











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Appendiceal intussusception is defined as the partial or complete invagination of the appendix and its corresponding mesentery within the adjoining intestinal lumen. In 1958, McKidd reported the first case in the literature, involving a 7-year-old patient.1 It is a rare condition with few cases reported in the literature, with an incidence of 0.01 % according to a cohort study conducted by Collins, which included 71 000 patients who underwent appendectomy over a 40-year period.2,3 It is most common in women in the fourth or fifth decades of life. Diagnosing this condition is difficult due to its non-specific symptoms and low incidence. The purpose of this publication is to present a case treated at our institution.
Case report
This is the case of a 43-year-old female patient with a history of a low-grade neuroendocrine tumor in the upper rectum, resected endoscopically 3 years earlier, who was undergoing clinical and endoscopic follow-up. She was completely asymptomatic but, during her the last total colonoscopy, a lesion of 2 cm in size was found at the level of the meatus of the appendix (Figure 1). A biopsy of the lesion was performed, revealing normal-looking mucosa with no signs suggesting malignancy or other pathological changes. CT scan of the abdomen and pelvis, as well as 5-hydroxyindoleacetic acid levels were normal. Her clinical examination was normal.

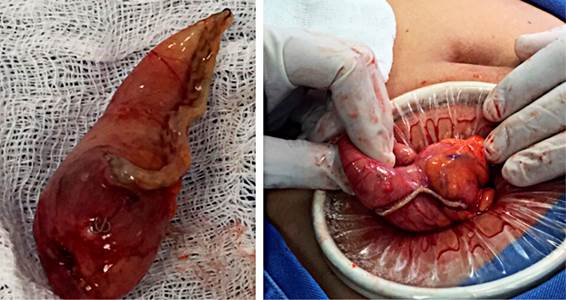
Although the histopathological study was inconclusive, it was decided to perform minimally invasive surgery. Surgery was started with a laparoscopy in which no cecal appendix was observed; a Rockey Davis incision was then made using an Alexis wound retractor to expose the cecum. Appendicular invagination was confirmed through palpation and visualization (Figure 2).

A cecectomy was performed using a mechanical linear cutter and the specimen was sent to pathology (Figure 3). Postoperative evolution was adequate and without complications. Pathology confirmed invagination secondary to foci of endometriosis (Figure 4).

During postoperative follow-up, it was possible to obtain the report of the colonoscopy performed 3 years earlier when the neuroendocrine tumor in the rectum was treated, with a report of cecum and meatus of the appendix within normal limits, although without photographic documentation.
Discussion
The pathophysiology of this condition is unknown; however, it is associated with the presence of appendix alterations, most notably a mass at that level. Altered peristalsis is thought to occur and is associated with inflammation, foreign body, Crohn’s disease, parasites, polyps, lymphoid hyperplasia, ecchymoses, mucosa-associated lymphoid tissue lymphoma (MALT), adenoma, papilloma, adenocarcinoma, endometriosis, and mucocele4-7; the latter 2 are the main causes of invagination in adults, while inflammatory processes are the most common in children8-10.
Given its low incidence and the multiple and unspecific symptoms, the diagnosis of this condition poses a challenge for physicians. Three types of symptoms have been described in these patients:
symptoms of typical acute appendicitis;
nonspecific symptoms of intussusception (severe abdominal pain, vomiting, diarrhea, and melena); and
sensation of a mass, pain in the lower right quadrant, and melena for several months.
Most patients are asymptomatic with incidental findings during colonoscopy, which can also be found intraoperatively (57 %) or by pathology (11 %)1,7,8,11.
Regarding its etiology, the most common cause of appendiceal intussusception in adults is endometriosis, a benign entity first described in 1860 by Von Rokitansky12. It is defined as the presence of endometrial glands and stroma outside the uterine cavity. Between 10 % and 15 % of women suffer from endometriosis.11,13-15. The rectum and sigmoid colon are the main sites of intestinal implantation, followed by the ascending colon, small intestine, and appendix, which is observed in 0.08 % to 8 % of cases (Figure 5)8,10,12,16.

Histologically, it is characterized by the presence of endometrial glands and stroma, which may be associated with macrophages. Atypical benign changes include necrotic pseudoxanthomatous nodules; vascular, perineural and nodal involvement; and metaplastic changes in both glands and stroma. In addition, it may contain premalignant changes such as polypoid endometriosis, stromal endometriosis, mesothelial hyperplasia associated with endometriosis, and atypical endometriosis with a 1% risk of conversion to cancer15.
The diagnostic methods used include enhanced abdominal tomography and colon enema, followed by ultrasound, which is very useful in the pediatric population. In colonoscopies performed in adults for various reasons, it is described as a pseudopedunculated polyp17-19 or mass in the meatus of the appendix, as in this case. No more than 200 cases have been reported in the literature; however, it is impossible to know the incidence of this finding. If it is approached as a polypoid lesion, performing a polypectomy may lead to the risk of perforation and peritonitis20. It is important to bear this entity in mind when evaluating lesions at the meatus of the appendix. To this end, a report by McSwain proposed a classification of intussusception depending on the anatomy found, simplified years later by Langsman17,21:
Type I: invagination of the tip of the appendix into the proximal appendix,
Type II: invagination begins at any point of the appendix other than the tip and base of the appendix,
Type III: invagination begins at the appendicular base into the most distal part of the cecum,
Type IV: retrograde invagination of a proximal segment within a distal segment of the same appendix,
Type V: complete invagination of the appendix into the cecum (as in this case).
Surgical treatment is the standard management, considering that there is always the probability of a malignant disease causing the intussusception. In most cases, patients are taken to cecectomy, but some cases may undergo a right hemicolectomy22. Endometriosis is the most common cause described in the reports of the last 10 years.
This case illustrates this disease very well. However, two more cecectomies with appendicular invagination secondary to endometriosis were performed in the following two years on the service, implying that the frequency is not as low as reported in the literature. For this reason, appendicular intussusception should be listed as one of the differential diagnoses of lesions in the meatus of the appendix.

