











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Appendiceal tumors are a rare entity with a reported incidence between 0.1% and 17%1. One of the main situations that slow down the diagnosis of this pathology is its similarity to appendicitis. The neoplasm obstructs the appendiceal orifice, leading to obstruction and an acute inflammatory process2. This is a concern as appendiceal tumors may go unnoticed, increasing their incidence.
Most of these cases are evidenced in appendectomies with atypical intrasurgical findings such as appendicular plastrons or masses with neoplastic characteristics non-consistent with appendicitis only3. Appendix neoplasms secondary to metastatic involvement are also less common. The literature reports that secondary malignant involvement of the appendix is, within these cases, more common due to the direct extension of colon carcinoma, pelvic neoplasms and less frequent due to distal metastasis4.
Case report
This is a 65-year-old male patient from Cartagena, Bolívar, Colombia. He consulted for a 15 day-of-evolution clinical picture consistent with abdominal pain in the right iliac fossa, jaundice, choluria, unintentional weight loss, and hyporexia.
The patient has no relevant pathological history. He has a surgical history of right inguinal herniorrhaphy without documented complications or previous pharmacological management. He was admitted with generalized abdominal pain (especially in the right iliac fossa), signs of peritoneal irritation, and generalized jaundice.
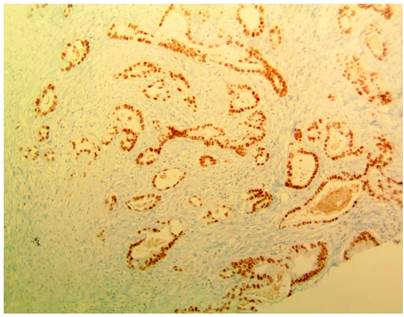
A laparoscopic appendectomy and biliary bypass by endoscopic retrograde cholangiopancreatography were required with the insertion of a biliary stent in the referral hospital. Intrasurgical finding of an appendicular plastron, abundant sallow peritoneal fluid, narrowing of the common hepatic duct, with suspicion of neoplastic involvement. The patient was transferred to Hospital Militar Central in Bogotá, Colombia, to continue with comprehensive management. The obstructive biliary syndrome was documented with a total bilirubin count of 3.02 mg/dL, direct bilirubin of 2.71 mg/dL, alkaline phosphatase of 1006 IU/L, alanine aminotransferase (ALT) of 149 U/L and aspartate aminotransferase (AST) of 139 U/L. The magnetic resonance (MR) cholangiography findings are presented in Figure 1, and those from the computed axial tomography (CT) in Figure 2. The result of the appendicular biopsy showed compromise due to moderately differentiated adenocarcinoma of serous and muscle layer (Figure 3), positive immunohistochemistry for CK7, EMA, monoclonal CEA, and CDX2 antibodies (Figure 4). This suggested an extra-appendicular origin, probably from the upper or hepatobiliary gastrointestinal tract.
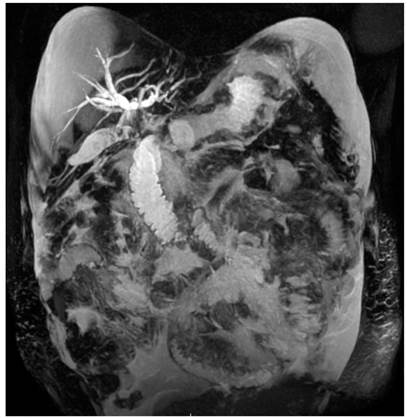
Figure 1 3D MR cholangiography. Intrahepatic bile duct dilation. Abrupt transition and thready liquid flow into the common hepatic duct are observed in the right and left hepatic ducts. Distended gallbladder with multiple hypointense images and interior perigallbladder fluid.

Figure 2 Cecal appendix with contrast material in its lumen, periappendiceal fat stranding, and, in contact with its vertex, heterogeneous mass of poorly defined contours with hypodense and dense areas of 35 x 32 x 44 mm.
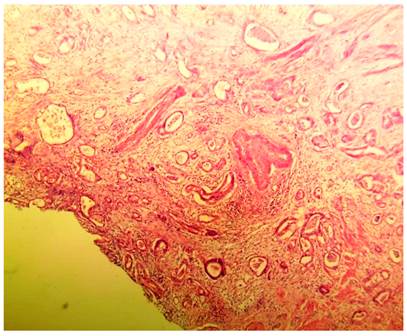
Figure 3 Microscopic findings of the surgical specimen. Hematoxylin and eosin staining show multiple tumoral cells infiltrating the appendiceal serous layer to the submucosa.
The patient was taken back to endoscopic retrograde cholangiopancreatography, evidencing type IV Klatskin tumor. A 10 x 10 French (Fr) stent was inserted in the right hepatic duct and another 12 x 10 Fr stent in the left hepatic duct. Antibiotic coverage with piperacillin/tazobactam was also initially indicated for 72 hours. However, cholangitis was diagnosed given the persistence of obstructive biliary syndrome and fever onset. Therapeutic stepping to meropenem and biliary bypass by interventional radiology were required.
The oncology service proposed to initiate palliative chemotherapy once bilirubin reached under 3 mg/dL. After the first cycle of chemotherapy, the patient was discharged to continue with outpatient management.
Discussion
This report presents the case of a patient with an unusual appendiceal tumor because it began as abdominal pain, typically characterized as inflammatory appendicitis. However, intraoperative and later anatomopathological findings showed an appendix metastatic cholangiocarcinoma, an unusual presentation in the literature.
Most appendiceal tumors are epithelial neoplasms and neuroendocrine tumors5, being less frequent metastatic tumors, lymphomas, neuroectodermal, mesenchymal tumors, and Kaposi’s sarcoma6. In a review of the literature, which retrospectively evaluated the histopathological findings of appendectomies, only 7 patients showed metastatic compromise out of 80,698 patients7. This is a significant figure that puts into perspective the unusualness of this presentation. The bile duct was not reported in this study’s primary sites of metastasis. This situation was atypical for the presentation8.
A case report denoted an appendix metastatic cholangiocarcinoma in a patient with the obstructive biliary syndrome, abdominal pain, and jaundice9. However, the appendiceal finding in this patient was derived from previously performed imaging studies, such as a contrasted computed tomography, which showed cholangiocarcinoma with direct liver extension. Then, a PET scan denoted a mass in the proximal appendix, suggestive of malignancy. This contrasts with the primary intrasurgical finding in the appendectomy in our case.
On the other hand, a case of acute appendicitis with a subsequent finding of appendicular metastatic involvement due to cholangiocarcinoma was also reported in the literature10, a similar clinical presentation to our case. Nevertheless, radiological findings suggest preponderance by metastatic extension, by contiguity rather than by distant seeding of malignant cells11, which could favor a greater presence of secondary involvement by colorectal cancer than by more distant as bile duct-dependent ones.
More information on the clinical presentation of these patients is needed due to the significant limitation of high-quality evidence in this regard. The heterogeneity of the patients’ characteristics on metastatic appendiceal adenocarcinoma reports and, above all, the extreme scarcity of reported cases in the literature do not allow us to infer differences that explain the clinical presentation nor to discern the predictors or prognostic factors of this disease.
We consider that the main strength of this case is the unusual presentation of a metastatic appendiceal tumor of biliary origin, minimally reported in the literature. Likewise, a deep diagnostic exercise and follow-up in a high complexity hospital offer relevant information on the need for and importance of a multidisciplinary approach for patients who present this type of pathology. Given this, it is important to evaluate the presence of similar cases in future studies, which can offer systematized and high-quality information on this clinical presentation.

