










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista colombiana de Gastroenterología
Print version ISSN 0120-9957On-line version ISSN 2500-7440
Rev. colomb. Gastroenterol. vol.35 no.4 Bogotá Oct./Dec. 2020 Epub July 12, 2021
https://doi.org/10.22516/25007440.460
Case report
Megaesophagus as a complication of achalasia: Case report and narrative literature review
1
*
 http://orcid.org/0000-0001-9804-8990
http://orcid.org/0000-0001-9804-8990
1
http://orcid.org/0000-0002-9085-1719
2
http://orcid.org/0000-0002-9219-4548
2
http://orcid.org/0000-0001-5660-6229
2
http://orcid.org/0000-0002-4523-7947
1Departamento de Medicina Interna, Hospital Universitario San Ignacio. Pontificia Universidad Javeriana. Bogotá DC, Colombia.
2Unidad de Gastroenterología y Endoscopia Digestiva, Hospital Universitario San Ignacio. Departamento de Medicina Interna, Pontificia Universidad Javeriana. Bogotá DC, Colombia.
Megaesophagus occurs in between 5% and 20% of patients with achalasia. It is a primary esophageal motor disorder that has been known for more than 300 years. It should be considered in all patients with dysphagia that is not explained by an obstructive or inflammatory process after a detailed endoscopic study. The following is the case of a patient with progressive dysphagia, in whom megaesophagus was documented as a complication of untreated, long-standing achalasia. Chagas disease was ruled out by enzyme immunoassay (ELISA) and indirect immunofluorescence (IF), as recommended by current guidelines. Given the low frequency of this entity in our environment and the therapeutic implications for patients with achalasia, a narrative literature review was carried out to describe its diagnosis and treatment alternatives.
Keywords: Achalasia; Dysphagia; Esophageal motility; High-resolution manometry; Megaesophagus
El megaesófago se presenta entre el 5 % y el 20 % de pacientes con acalasia, un trastorno motor esofágico primario reconocido hace más de 300 años, a considerarse en todo paciente con disfagia no explicada por un proceso obstructivo o inflamatorio luego de un estudio endoscópico detallado. Se presenta el caso de un paciente con disfagia progresiva, en quien se documentó megaesófago como complicación de una acalasia de largo tiempo de evolución, no tratada. Se descartó la enfermedad de Chagas mediante enzimoinmunoensayo (ELISA) e inmunofluorescencia indirecta (IFI), tal como recomiendan las guías actuales. Ante la baja frecuencia de esta entidad en nuestro medio y las implicaciones terapéuticas que tiene para los pacientes con acalasia, se realizó una revisión narrativa en la literatura sobre su diagnóstico y alternativas de manejo.
Palabras clave: Acalasia; disfagia; motilidad esofágica; manometría de alta resolución; megaesófago
Introduction
Achalasia is a primary esophageal motor disorder and a rare condition with an annual incidence of 1/100 000 people1,2. It is an acquired degenerative disease characterized by the selective loss of inhibitory neurons of the myenteric plexus that causes motor disorders of the esophagus secondary to lack of lower esophageal sphincter relaxation (hence its name: a: “not”, chalasia: “relaxation”). Little more than 5% of these patients will undergo esophagectomy in advanced stages of the disease, with varying outcomes in terms of symptomatic improvement and long-term prognosis3. The following is the case of a patient with megaesophagus and long-standing achalasia.
Case presentation
A 42-year-old male driver, with no relevant medical history, consulted due to 3 years of progressive dysphagia initially for solids and then for liquids, and regurgitation, with a worsening of symptoms in the last 4 months associated with a weight loss of 15 kg (Eckardt score 9). On admission, the patient showed signs of severe malnutrition and halitosis, without dyspnea, peripheral lymphadenopathy, visceromegaly, or ascites. A nasogastric intubation was carried out, obtaining abundant food drainage. A chest x-ray was performed in which an apparent mediastinal mass displacing the midline was observed (Figure 1). In view of this finding and persistent dry cough, an enhanced chest computed tomography (CT) scan was performed, in which megaesophagus and suggestive findings of achalasia were reported, but no neoplastic involvement of the gastroesophageal junction could be ruled out (Figure 2).
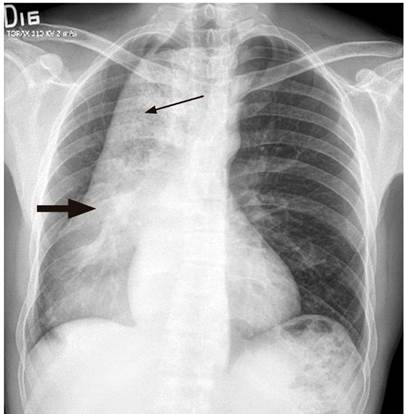
Figure 1 Chest x-ray, posteroanterior (PA) view. Mediastinal mass extending to the right and posterior to the mediastinum (thick arrow). Irregular air-fluid level and heterogeneous opacity content suggestive of food (thin arrow). Source: Gastroenterology Unit. Hospital Universitario San Ignacio. Bogotá D.C. Colombia.
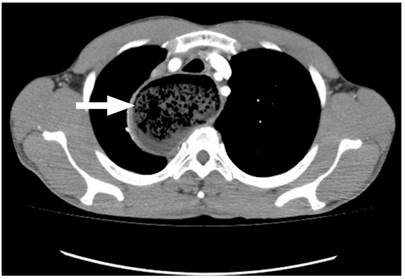
Figure 2 Enhanced chest CT scan. Esophageal dilation, with a maximum transverse diameter of 7 cm, with tortious margins. Heterogeneous material suggestive of food content (thick arrow). Source: Gastroenterology Unit. Hospital Universitario San Ignacio. Bogotá D.C. Colombia.
During the esophagogastroduodenoscopy, traces of food content were found in the esophagus. The esophageal body was severely dilated, tortuous, with angulations, and the gastroesophageal junction was punctiform, although it was difficult to pass through (Figure 3). Barium esophagogram revealed a severely dilated esophageal body, with the lower esophagus in a sigmoid-likepattern (Figure 4).
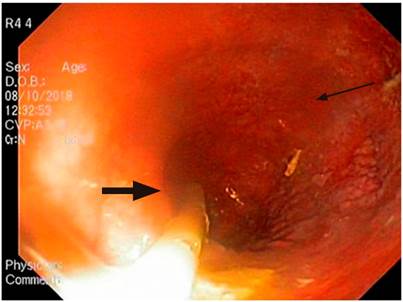
Figure 3 Esophagogastroduodenoscopy (upper GI endoscopy or EGD). Proximal esophagus with increased luminal caliber, nasogastric tube and undigested food remains (thick arrow). Congested mucosa with no stigmata of recent hemorrhage (thin arrow). Source: Gastroenterology Unit. Hospital Universitario San Ignacio. Bogotá D.C. Colombia.
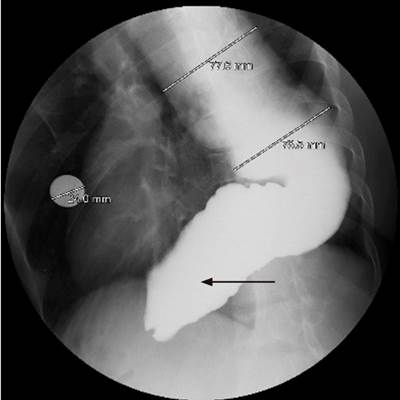
Figure 4 Barium esophagogram. Gastroesophageal junction below the left hemidiaphragm, which shows an alteration in lower esophageal sphincter relaxation that causes delayed gastric emptying. Sigmoid appearance of distal esophagus (thin arrow). Source: Gastroenterology Unit. Hospital Universitario San Ignacio. Bogotá D.C. Colombia.
Subsequently, a high-resolution esophageal manometry with impedancometry was performed (Figure 5), finding evidence of 100% failed waves (distal contractile integral [DCI] less than 100 mm Hg/s/cm), elevated integrated relaxation pressure (IRP) greater than 15 mm Hg, upper esophageal sphincter with adequate pharyngoesophageal coordination and incomplete bolus clearance in 100 % of the evaluated swallows, which was interpreted as type I or classic achalasia.
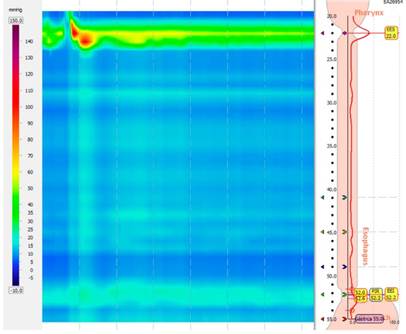
Figure 5 High-resolution manometry. Type I or classic achalasia (with elevated IRP greater than 15 mm Hg and 100 % failed swallowing). Source: Gastroenterology Unit. Hospital Universitario San Ignacio. Bogotá D.C. Colombia.
Enteral nutrition was initiated to cover basal caloric requirements. In order to rule out Chagas disease as an etiology, indirect immunofluorescence (IF) and enzyme immunoassay (ELISA) tests were performed, both of which were negative for the chronic phase of the disease and, most importantly, did not reveal any risk factors for it. The case was presented to an interdisciplinary board (gastrointestinal surgery, clinical gastroenterology), where it was decided that esophagectomy was the best treatment option for this patient. So far, he has had an acceptable progress, with tolerance to soft diet and improvement of his nutritional status.
Discussion
Achalasia is most common between the fifth and sixth decades of life, but can occur at any age, with no difference between sexes. It progresses slowly, with an average duration between 5 and 6 years, being dysphagia the main symptom4.
The pattern of dysphagia in patients with dilated esophagus is unique5, and the passage of food often improves by swallowing fluids or by performing maneuvers such as bending the legs, standing up or jumping. Weight loss can be massive and nocturnal regurgitation can be significant and accompanied by respiratory symptoms such as aspiration and chronic cough6.
The effects of the disease become apparent as the disease progresses. Esophagus dilation with retained food and the presence of air-fluid level on chest x-ray are usually late findings7,8.
In certain cases, diagnosis is usually delayed due to the existing association with reflux disease symptoms since up to 47% of patients have heartburn8-10. Moreover, since the fermentation of the retained food produces lactic acid, monitoring esophageal pH can lead to false positive results. For this reason, esophageal pH monitoring is not recommended on a regular basis11. Functional studies such as esophagogram and high-resolution esophageal manometry (HRM) have the highest diagnostic performance1,2,12,13.
Defined manometric characteristics are aperistalsis and incomplete relaxation of the lower esophageal sphincter (LES); elevated lower esophageal sphincter pressure and esophageal pressurization may also be found1,2,8. The absence of peristalsis is absolutely necessary for diagnosing achalasia, and while it may be absent, incomplete relaxation is normally present14. From a manometric point of view, aperistalsis should be differentiated from other causes, such as scleroderma esophagus, post-fundoplication or Barrett’s esophagus, which makes it important to cross-examine the patient’s medical history to achieve this differentiation. Figure 6 presents a practical algorithm for the classification of esophageal HRM according to the Chicago Classification v3.015.
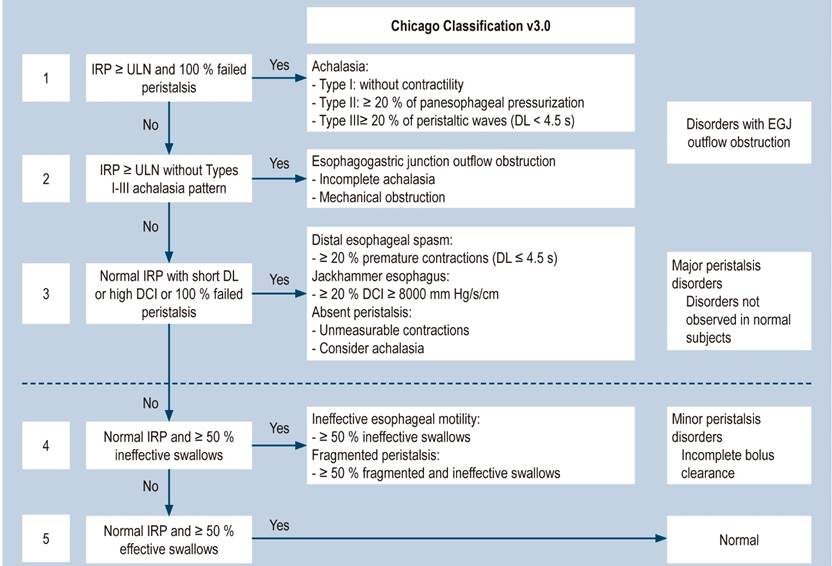
Figure 6 Algorithm for the interpretation of esophageal HRM according to the Chicago Classification v3.015. Taken from: Hani A et al. Rev Colomb Gastroenterol. 2017;32(4):369-378.
The esophagogram of a patient with end-stage achalasia or megaesophagus shows contrast agent retention in a dilated, tortuous esophagus, in both sagittal and coronal view.
Regarding treatment, no therapy can restore muscle activity in a denervated esophagus. Medical therapy is not recommended16,17. Botulinum toxin should be used in patients who are not suitable for more invasive procedures18-20 and other procedures (graduated pneumatic dilation, per-oral endoscopic myotomy [POEM], and laparoscopic Heller myotomy with anti-reflux surgery) are thought to have a similar efficacy. The decision regarding the type of treatment should be based on the patient’s age and characteristics, the type of achalasia on high-resolution manometry, the patient’s preference and the center’s experience. Pneumatic dilation21 is probably less effective in rare forms of achalasia (type 3), which is associated with reduced gastroesophageal junction distensibility and esophageal spasms that may persist after dilation.
Surgical myotomy is reserved for patients who do not respond to dilation22, typically after three attempts. Improvement is achieved in 65% to 90% of cases after performing this procedure, with an average of 80%23.
Megaesophagus, also known as sigmoid esophagus, results from chronic dilatation of the esophagus24. In this group of patients, there seems to be a higher prevalence of Chagas disease, especially in the American continent, condition that was ruled out in our patient25.
Approximately 5% of patients with achalasia progress to end-stage disease or megaesophagus, requiring surgery; this incurable disease is often characterized by obstructive symptoms despite treatment or may progress to marked esophageal dilation with loss of distal morphologic configuration. Surgical therapy in these patients is challenging given their significant altered anatomy.
Orringer and Stirling26 defined megaesophagus as an esophagus with a diameter greater than or equal to 8 cm as evidenced on a barium study, and advanced achalasia is considered in patients with more than 7 cm of esophageal dilation, findings of esophagus usually tortuous, manometrically weak and without contractions. Other authors use distal angulation and sigmoid configuration as predictors of myotomy failure due to the impossibility of achieving a permissive esophageal pressure gradient for emptying, thus confirming that there is no universally accepted criterion for defining it. In these cases, surgical resection is believed to be the treatment of choice, as happened in the case presented here, taking into account that megaesophagus is a dysfunctional organ and a potential source of gastroesophageal reflux disease, retention esophagitis, tracheobronchial aspiration, and development of neoplasms27,28.
Panda and Morse, from the Division of Thoracic Surgery at Harvard Medical School29, suggest the following objectives to be achieved when performing an esophagectomy:
To relieve intractable obstructive symptoms.
To restore food tract transit and, thereby, improve nutrition and reduce the risk of aspiration.
To remove a dysfunctional megaesophagus, in which stasis predisposes to esophagitis and malignancy.
Esophagectomy with esophageal replacement remains the surgical treatment of choice for patients with end-stage achalasia who have failed to respond to conservative treatment. In general, it is effective in improving the patient’s symptoms and its low morbidity and mortality will depend on the experience of the center where it is performed.
On the other hand, the experience from the POEM procedure in Greek patients30 shows that this technique was successful in 2 patients over 74 and 92 years of age with a diagnosis of megaesophagus, with previous anterior POEM without symptom improvement and who underwent posterior POEM, with significant clinical improvement of symptoms; however, there are few studies on the performance of POEM in this type of patient. In Brazil, studies addressing megaesophagus cases treated with POEM are mostly focused on Chagas disease patients31. Table 1 summarizes the therapeutic alternatives in patients with achalasia, taking into account the average time of success of each intervention.
Table 1 Summary of therapeutic alternatives for achalasia3
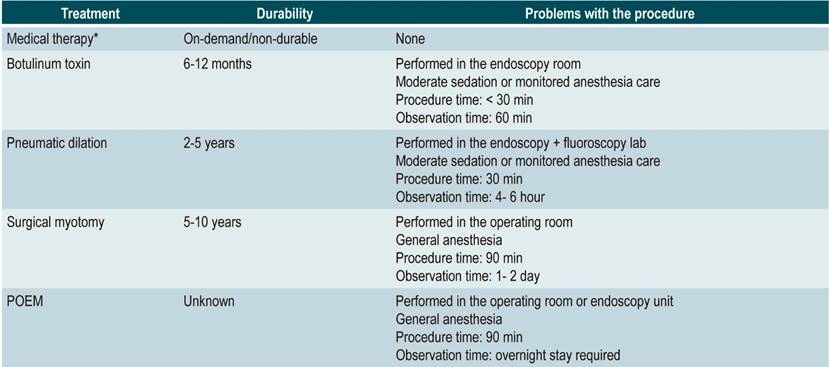
*Oral calcium antagonists (nifedipine), isosorbide dinitrate, sildenafil. Taken from: Pandolfino JE et al. JAMA. 2015;313(18):1841-1852.
Conclusion
Most cases of achalasia can be treated conservatively with pneumatic dilation, Heller myotomy, or POEM; however, esophagectomy is often needed in patients with megaesophagus. Few studies have shown the success of POEM in megaesophagus or end-stage achalasia cases, which also includes Chagasic megaesophagus, a condition that must be ruled out in Latin America.
REFERENCES
1. Oude Nijhuis RAB, Zaninotto G, Roman S, Boeckxstaens GE, Fockens P, Langendam MW, Plumb AA, Smout A, Targarona EM, Trukhmanov AS, Weusten B, Bredenoord AJ. European guidelines on achalasia: United European Gastroenterology and European Society of Neurogastroenterology and Motility recommendations. United European Gastroenterol J. 2020;8(1):13-33. https://doi.org/10.1177/2050640620903213 [ Links ]
2. Mion F. Achalasia guideline: another step towards standardization of its management. United European Gastroenterol J. 2020,8(1):9-10. https://doi.org/10.1177/2050640620902570 [ Links ]
3. Pandolfino JE, Gawron AJ. Achalasia: a systematic review. JAMA. 2015;313(18):1841-1852. https://doi.org/10.1001/jama.2015.2996 [ Links ]
4. Enestvedt BK, Williams JL, Sonnenberg A. Epidemiology and practice patterns of achalasia in a large multi-centre database. Aliment Pharmacol Ther. 2011;33(11):1209-1214. https://doi.org/10.1111/j.1365-2036.2011.04655.x [ Links ]
5. Katz PO, Dalton CB, Richter JE, Wu WC, Castell DO. Esophageal testing of patients with non-cardiac chest pain or dysphagia. Ann Intern Med. 1987;106(4):593-597. https://doi.org/10.7326/0003-4819-106-4-593 [ Links ]
6. Bhattacharyya N. The prevalence of dysphagia among adults in the United States. Otolaryngol Head Neck Surg. 2014;151(5):765-769. https://doi.org/10.1177/0194599814549156 [ Links ]
7. Sonnenberg A. Hospitalization for achalasia in the United States 1997-2006. Dig Dis Sci. 2009;54(8):1680-1685. https://doi.org/10.1007/s10620-009-0863-8 [ Links ]
8. Khashab MA, Vela MF, Thosani N, Agrawal D, Buxbaum JL, Abbas Fehmi SM, Fishman DS, Gurudu SR, Jamil LH, Jue TL, Kannadath BS, Law JK, Lee JK, Naveed M, Qumseya BJ, Sawhney MS, Yang J, Wani S. ASGE Guideline on the management of achalasia. Gastrointest Endosc. 2020;91(2):213-227. https://doi.org/10.1016/j.gie.2019.04.231 [ Links ]
9. Spechler SJ, Souza RF, Rosenberg SJ, Ruben RA, Goyal RK. Heartburn in patients with achalasia. Gut. 1995;37(3):305-308. https://doi.org/10.1136/gut.37.3.305 [ Links ]
10. Smart HL, Mayberry JF, Atkinson MK. Achalasia following gastroesophageal reflux. J R Soc Med. 1986;79(2):71-73. https://doi.org/10.1177/014107688607900204 [ Links ]
11. Smart HLO, Foster PN, Evans DF, Slevin B, Atkinson M. Twenty four hour oesophageal acidity in achalasia before and after pneumatic dilatation. Gut. 1987;28(7):883-7. https://doi.org/10.1136/gut.28.7.883 [ Links ]
12. Fox M, Hebbard G, Janiak P, Brasseur JG, Ghosh S, Thumshirn M, Fried M, Schwizer W. High-resolution manometry predicts the success of oesophageal bolus transport and identifies clinically important abnormalities not detected by conventional manometry. Neurogastroenterol Motil. 2004;16(5):533-542. https://doi.org/10.1111/j.1365-2982.2004.00539.x [ Links ]
13. Pandolfino JE, Ghosh SK, Zhang Q, Jarosz A, Shah N, Kahrilas PJ. Quantifying EGJ morphology and relaxation with high-resolution manometry: a study of 75 asymptomatic volunteers. Am J Physiol Gastrointest Liver Physiol. 2006;290(5):G1033-G1040. https://doi.org/10.1152/ajpgi.00444.2005 [ Links ]
14. Zaninotto G, Bennett C, Boeckxstaens G, Costantini M, Ferguson MK, Pandolfino JE, Patti MG, Ribeiro U Jr, Richter J, Swanstrom L, Tack J, Triadafilopoulos G, Markar SR, Salvador R, Faccio L, Andreollo NA, Cecconello I, Costamagna G, da Rocha JRM, Hungness ES, Fisichella PM, Fuchs KH, Gockel I, Gurski R, Gyawali CP, Herbella FAM, Holloway RH, Hongo M, Jobe BA, Kahrilas PJ, Katzka DA, Dua KS, Liu D, Moonen A, Nasi A, Pasricha PJ, Penagini R, Perretta S, Sallum RAA, Sarnelli G, Savarino E, Schlottmann F, Sifrim D, Soper N, Tatum RP, Vaezi MF, van Herwaarden-Lindeboom M, Vanuytsel T, Vela MF, Watson DI, Zerbib F, Gittens S, Pontillo C, Vermigli S, Inama D, Low DE. The 2018 ISDE achalasia guidelines. Dis Esophagus. 2018 Sep 1;31(9). https://doi.org/10.1093/dote/doy071 [ Links ]
15. Hani A, Bernal W, Leguízamo AM, Zuluaga C, Vargas R, Vergara H, Ardila Hani A, Costa V. Cómo realizar e interpretar una manometría esofágica de alta resolución usando la clasificación de Chicago 3.0. Rev Colomb Gastroenterol. 2017;32(4):369-378. https://doi.org/10.22516/25007440.181 [ Links ]
16. Wong RK, Maydonovitch CL, Garcia JE, Johnson LF, Castell DO. The effect of terbutaline sulfate, nitroglycerin, and aminophylline on lower esophageal sphincter pressure and radionuclide esophageal emptying in patients with achalasia. J Clin Gastroenterol. 1987;9(4):386-9. https://doi.org/10.1097/00004836-198708000-00006 [ Links ]
17. Dimarino AJ, Cohen S. Effect of an oral beta2-adrenergic agonist on lower esophageal sphincter pressure in normal subjects and in patients with achalasia. Dig Dis Sci. 1982;27(12):1063-6. https://doi.org/10.1007/BF01391441 [ Links ]
18. Pamphlett R. Early terminal and nodal sprouting of motor axons after botulinum toxin. J Neurol Sci 1989;92(2-3):181-92. https://doi.org/10.1016/0022-510X(89)90135-4 [ Links ]
19. Annese V, Basciani M, Perri F, Lombardi G, Frusciante V, Simone P, Andriulli A, Vantrappen G. Controlled trial of botulinum toxin injection versus placebo and pneumatic dilation in achalasia. Gastroenterology. 1996;111(6):1418-24. https://doi.org/10.1016/S0016-5085(96)70002-1 [ Links ]
20. Pasricha PJ, Rai R, Ravich WJ, Hendrix TR, Kalloo AN. Botulinum toxin for achalasia: long-term outcome and predictors of response. Gastroenterology. 1996;110(5):1410-5. https://doi.org/10.1053/gast.1996.v110.pm8613045 [ Links ]
21. Vaezi MF, Richter JE, Wilciox CM, Schroeder PL, Birgisson S, Slaughter RL, Koehler RE, Baker ME. Botulinum toxin versus pneumatic dilatation in the treatment of achalasia: a randomised trial. Gut. 1999;44(2):231-9. https://doi.org/10.1136/gut.44.2.231 [ Links ]
22. Cheung W-K, Ho M-P, Chou A-H. Delayed discovery and diagnosis of achalasia resulting in megaesophagus in an elderly nursing home resident. J Am Geriatr Soc. 2015;63(1):201-3. https://doi.org/10.1111/jgs.13219 [ Links ]
23. Campos GM, Vittinghoff E, Rabl C, Takata M, Gadenstätter M, Lin F, Ciovica R. Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Ann Surg. 2009;249(1):45-57. https://doi.org/10.1097/SLA.0b013e31818e43ab [ Links ]
24. Maiti A, Bhattacharjee M. Megaesophagus in Achalasia. Am J Med Sci. 2016;351(5):549. https://doi.org/10.1016/j.amjms.2016.02.039 [ Links ]
25. Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management of achalasia. Am J Gastroenterol. 2013;108(8):1238-49; quiz 1250. https://doi.org/10.1038/ajg.2013.196 [ Links ]
26. Orringer MB, Stirling MC. Esophageal resection for achalasia: indications and results. Ann Thorac Surg. 1989;47(3):340-5. https://doi.org/10.1016/0003-4975(89)90369-X [ Links ]
27. Molena D, Yang SC. Surgical management of end-stage achalasia. Semin Thorac Cardiovasc Surg. 2012;24(1):19-26. https://doi.org/10.1053/j.semtcvs.2012.01.015 [ Links ]
28. Bazerbachi F, Blackmon SH, Ravi K, Song LMWK. Endoscopic esophagoplasty for megaesophagus with sump stasis in end-stage achalasia. Videogie. 2017;2(10):274-5. https://doi.org/10.1016/j.vgie.2017.07.008 [ Links ]
29. Panda N, Morse CR. Esophagectomy for end-stage achalasia. J Xiangya Med. 2019;(7):1-6. https://doi.org/10.21037/jxym.2019.01.04 [ Links ]
30. Eleftheriadis N, Eleftheriadou ED. Successful peroral endoscopic myotomy performed in Endoscopy Deparment as a radical long-term treatment for esophageal achalasia -The Greek experience. Ther Clin Risk Manag. 2017;13:185-190. https://doi.org/10.2147/TCRM.S127111 [ Links ]
31. Hourneaux de Moura ET, Hourneaux de Moura EG. Endoscopic pneumatic dilatation and peroral endoscopic myotomy in dilated megaesophagus. Mini-invasive Surg. 2017;1:148-152. https://doi.org/10.20517/2574-1225.2017.27 [ Links ]
Citation: Rondón-Carvajal J, Ardila-Hani C, Hani-Ardila A, Vargas-Rubio R, Leguízamo-Naranjo AM, Cañadas-Garrido R, Puentes-Leal G. Megaesophagus as a complication of achalasia: Case report and narrative literature review. Rev Colomb Gastroenterol. 2020;35(4):551-557. https://doi.org/10.22516/25007440.460
Ethical responsibility Protection of people and animals. Authors of this report state that no experiments were carried out on humans or animals in the making of this study.
Data confidentiality Authors of this report state that this article does not contain any data of the patient.
Right to privacy and informed consent Authors of this report state that this article does not contain any data of the patient.
Received: September 02, 2019; Accepted: April 23, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
