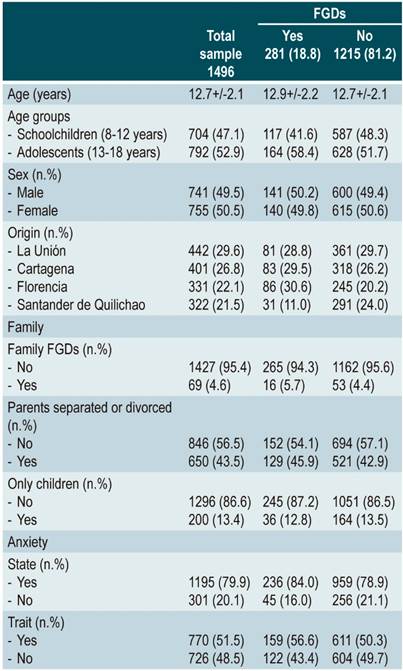
We included 1,496 schoolchildren and adolescents whose average age was 12.7 ± 2.1 years (range: 8 to 18 years). Of these children, 50.5% were female. Significant differences were found for the age group between 13 and 18 years of age, for children from Florencia, Caquetá and Santander de Quilichao, Cauca, and for those with state-anxiety (transitory anxiety) and trait-anxiety (tendency to experience states of anxiety). The parents of 43.5% of the children were either separated or divorced, 13.4% of the subjects were only children, and 4.6% had histories of familial FGDs. FGDs were identified in 18.8%: FC in 9.2%; IBS in 3.7%, and FAP and FAPS in 2.3% each (Table 1).
Analysis of Association
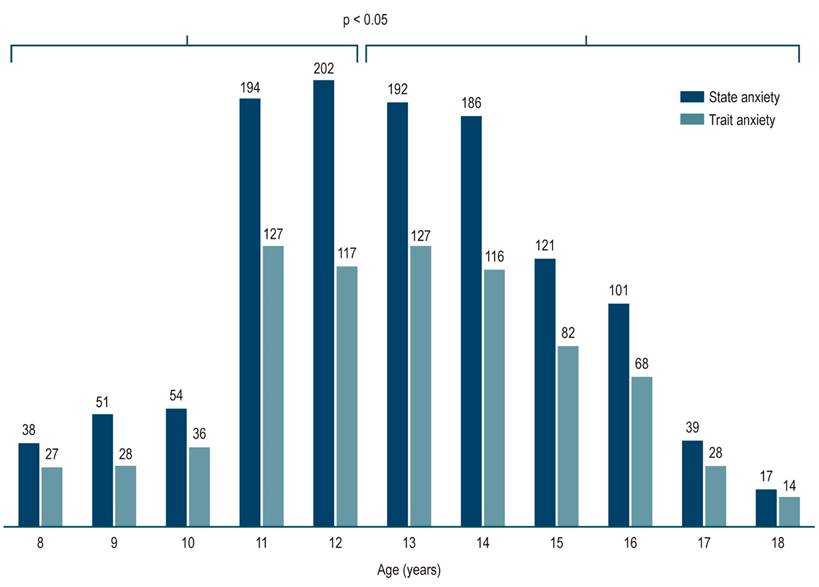
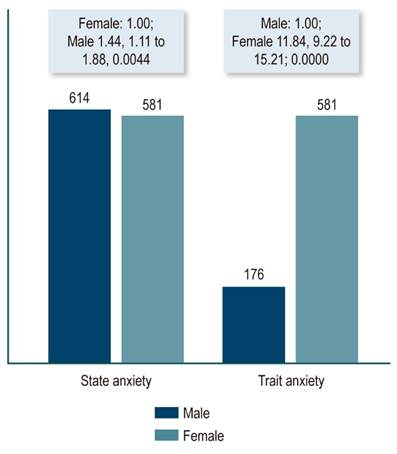
Adolescents between 13 and 18 years of age predominated in the group of children with state-anxiety (transitory anxiety) (OR: 1.47; 95% CI: 1.13-1.91; p = 0.0026) (Figure 1). Male subjects also predominated within the state anxiety group (OR: 1.44; 95% CI: 1.11-1.88; p = 0.0044) (Figure 2). Analysis of the children in the trait-anxiety group (tendency to experience anxiety states) found a predominance of adolescents (OR: 1.34; 95% CI: 1.08-1.65; p = 0.0046) (Figure 1), females (OR: 11.84; 95% CI: 9.22-15.21; p = 0.0000) and children with relatives with FGD (OR: 1.94; 95% CI: 1, 13-3.39; p = 0.0097). No possible associations were found between the presence of any FGD and state-anxiety or trait-anxiety even when each of the main FGDs (FC, IBS, FAP and FAPS) was individually analyzed (p> 0.05). This was also true for the other variables studied.
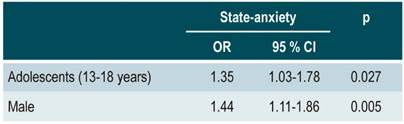
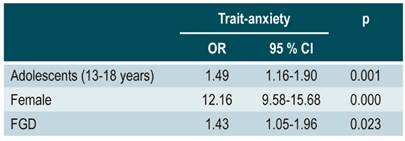
After controlling for possible confounders, the variables that best explained the presence of state-anxiety (transitory anxiety) were the age group of adolescents and male sex (Table 2). Those that best explained the presence of trait-anxiety (tendency to experience anxiety states) were the age group of adolescents, female sex and the presence of some FGD (Table 3).
Discussion
Prevalence of FGDs
Prevalence of FGDs was 18.8% In this group of Colombian schoolchildren and adolescents. The most common FGD was FC (9.2%), followed by IBS (3.7%) and FAP together with FAPS (2.3%). These data are similar to those previously reported in Colombia 16, Latin America 4 and elsewhere. 3
Prevalence of State-anxiety and Trait-anxiety
The prevalences for state-anxiety and trait-anxiety in this study were 20.1% and 48.5%, respectively. These data are similar to those reported by Cunningham et al. 17 Their study of 100 North American children between 8 and 18 years of age (13.0 ± 3.1 years; 73.0 % girls; 87.0% Caucasian) who had been diagnosed with FAP according to the Rome III Criteria found that 74.0% had had abdominal pain for more than one year. Symptoms of anxiety were identified according to the Screen for Child Anxiety Related Disorders-Parent/Child Report (SCARED-C/P). The study found that 54% of children with FAP has symptoms of anxiety (44.0% with panic-somatic symptoms, 43.0% with generalized anxiety and 42.0% with separation anxiety).
Possible Associations
Our study found that trait anxiety predominated among adolescents, females and those with familial FGDs. We found that neither trait anxiety nor state anxiety predominated in the group with vomiting and aerophagia, those with abdominal pain related to FGDs, and those with constipation and incontinence. This was true even when each FGD was individually analyzed (p> 0.05). These data are similar to those of Rutten et al. who found no significant differences among anxiety symptoms, IBS, and FGD-related FAP (p = 0.34) in 259 Dutch children between 8 and 18 years of age (132 children with IBS: 59.1%; IBS-e +: 25.8%; IBS-m +: 10.6%; IBS-d +: 4.5%; IBS-ss: 13.5 ± 2 , 9 years; 67.4% girls and 127 boys with abdominal pain related to FGD: 40.2%; FAP +: 59.8%; FAPS: 13.3 ± 2.7 years; 74.0% girls). They determined anxiety by means of the Revised Anxiety and Depression Scale - short version (RCADS-25).
However, authors such as Gulewitsch et al. have reported the opposite. 19 They studied children between 7.5 and 13 years of age. Their study population was 53.3% girls and included 18 children who had been diagnosed with FAP and six who had been diagnosed with IBS according to the Rome III criteria whose mean age was 9.8 ± 1.6 years. It also included 24 healthy children aged 9.9 ± 1.6 years and 12 children with anxiety disorders defined by STAIC aged 10.1 ± 1.6 years. They found that healthy children (32.01 ± 5.90) showed much more anxiety according to STAIC (p <0.01) than did children with abdominal pain (FAP + IBS) (38.42 ± 8.26). They did not report altered reactions of the parasympathetic nervous system during stress for any of the three study groups.
Possible Risk Factors
Our study has found possible risk factors relating trait-anxiety, gender, age and the presence of an FGD. A study by Waters et al. of 54 North American children between 6 and 13 years of age who had been diagnosed with anxiety (53.7% girls, 9.6 ± 1.4 years) and 51 healthy children (62.7% girls, 9.7 ± 1 , 9 years old) found that the group of anxious children had more symptoms of FGD than did the control group (p <0.001). The most common FGD was FC. Anxiety symptoms were identified by means of the Spence Children’s Anxiety Scale (SCAS-P, SCAS-C) and functional gastrointestinal disorders were identified by the Questionnaire on Pediatric Gastrointestinal Symptoms (QPGS) Rome Criteria. The group of anxious children with FGD had higher total scores on SCAS-C and SCAS-P than did to the group of anxious children without FGD and those of the healthy control group. Similarly, the study found an association between family histories of gastrointestinal problems and anxious children with (p <0.04) and without FGDs (p <0.007). They concluded that the incidence of symptoms consistent with FGD was significantly higher in children diagnosed with anxiety disorders than those who were not diagnosed with anxiety disorders. 20
Pollard et al. found that gastrointestinal symptoms decreased in pediatric patients with abdominal pain related to FGDs during the summer months (p = 0.017). They studied 34 North American children (61.8% girls, 10 ± 3 years of age) using the Revised Child Anxiety and Depression Scale (RCAD) and the Rome III criteria. 21 However, it was not clear whether the decrease in anxiety was the cause or the effect of the decrease in symptoms of FGD-related abdominal pain.
Finally, Shelby et al. 22 conducted a study of 332 North American children with FAP (63.8% girls; 89.7% white; 11.7 ± 2.5 years; 40.1% with FGD, 27.4 % IBS + 17.8% FD) and a control group of 159 children (54.4% girls; 94.5% white; 10.8 ± 2.0 years; 7.5% with FGD, 6.3% IBS + 1, 9% DF). They identified anxiety using the Adult Lifetime and Child and Parent Versions of the Anxiety Disorders Interview Schedule-IV(ADIS) and followed subjects for at least 5 years. They found a higher proportion of children with anxiety disorders among those who had FAP than within the control group at baseline (OR: 4.59; 95% CI: 2.83-7.43; p = 0.001) and at follow-up (OR: 3.57; 95% CI) %: 2.00-6.36; p = 0.001).
Our study was cross-sectional, but longitudinal studies such as the one by Cunningham et al. have also been conducted. 23 That study followed 64 North American children between 8 and 18 years of age (average 13.6 years, 42.2% with IBS; 85.9% Caucasian; 75.0% girls) for 6 months and identified possible risk factors such as pain, disability and anxiety through the Screen for Child Anxiety-related Disorders-Child Report (SCARED-C) and found that two or more factors risk predict a torpid course in children with FGD.
Our study found that younger age is a possible protective factor, and that sex and the presence of FGDs are other factors related to development of anxiety. Our hypothesis is that possible predisposing or risk factors that have not been epidemiologically confirmed, include genetic and constitutional, temperamental, parenting styles, stressful life events, and unfavorable social environments, but that females have greater anxiety in general.
In conclusion, even though about half of the children studied presented relatively stable tendencies to have anxiety states, their prevalence is difficult to determine given methodological difficulties related to the delimitation and definition of anxiety. Similarly, a predominance of children between 13 and 18 years of age and of the female sex has been reported. Possible risk factors include age, sex and the presence of FGDs. Further studies that include other possible risk factors are needed. Genetic, constitutional, temperamental, parental style, stressful life events and unfavorable social environments are among the risk factors that should be considered
REFERENCES
1. Hyams JS, Lorenzo CD, Saps M, Shulman RJ, Staiano A, van Tilgurg M. Childhood Functional Gastrointestinal Disorders: Child/Adolescent. Gastroenterology. 2016;150(5):1456-68. https://doi.org/10.1053/j.gastro.2016.02.015 [ Links ]
2. Rasquin A, Di Lorenzo C, Forbes D, Guiraldes E, Hyams JS, Staiano A, Walker LS. Childhood functional gastrointestinal disorders: Child/adolescent. Gastroenterology . 2006;130(6):1527-37. https://doi.org/10.1053/j.gastro.2005.08.063 [ Links ]
3. Boronat AC, Ferreira-Maia AP, Matijasevich A, Wang Y-P. Epidemiology of functional gastrointestinal disorders in children and adolescents: A systematic review. World J Gastroenterol. 2017;23(21):3915-27. https://doi.org/10.3748/wjg.v23.i21.3915 [ Links ]
4. Velasco-Benítez CA, Saps M, Chanís R, Játiva E, Zablah R, Mejía M, Rodríguez L, Leyva A, Moreno J, Ramírez CR, Sánchez MP, Aragón LE, Nichols-Vinuenza D. La epidemiología de los desórdenes gastrointestinales funcionales en escolares y adolescentes latinoamericanos. Acta Gastroenterol Latinoam. 2017;47(2):148-58. [ Links ]
5. Spielberg CD. State-Trait Anxiety Inventory for Children Professional Manual. Redwood City, CA: Mind Garden, Inc.; 1973. [ Links ]
6. Dufton LM, Dunn MJ, Compas BE. Anxiety and Somatic Complaints in Children with Recurrent Abdominal Pain and Anxiety Disorders. J Pediatr Psychol 2009;34(2):176-86. https://doi.org/10.1093/jpepsy/jsn064 [ Links ]
7. Campo JV, Bridge J, Ehmann M, Altman S, Lucas A, Birmaher B, Di Lorenzo C, Iyengar S, Brent DA. Recurrent abdominal pain, anxiety, and depression in primary care. Pediatrics. 2004;113(4):817-24. https://doi.org/10.1542/peds.113.4.817 [ Links ]
8. Garber J, Zeman J, Walker L. Recurrent abdominal pain in children: psychiatric diagnoses and parental psychopathology. J. Am. Acad. Child Adolesc. Psychiatry. 1990;29(4):648-56. https://doi.org/10.1097/00004583-199007000-00021 [ Links ]
9. Liakopoulou-Kairis M, Alifieraki T, Protagora D, Korpa T, Kondyli K, Dimosthenous E, Christopoulos G, Kovanis T. Recurrent abdominal pain and headache: psychopathology, life events and family functioning. Eur Child Adolesc Psychiatry. 2002;11(3):115-22. https://doi.org/10.1007/s00787-002-0276-0 [ Links ]
10. Walker LS, Lipani TA, Greene JW, Caines K, Stutts J, Polk DB, Caplan A, Rasquin-Weber A.. Recurrent Abdominal Pain: Symptom Subtypes Based on the Rome II Criteria for Pediatric Functional Gastrointestinal Disorders. J Pediatr Gastroenterol Nutr. 2004;38(2):187-91. [ Links ]
11. Caplan A, Walker L, Rasquin A. Development and preliminary validation of the questionnaire on pediatric gastrointestinal symptoms to assess functional gastrointestinal disorders in children and adolescents. J Pediatr Gastroenterol Nutr . 2005;41(3):296-304. [ Links ]
12. Caplan A, Walker L, Rasquin A. Validation of the Pediatric Rome II Criteria for Functional Gastrointestinal Disorders Using the Questionnaire on Pediatric Gastrointestinal Symptoms. J Pediatr Gastroenterol Nutr . 2005;41(3):305-16. [ Links ]
13. Saps M, Nichols-Vinueza DX, Mintjens S, Pusatcioglu CK, Velasco-Benítez CA. Construct validity of the pediatric Rome III criteria. J Pediatr Gastroenterol Nutr . 2014;59(5):577-81. https://doi.org/10.1097/MPG.0000000000000482 [ Links ]
14. Spielberger CD. Manual for the state-trait inventory for children. Palo Alto, CA: Consulting Psychologists; 1973. [ Links ]
15. Walker LS, Beck JE, Garber J, Lambert W. Children’s Somatization Inventory: Psychometric properties of the revised form (CSI-24). J Pediatr Psychol . 2009;34(4):430-40. https://doi.org/10.1093/jpepsy/jsn093 [ Links ]
16. Saps M, Moreno-Gómez JE, Ramírez-Hernández CR, Rosen JM, Velasco-Benítez CA. A nationwide study on the prevalence of functional gastrointestinal disorders in school-children. Bol Med Hosp Infant Mex. 2017;74(6):407-12. https://doi.org/10.1016/j.bmhimx.2017.05.005 [ Links ]
17. Cunningham NR, Cohen MB, Farrell MK, Mezoff AG, Lynch-Jordan A, Kashikar-Zuck S. Concordant parent-child reports of anxiety predict impairment in youth with functional abdominal pain. J Pediatr Gastroenterol Nutr . 2013;60(3):312-7. https://doi.org/10.1097/MPG.0000000000000625 [ Links ]
18. Rutten JMTM, Benninga MA, Vlieger AM. IBS and FAPS in children: A comparison of psychological and clinical characteristics. J Pediatr Gastroenterol Nutr . 2014;59(4):493-9. https://doi.org/10.1097/MPG.0000000000000452 [ Links ]
19. Gulewitsch MD, Weimer K, Enck P, Schwille-Kiuntke J, Hautzinger M, Schlarb AA. Stress reactivity in childhood functional abdominal pain or irritable bowel syndrome. Eur J Pain. 2017;21(1):166-77. https://doi.org/10.1002/ejp.914 [ Links ]
20. Waters AM, Schilpzand E, Bell C, Walker LS, Baber K. Functional gastrointestinal symptoms in children with anxiety disorders. J Abnorm Child Psychol. 2013;41(1):151-63. https://doi.org/10.1007/s10802-012-9657-0 [ Links ]
21. Pollard KL, Campbell C, Squires M, Palsson O, van Tilburg MAL. Seasonal Association of Pediatric Functional Abdominal Pain Disorders and Anxiety. J Pediatr Gastroenterol Nutr . 2018;67(1):18-22. https://doi.org/10.1097/MPG.0000000000001886 [ Links ]
22. Shelby GD, Shirkey KC, Sherman AL, Beck JE, Haman K, Shears AR, Horst SN, Smith CA, Garber J, Walker LS. Functional abdominal pain in childhood and long-term vulnerability to anxiety disorders. Pediatrics . 2013;132(3):475-82. https://doi.org/10.1542/peds.2012-2191 [ Links ]
23. Cunningham NR, Jagpal A, Peugh J, Farrell MK, Cohen MB, Mezoff AG, Lynch-Jordan A, Kashikar-Zuck S. Risk categorization predicts disability in pain-associated functional gastrointestinal disorders after 6 months. J Pediatr Gastroenterol Nutr . 2017;64(5):685-90. https://doi.org/10.1097/MPG.0000000000001342 [ Links ]
Received: June 17, 2019; Accepted: August 19, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
