











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Gastric volvulus is a rare condition characterized by abnormal rotation of the stomach along its long or short axis, leading to varying degrees of obstruction1.
Its incidence reaches its peak after the fifth decade of life and adults account for 80% to 90% of cases. No association with sex or race has been reported2.
Gastric volvulus is classified according to its duration (acute or chronic), etiology (primary or secondary) and the axis of rotation (organoaxial or mesenteroaxial).
Its symptoms are not specific; however, acute gastric volvulus has been associated with epigastric pain, nausea without vomiting and impossibility to advance the nasogastric tube (Borchardt’s triad), while chronic volvulus, with peptic ulcer disease or biliary tract-related diseases such as cholelithiasis3.
The following is the case of a nonagenarian patient who was admitted to our institution due to atypical chest pain, and in whom organoaxial gastric volvulus was documented as an incidental finding in the admission chest X-ray.
Case
This is the case of an 89-year-old woman patient with a history of osteoporosis and multiple vertebral fractures who visited our health institutions looking for medical assistance due to having experienced the following symptoms and signs during 4 days: nonradiating chest pain whose intensity increased with inspiration, together with dyspnea while in resting position. The patient did not refer experiencing any gastrointestinal symptom such as abdominal pain, nausea or emesis.
On physical examination on admission, the general condition of the patient was acceptable, agitation, tachycardia and diaphoresis were observed, as well as epigastric pain on deep palpation without signs of peritoneal irritation.
In a chest X-ray requested on admission due to suspicion of vertebral fracture, an ascending gastric chamber in the posterior mediastinum, associated with hydro-aerial level and suggestive of gastric volvulus was documented as an incidental finding (Figure 1).
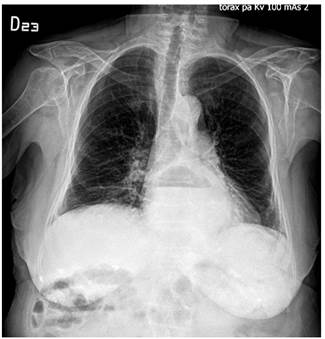
Figure 1 Chest X-ray: Ascending gastric chamber in the posterior mediastinum with hydro-aerial level.
Gastric decompression was started using a nasogastric tube, opioid administration was initiated for pain management, and intravenous hydration with isotonic fluids was started.
Subsequently, a contrast-enhanced CT scan of the chest and abdomen evidenced a hernia of the gastroesophageal junction, fundus and antropyloric region towards the thorax, as well as rotation of the stomach in its long axis, signs compatible with organoaxial gastric volvulus (Figure 2).
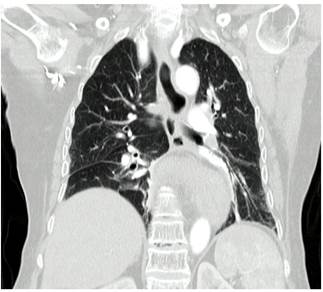
Figure 2 Contrast-enhanced CT scan: hernia of the gastroesophageal junction, fundus and antropyloric region towards the thorax and rotation of the stomach in its long axis.
Given these imaging findings, the advanced age of the patient and her comorbidities, which made her a high-risk surgical patient, endoscopic management was decided, thus an endoscopic devolvulation was performed without any complication (Figure 3).

However, gastric volvulus recurrence was detected in a control chest X-ray performed 24 hours after the endoscopic procedure.
In view of this recurrence, surgical management was decided together with the general surgery service: laparoscopic hiatal hernia repair surgery (laparoscopic hiatoplasty and Toupet fundoplication) and percutaneous gastrostomy fixation.
The procedure was performed without complications, with an adequate evolution of the patient’s condition during the postoperative period, tolerance to oral administration of food and improvement of thoracic pain. There was no evidence of recurrence in a control chest X-ray performed 72 hours after the surgical procedure.
Discussion
Gastric volvulus is a rare condition characterized by abnormal rotation of the stomach along its long or short axis, which leads to varying degrees of obstruction4.
Timely diagnosis and management determines the patient’s prognosis, since it can lead to intestinal obstruction, vascular involvement and even intestinal strangulation, which can progress to necrosis or perforation.
Around 70%-80% of gastric volvulus cases affect adults over 50 years of age and its occurrence is associated with predisposing factors such as phrenic nerve paralysis and some anatomical alterations of the diaphragm, abdominal organs or kyphoscoliosis5.
There are two main types of gastric volvulus: organoaxial, where rotation of the stomach on its vertical axis occurs, and mesenteroaxial, in which rotation occurs on the horizontal axis (Figure 4).
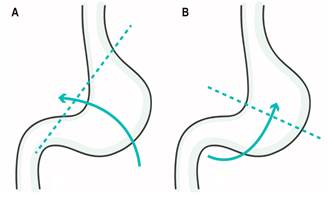
Figure 4 A. Organoaxial volvulus by rotation of the stomach on its longitudinal axis. B. Mesenteroaxial volvulus by rotation of the stomach on its transverse axis.
Primary (idiopathic) gastric volvulus is defined as a volvulus caused by abnormalities of the gastric ligaments. Gastric fixation failure may occur as a result of agenesis, elongation or injury of the gastric ligaments due to neoplasia, adhesions or skeletal deformity6,7.
Secondary volvulus is defined as a volvulus caused by other anatomical abnormalities such as paraesophageal hernia, diaphragmatic hernia, diaphragm eventration and phrenic nerve palsy.
The classic finding of acute gastric volvulus on plain X-rays of the abdomen is the presence of a gastric bubble or hydroaerial levels in the upper abdomen or the chest.
In mesenteroaxial volvulus, there may be two gastric bubbles (one in the fundus and the other in the antrum), while in organoaxial volvulus there is only one bubble and the stomach is in a horizontal position.
CT scan has the additional advantage of showing the relationship between the stomach and surrounding structures, as well as anatomical abnormalities associated with secondary gastric volvulus.
Usually, acute volvulus management requires, as it was the case of our patient, endoscopic decompression, initial endoscopic devolvulation, percutaneous endoscopic gastrostomy, gastropexy and repair of predisposing structural defects to prevent recurrence8. Yao-Chun Hsu et al., in a study in which 44 patients (median age of 71 years) with gastric volvulus who received conservative treatment in the presence of mild to moderate symptoms were followed-up for 36 months, reported that recurrence was observed in 64% cases and that none of the patients presented with acute complications during the follow-up period; however, laparoscopic surgery was required in one patient due to the presence of recurrent symptoms affecting the patient’s quality of life9,10. The average recurrence-free duration was 3 months and the factors associated with recurrence were longer duration between the onset of symptoms and (1.6 months; p=0.065), previous thoracic or abdominal surgery (p=0.061) and peritoneal adhesions (p=0.015)11.
On the other hand, it has been described that surgical management is superior to management based only on percutaneous endoscopic gastrostomy, as the latter does not prevent recurrence. Traditionally, gastric volvulus has been treated by means of surgery in combination with endoscopic techniques in some patients, including devolvulation alone or devolvulation plus one or two percutaneous gastrostomies12. In patients with organoaxial volvulus, endoscopic approach is limited by the obstruction at the gastroesophageal junction, which prevents safe passage of the gastroscope and in turn makes more difficult guiding the position of the stomach; in addition, endoscopic management does not address the diaphragmatic disease seen in most gastric volvulus cases.
Several surgical methods for treating gastric volvulus have been described, including diaphragmatic hernia repair, gastropexy, partial gastrectomy due to necrosis, antral fundus gastrogastrostomy (Opolzer’s operation) and gastropexy with fixation of the gastrocolic ligament (Tanner’s operation), among others.
Combined management (surgery plus preoperative or intraoperative percutaneous endoscopic gastrostomy) favors that the gastrostomy tube acts as the main anchor of the stomach to the anterior abdominal wall, which allows the laparoscopic repositioning of the gastropexy sutures to achieve an optimal anatomical position of the stomach along its natural axis; besides, it has been described there is no difference in terms of the efficacy of combined management between performing endoscopic gastrostomy prior to or during surgery. The passage of the gastroscope through the esophagogastric junction or the lack of endoscopic devolution is a limiting factor for preoperative endoscopic gastrostomy13.
Two techniques have been described to perform endoscopic devolvulation. First, the Alfa-loop maneuver, described by Tsang in 1995, which comprises six main steps, and in which an alpha loop is formed at the proximal end of the stomach affected by gastric volvulus by advancing the endoscope tip through the site of the stricture that produces the volvulus; subsequently the endoscope tip is brought into the duodenum by torquing the endoscope clockwise. Second, fluoroscopy based dual endoscopic technique, in which the adult gastroscope is brought into the duodenum, which favors the displacement of the stomach towards the abdominal cavity and the repositioning of the antrum maintaining its axis; then a pediatric gastroscope is passed next to the adult gastroscope and an endoscopic percutaneous gastrostomy is performed to fixate the anterior wall of the stomach to the abdominal wall14.
In our case, in view of the gastric volvulus recurrence despite endoscopic management, and with the intention of performing gastric fixation to avoid a new recurrence, together with the general surgery service, a surgical approach consisting of a hiatoplasty and a Toupet fundoplication, in addition to percutaneous gastrostomy for gastric fixation purposes, was decided, which allowed achieving complete devolvulation, absence of recurrence and an adequate evolution of the clinical condition of the patient.
Conclusion
Gastric volvulus is a rare condition with a spectrum of clinical presentation ranging from chronic course of the disease characterized by nonspecific symptoms to acute clinical presentation, with sudden onset of symptoms and a high risk of mortality.
Clinical suspicion and timely diagnosis based on imaging findings is of great importance, as imaging tests allow for the identification of this condition, as well as the mechanism causing it and associated complications. Early endoscopy is necessary and treatment with endoscopic or laparoscopic gastropexy is required as a less invasive and viable alternative to a more aggressive surgical procedure in some older adults with significant comorbidities.

