











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Cystic Intestinal pneumatosis is defined as the presence of cyst-like lesions in the intestinal wall and is divided into two categories: life-threatening intestinal pneumatosis and benign intestinal pneumatosis1. It has a low incidence and its etiology is unclear; besides an incidence of 3 cases per 10 000 individuals has been estimated in the general population2. The average age of onset is 45.3 ± 15.6 years, the mean course of the disease is 6 months, and a male to female ratio occurrence of 2.4: 1 have been described3. Risk factors associated with its development include the use of certain drugs, the presence of gastrointestinal conditions such as Crohn’s disease, ulcerative colitis, and other non-gastrointestinal diseases such as chronic obstructive pulmonary disease (COPD); in addition, idiopathic intestinal pneumatosis accounts for only 15% of cases4.
As for its pathophysiology, three possibilities have been proposed as a source of gas: intraluminal gastrointestinal gas, bacterial gas production and pulmonary gas. The first theory occurs due to increased intraluminal pressure in the context of mucosal barrier injury. The second theory involves colonization of gas-producing bacteria in intramural compartments due to mucosal involvement; these bacteria produce hydrogen tensions that exceed blood nitrogen pressures, leading to a hydrogen diffusion gradient into the submucosal vessels. The last theory proposes that alveolar rupture could cause gas dissection into the vascular channels of the mediastinum, tracking caudally to the retroperitoneum and then to the mesentery of the bowel5.
It has a nonspecific clinical presentation. Patients may be asymptomatic or present with abdominal pain, intestinal obstruction, diarrhea, hematochezia and tenesmus1,2. The clinical case of a 35-year-old patient with no relevant history of disease who presented with surgical acute abdomen and was taken to surgery, where a cystic intestinal pneumatosis was identified.
Clinical case
This is the case of a 35-year-old man who sought medical assistance due to having experienced a nonspecific and high intensity lower abdominal pain that radiated to the right lumbar region, without clinical signs of acute abdomen, for one month. He was initially diagnosed with urinary tract infection and was treated with levofloxacin on an outpatient basis; however, provided that his condition did not improve, he sought for medical assistance again. A contrast enhanced CT scan of the abdomen showed segmental cystic intestinal pneumatosis in the splenic flexure of the colon associated with adjacent pneumoperitonea (Figure 1). He was assessed by the general surgery service, where laparoscopic management was started. A plastron with omentum and pneumatosis in the splenic flexure were found during the laparoscopy, thus it was suspended and a laparotomy was then performed, where a left hemicolectomy, a partial omentectomy and a left colostomy were carried out.
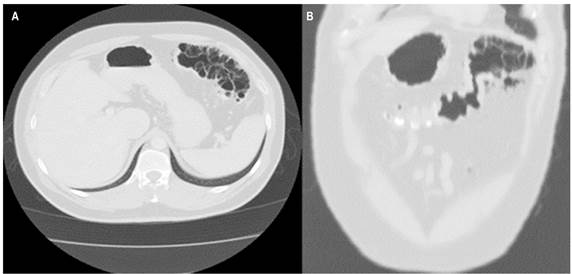
Figure 1 CT scan showing cystic intestinal pneumatosis in the splenic flexure of the colon, associated with multiple pneumoperitonea. A. Axial view. B. Coronal plane.
The surgical specimen was sent to the pathology service, where a 15 cm serous light brown colonic segment with diameters ranging from 2 to 4 cm and fully covered by a mesentery measuring up to 4 cm was recognized. More than 80% of the mucosa had been replaced by air cystic formations, being the largest 4.5 x 4 cm and the smallest, 2 x 1 cm; with a wall measuring 0.1 cm; these lesions, although smaller in size, were also be observed in the surrounding mesentery (Figure 2). In addition, multiple cystic lesions located in the submucosa and the muscularis propria were observed on microscopic analysis (Figure 3), together with foreign body-like multinucleated giant cells and macrophages (Figure 4). Lesions extended into the subserosa, where reactive mesothelial cells were also observed. These findings allowed confirming the cystic intestinal pneumatosis diagnosis.
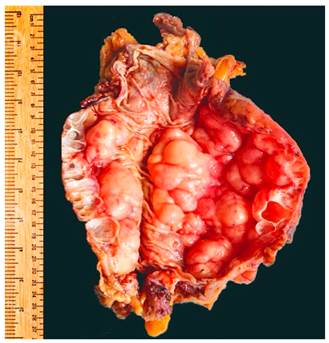
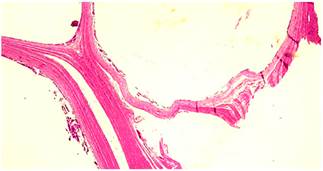
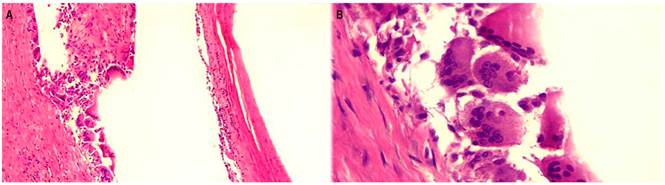
Figure 4 Histologically, cystic structures covered by foreign body-like multinucleated giant cells and mononuclear inflammatory infiltrate are evidenced. A. 4 X. B. 40 X.
In addition, the patient received antibiotic therapy with carbapenemics for 14 days as part of the treatment of secondary peritonitis, without requiring to undergo a new surgery. There was no recurrence of digestive tract symptoms or other symptoms in the months following the surgical procedure.
Discussion
Cystic intestinal pneumatosis is a rare disease characterized by the presence of cystic structures in the intestinal submucosa, the subserosa and the muscularis propria of any part of the gastrointestinal tract, most frequently in the colon3. More than 80% of cystic intestinal pneumatosis are considered to be iatrogenic; however, sometimes its occurrence is attributed to bacterial, metabolic or pulmonary factors, as well as to collagen tissue disorders, human immunodeficiency syndrome or the use of certain drugs such as glucocorticoids1,6, which causes and increased intraluminal pressure and forces the exit of gas through the altered mucosa. This in turn produces a tissue response that can be histologically evidenced by the presence of multinucleated giant cells associated with macrophages3, whose complications may require surgical management7.
Li-Li Wu et al.8, in a study that included 239 cystic intestinal pneumatosis cases, reported that the patients’ mean age was 45.3 ± 15.6 years, and that abdominal pain was the most common symptom (53.9 %), followed by diarrhea (53, 0 %), bloating (42.4 %), nausea and vomiting (14.3 %), rectorrhagia (12.9 %), mucous stools (12.0 %), constipation (7.8 %), and complications such as intestinal obstruction and perforation (16.3 %)8. Life-threatening conditions were associated with mesenteric ischemia, necrosis or intestinal obstruction; these patients showed clinical signs of sepsis and symptoms of shock, presented with acute abdomen and needed surgical management7. In conclusion, compared to asymptomatic patients, those who develop any complication have unfavorable outcomes2. On the other hand, Greenstein et al.9 described the following indications for surgical management: symptoms of obstruction (emesis, nausea, pain), more than 12 leukocytes per mm3, portal venous gas visualized on CT scan, and being older than 60 years; in addition, according to these authors, patients with lactate levels > 2.0 mmol/L and a primary abdominal process have a high mortality rate.
Traditionally, intestinal pneumatosis has been associated with a high mortality rate (20%)9. Morris et al.10, in a study conducted in 104 patients diagnosed with intestinal pneumatosis in a 7-year period by means of CT scan findings, reported a 22% mortality rate and found that imaging findings do not correlate with the severity of intestinal ischemia. They also reported that 56% patients underwent bowel resection due to ischemia and that the colon was most frequently involved (46%), followed by the small intestine (27%) and both, the small and large intestine (7%).
Macroscopically, intestinal pneumatosis is characterized by the presence of multiple cyst-like structures in the mucosa of the intestinal wall, sometimes such structures are described as cerebriform-like. Microscopically, cyst-like formations of variable size (from millimeters to a few centimeters) are observed on the mucosa, submucosa or the muscularis propria; histologically, these cyst-like formations are covered by macrophages, foreign body-like giant multinucleated cells and mononuclear inflammatory infiltrate3. Early cysts may be covered by endothelial cells, which can sometimes be interpreted as distension of lymphatic vessels11.
The content of the cysts consists of a mixture of nitrogen and hydrogen with variable amounts of oxygen, carbon dioxide, butane, propane, methane, ethane and argon, which generate a foreign body type inflammatory response mediated by multinucleated giant cells that express cluster of differentiation 68 (CD68) in complementary immunohistochemistry studies11.
In conclusion, cystic intestinal pneumatosis can be asymptomatic or life-threatening. In most cases, diagnosis is made based on imaging findings6, in which numerous porous-like cystic air areas are evidenced within the intestinal wall2, or based on endoscopic findings, where numerous cerebriform-like mucosal folds are visualized in the intestinal wall8. Its treatment must be focused on the underlying disease and severe complications such as mesenteric infarction, intestinal perforation and peritonitis, which must be surgically managed7; however, it is important to keep in mind that its prognosis varies depending on the symptoms and complications experienced by the patient. Diagnosis can often be difficult and requires an excellent clinical skill.

