











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Cirrhosis, or advanced chronic liver disease, is the final stage of all chronic diseases that affect the liver1, a dynamic inflammatory process characterized by progressive fibrosis of the parenchyma and severe disruption of hepatic lobular and vascular architecture2.
Any chronic aggression against the hepatic parenchyma will eventually result in cirrhosis3. Non-alcoholic fatty liver disease (NAFLD) remains the leading cause worldwide chronic liver disease4,5. As of 2017, the second most frequent liver transplant cause in the United States after hepatitis C virus (HCV) infection6.
NAFLD is defined as a spectrum of alterations in the liver parenchyma. These alterations include the accumulation of triacylglycerol (TAGs)-rich microvesicular and macrovesicular lipid droplets without other secondary causes7. It primarily manifests in people with dyslipidemia, carbohydrate metabolism, and eating disorders. Like obesity, sedentary lifestyle, and high-calorie diet rates have increased, as has non-alcoholic steatohepatitis (NASH)4,5. An estimated 20% will have NASH from the total number of patients diagnosed with NAFLD. In this group, between 3% and 20% will progress to cirrhosis, and between 4% and 27% will have hepatocellular carcinoma (HCC)8,9.
In recent years, several studies have detected a NASH rate increase in Colombia as one of the main etiological factors of advanced chronic liver disease in specialized care centers in different geographical areas of the national territory10-12. These studies have been conducted in overly complex hospital reference centers, where patients in more advanced stages of the disease are usually admitted, possibly leading to an underestimation of the relevance of NASH as an aetiological factor of cirrhosis in our environment. Conducting this study in an outpatient hepatology center could more accurately reflect the relevance of NASH as a cause of advanced chronic liver disease in our country.
The main objective of this study was to describe a group of patients with liver cirrhosis. Additionally, to determine the contribution of NASH as an etiological factor of this population in Cartagena de Indias, Colombia, in an outpatient hepatology care center.
Methodology
A retrospective, cross-sectional, analytical study was conducted. Clinical records of patients were used as the primary source of information. This study took place between January 2013 and August 2020. The population consisted of all the patients visiting Centro Médico Gastropack for liver care monitoring in the city of Cartagena de Indias, Colombia, with a liver cirrhosis diagnosis through:
Clinical criteria: Signs of decompensation and laboratory findings or an upper GI endoscopy (EGD) confirming the presence of esophageal varicose veins.
Radiological criteria: Liver surface nodularity (LSN) increase, liver echogenicity at ultrasound examination increase, right lobe atrophy, hypertrophy of the caudate lobes, liver volume (LV) decrease, portosystemic collaterals, HCC.
Elastography criteria: The Baveno VI > 15 kPa definition was used regardless of etiology13.
Pathological criteria: Liver biopsy with evidence of severe fibrosis or established cirrhosis.
The following paraclinical tests were systematically requested at the time of liver cirrhosis diagnosis to determine the etiology: Hepatitis B surface antigen (HBsAg), anti-HCV, protein electrophoresis, immunoglobulin G (IgG) levels, immunoglobulin M (IgM) levels, ceruloplasmin, ferritin, transferrin saturation index, total antinuclear antibodies, anti-smooth muscle antibodies, anti-mitochondrial antibodies, complete blood count, lipid profile, glycated hemoglobin (HbA1c), creatinine, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, direct bilirubin, albumin, international normalized ratio (INR), alkaline phosphatase, and γ-glutamyltransferase as part of the staging of the degree of liver injury.
All study subjects were under a monitoring protocol that included screening for hepatocellular carcinoma (total abdominal ultrasound and measurement of alpha-fetoprotein every 6 months) (14 and esophageal varicose veins EGD as follows13:
EGD was performed every 2 years in compensated patients without varicose veins in the EGD screening and persistent liver injury.
EGD was performed yearly in compensated patients with small varicose veins and persistent liver injury.
EGD was performed every 3 years in compensated patients -with no varicose veins in the EGD screening, for whom the etiological factor was controlled and had no other related risk factor.
EGD was performed every 2 years in compensated patients -with varicose veins in the EGD screening, for whom the etiological factor was controlled and had no other related risk factor.
EGD was performed every year in decompensated patients.
The CEAP classification15 was used to describe esophageal varicose veins.
The etiological diagnosis of cirrhosis was made following the current international clinical practice guidelines. NAFLD diagnosis was conducted per the American Association for the Study of Liver Diseases (AASLD) of 201816. HCV diagnosis infection was determined according to 2019 AASLD recommendations17. Chronic hepatitis B virus (HBV) diagnosis was determined according to the 2018 AASLD recommendations18. Autoimmune hepatitis (AIH) diagnosis was determined following the 2019 AASLD recommendations19. Alcohol-related liver disease diagnosis was determined using the 2019 AASLD diagnostic criteria20. Primary biliary cholangitis diagnosis was determined using the 2018 AASLD diagnostic criteria21. Primary sclerosing cholangitis diagnosis was determined according to the 2009 AASLD guidelines22. Cryptogenic cirrhosis was discerned in cases where determining attributable etiology was impossible.
Statistical Analysis
Percentages were used for the description of qualitative variables. To determine statistical significance, the difference between means and medians was compared among the quantitative variables, considering p < 0.05.
Ethical Aspects
This study did not entail any risk to the participants as no intervention was performed. All ethical standards for research in human beings given by Colombian Resolution 8430 of October 4, 1993, and the guidelines of the Declaration of Helsinki were met. This document was submitted to and approved by the Gastropack ethics committee.
Results
In this study, 346 clinical records of patients with previous cirrhosis of the liver diagnosis were included. They visited outpatient monitoring by hepatology between January 2013 and August 2020. No diagnosis was made de novo because all patients were referred from other institutions. Neither was it possible to determine the time since diagnosis due to the lack of information in the medical records analyzed. Due to a lack of data, it was impossible to assess alcohol consumption in alcohol-related cirrhosis patients.
Most patients were women (54.3%). The diagnosis was mostly made using the clinical-radiological method (73.4%). Only 51 patients (14.7%) had the definitive pathological study (Figure 1). The most common causes of advanced chronic liver disease were cryptogenic in 35% of the population (121 patients) and NASH cirrhosis, 30.9% (107 patients) (Figure 2).
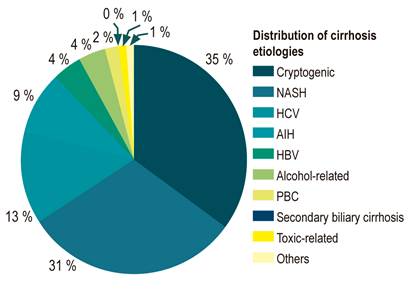
Figure 1 Distribution of cirrhosis etiologies. AIH: Autoimmune hepatitis; PBC: Primary biliary cholangitis; Secondary biliary cirrhosis; NASH: Non-alcoholic steatohepatitis; HBV: Hepatitis B virus; HCV: Hepatitis C virus.
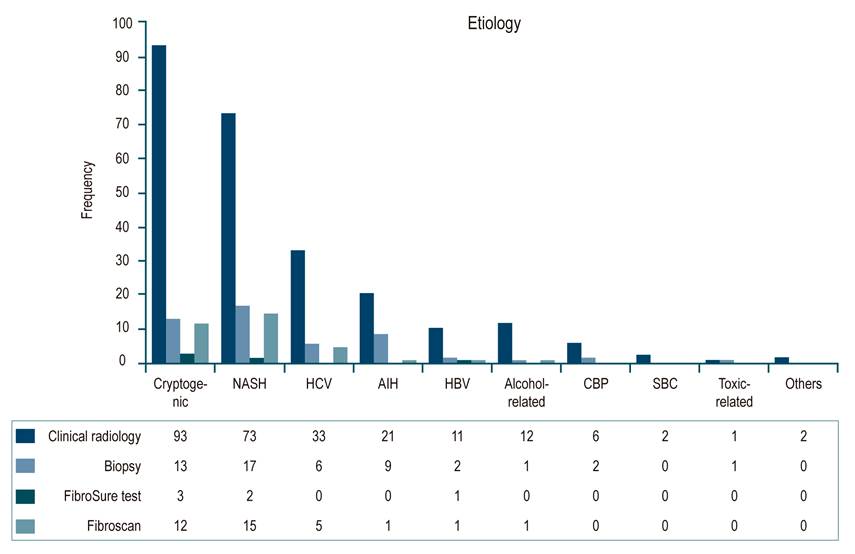
Figure 2 Diagnostic methods used discriminated by etiology. AIH: Autoimmune hepatitis; PBC: Primary biliary cholangitis; SBC: Secondary biliary cirrhosis; NASH: Non-alcoholic steatohepatitis; HBV: Hepatitis B virus; HCV: Hepatitis C virus.
No statistically significant differences were found in our study in terms of decompensation rates (p = 0.081). The highest decompensation percentages were found in patients with secondary biliary cirrhosis (100%) and toxic-related cirrhosis (100%). The lowest decompensation rates were found in patients with primary biliary cholangitis (PBC) (50%) and the category of other etiologies (50%) (Table 1).
Table 1 Characteristics of Inpatients Classified by Etiology
| Cause/variables (%) | Cryptogenic n (%) | NASH n (%) | HCV n (%) | AIH n (%) | HBV n (%) | Alcohol-related n (%) | PBC n (%) | Secondary Biliary Cirrhosis n (%) | Toxic-related (%) | Others n (%) | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | |||||||||||
| - Women | 65 (53.7) | 58 (54.2) | 27 (61.4) | 23 (74.2) | 5 (33.3) | 0 | 5 (62.5) | 1 (50) | 2 (100) | 2 (100) | 0.001 |
| Esophageal Varicose Veins | |||||||||||
| - Yes | 73 (64.0) | 63 (64.2) | 34 (80.9) | 20 (74) | 7 (63.6) | 11 (78.6) | 5 (71.4) | 2 (100) | 0 | 0 | 0.062 |
| Size of Varicose Veins (VVs) | |||||||||||
| - Small | 18 (24.6) | 22 (34.9) | 14 (41.1) | 4 (20) | 5 (71.4) | 5 (45.4) | 2 (40) | 0 | 0 | 0 | 0.119 |
| - Medium | 17 (23.2) | 9 (14.2) | 9 (26.4) | 4 (20) | 1 (14.2) | 1 (0.09) | 1 (20) | 0 | 0 | 0 | |
| - Large | 26 (35.6) | 22 (34.9) | 6 (17.6) | 8 (40) | 0 | 3 (27.2) | 0 | 2 (100) | 0 | 0 | |
| - Unclassified | 12 (16.4) | 10 (15.8) | 5 (14.7) | 4 (20) | 1 (14.2) | 2 (18.1) | 2 (40) | 0 | 0 | 0 | |
| Red Dots | |||||||||||
| - Yes | 7 (9.5) | 8 (12.6) | 2 (5.8) | 1 (5) | 0 | 2 (18.1) | 0 | 0 | 0 | 0 | 0.486 |
| - No | 47 (64.3) | 37 (58.7) | 25 (73.5) | 14 (70) | 5 (71) | 6 (54.4) | 3 (60) | 1 (50) | 0 | 0 | |
| - No Reference | 19 (26) | 18 (28.5) | 7 (20.5) | 5 (25) | 2 (28) | 3 (27.2) | 2 (40) | 1 (50) | 0 | 0 | |
| Decompensation* | |||||||||||
| - Yes | 77 (63.6) | 55 (51.9) | 30 (68.2) | 16 (51.6) | 8 (53.3) | 13 (92.9) | 4 (50) | 2 (100) | 2 (100) | 1 (50) | 0.081 |
| Ascites* | |||||||||||
| - Yes | 51 (42.1) | 32 (30.2) | 16 (36.4) | 9 (29) | 6 (40) | 9 (64.3) | 2 (25) | 1 (50) | 0 | 1 (50) | 0.287 |
| Hepatic Encephalopathy* | |||||||||||
| - Yes | 27 (23.3) | 26 (24.5) | 8 (18.2) | 8 (25.8) | 1 (6.7) | 6 (42.9) | 1 (12.5) | 0 | 1 (50) | 0 | 0.451 |
| Hepatocellular Carcinoma (HCC)* | |||||||||||
| - Yes | 6 (5) | 4 (3.8) | 6 (13.6) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.221 |
| Upper GI bleeding* | |||||||||||
| - Yes | 25 (20.7) | 23 (21.7) | 13 (29.5) | 7 (22.5) | 3 (20) | 7 (50) | 2 (25) | 1 (50) | 0 | 1 (50) | 0.409 |
| Child-Pugh Classification* | |||||||||||
| - A | 33 (42.9) | 56 (60.9) | 18 (47.4) | 12 (54.5) | 8 (66.7) | 2 (20) | 4 (50) | 0 | 0 | 2 (100) | 0.05 |
| - B | 32 (41.8) | 30 (32.6) | 15 (39.5) | 7 (31.8) | 1 (8.3) | 4 (40) | 4 (50) | 1 (100) | 2 (100) | 0 | |
| - C | 12 (15.6) | 6 (6.5) | 5 (13.2) | 3 (13.6) | 3 (25) | 4 (40) | 0 | 0 | 0 | 0 | |
*Note that data could not be obtained for all patients.
Due to a lack of data during admission, the Child-Turcotte-Pugh prognostic scale was calculated in 76% (264 patients) of the study population. Of them, 51.1% (135 patients) were in stage A, 36.3% (96 patients) in stage B, and only 12.5% (33 patients) in stage C (Table 1). Of the total number of patients, 60.1% (208 patients) had a history of decompensation in the months before the outpatient evaluation. The main decompensation causes were ascites 36.7% (127 patients), upper GI bleeding in 23.6% of cases (82 patients), and hepatic encephalopathy in 22.5% (78 patients). Of the total number of patients evaluated, 62.1% (215 participants) had esophageal varicose veins evidenced in the EGD, of which 50.6% corresponded to large varicose veins (Table 1).
Among the different etiologies, there was a higher incidence of varicose veins in patients with secondary biliary cirrhosis in 100% (2 patients) and chronic HCV infection in 80.9% (34 patients). The lowest number of varicose veins incidence in patients was related to toxic and other different etiologies, 0%. Although, no statistically significant differences were evident (p = 0.062).
Regarding vein size, they were larger in secondary biliary cirrhosis patients with 100% of large varicose veins (2 patients) and 40% of cases (8 patients) in AIH (Table 1). Unfortunately, obtaining the body mass indices (BMI) for patients with non-NASH etiology cirrhosis was impossible due to a lack of information in the medical records.
Patients with NASH Cirrhosis
Of the total population, 107 patients showed a NASH cirrhosis diagnosis. The majority were women (54.2%). The diagnosis was mostly made using the clinical-radiological method (68.4%). Only 17 patients (15.8%) underwent the definitive anatomopathological study (Figure 1). Findings among these patients included 80.37% (86 patients) who had type 2 diabetes mellitus (T2DM), 46.7% (50 patients) were overweight (2 overweight patients; 48 obese patients), 41.12% (44 patients) had dyslipidemia, and 13% (14 patients) had primary hypothyroidism (Table 2).
Table 2 Comorbidities Found in Patients Diagnosed with NASH Cirrhosis
| NASH Cirrhosis | |||
|---|---|---|---|
| Yes n (%) | No n (%) | No information n (%) | |
| DM2 | 86 (80,3) | 21 (19,6) | 0 |
| Overweight | 50 (46,7) | 22 (20,5) | 35 (32,7) |
| BMI = 25-29.9 kg/m2 | 48 | ||
| BMI > 30 kg/m2 | 2 | ||
| Dyslipidemia | 44 (41,1) | 62 (57,9) | 1 (0,9) |
| Primary Hypothyroidism | 14 (13,1) | 21 (19,6) | 72 (67,2) |
Due to a lack of information, only the Child-Turcotte-Pugh prognostic scale in 85.9% (92 patients) was calculated. Of them, 60.9% (56 patients) were in class A, 32.6% (30 patients) in class B, and only 6.5% (6 patients) in class C (Table 1). Of the total population, 51.4% (55 patients) had a history of decompensation in the months before the outpatient evaluation. The main cause was ascites in 29.9% of cases (32 patients), followed by hepatic encephalopathy in 24.5% (26 patients) and upper GI bleeding in 21.7% (23 patients). Of the total number of patients evaluated with NASH cirrhosis, 58.9% (63 participants) had esophageal varicose veins evidenced in the EGD screening, and 58.9% corresponded to large varicose veins (Table 1).
Discussion
This study showed that NASH cirrhosis is the second most important cause of advanced chronic liver disease in our environment (30.9%), only below cryptogenic cirrhosis (35%) (Figure 1). However, it is worth noting that some of these patients could correspond to late-diagnosed NASH cirrhosis.
This finding, known as a burnt-out phenomenon, is well documented in the medical literature and refers to the paradoxical event that occurs in the most advanced fibrotic stages of the disease, in which the histopathological findings reveal little or no amount of fatty deposit, making definitive aetiological diagnosis difficult22. For this reason, NASH has been recognized as one of the leading causes of cryptogenic cirrhosis and accounts for most cases24-26.
However, this relationship is not always easy to determine because the available studies are primarily retrospective, and not all the information necessary to establish a definitive etiology is available. In addition, in daily practice, many biopsies are performed in the advanced stages of the disease. Moreover, changes in lifestyle aimed at patients with metabolic risk factors could modify the appearance or progression of NASH, making the aetiological link even more difficult at the time of diagnosis. Thus, potentially explaining why the primary origin of cirrhosis in our study was cryptogenic.
The actual incidence of NASH cirrhosis remains unknown since the existing studies used different population groups, diagnostic methods, and other variable parameters with inconsistent epidemiological results27. Nonetheless, more recent data have shown an increase in the prevalence of NASH cirrhosis and advanced fibrosis associated with NAFLD between 2 and 2.5 times compared to results from previous years28.
In the first reports made in Latin America, NASH was not among the most relevant causes of cirrhosis. It is probably related to the lack of awareness of the disease and the poor search for comorbidities29. More recent studies, such as the one conducted by García et al., in 2020, in Argentina, have highlighted the increase in NASH cirrhosis diagnoses in recent years, identifying it as the third most important cause of cirrhosis (13.5%) and showing a significant increase when compared to the 1995-2002 period, in which no diagnosis was made30.
Apart from the fact that population genetic differences could explain these variations, it is also true that the lack of uniformity in the diagnostic methods used and the absence of specific protocols for screening this population have led to a large number of patients with NAFLD being diagnosed in advanced stages of the disease.
Multiple descriptive studies of the population with liver cirrhosis have been conducted in Colombia. In 2013, Giraldo-Montoya et al. conducted a descriptive study in a cohort of patients with a previous diagnosis of advanced chronic liver disease in outpatient hepatology follow-up, which showed that NASH cirrhosis was the fourth most prevalent cause (11%)10.
In 2016, Prieto et al. ranked NASH as the leading cause of cirrhosis (25.5%) in a group of patients in Bogotá who consulted outpatient monitoring for hepatology12. In 2017, Escorcia et al. conducted a retrospective, cross-sectional study in Barranquilla to describe cirrhotic patients under outpatient follow-up. In that study, they found NASH cirrhosis as the second most important cause of the advanced chronic liver disease (24.6%)11.
Regarding previous local studies data, our study shows that there has been an increase in the proportion of these patients. In our population, 30.92% had a diagnosis of NASH cirrhosis, the highest number reported in recent years, which could be higher given that many of the patients with cryptogenic cirrhosis could correspond to late NASH cirrhosis diagnosis, as previously mentioned. This upward trend is related to the increased prevalence of metabolic risk factors nationally.
In Colombia, according to data from the Food and Nutritional Security Observatory (OSAN, for its acronym in Spanish), the prevalence of obesity went from 13.7% in 2005 to 16.5% in 2010 and 18.7% in 2015. In the same period, the prevalence of overweight went from 32.3% to 34.6% and 37.7% in 201531. As a result, obesity has led to an increase in mortality and a higher risk of presenting chronic non-communicable diseases (NCDs) such as DM2, high blood pressure (HBP), dyslipidemia, and cardiovascular disease (CVD)32 all risk factors for the development and NAFLD progression33,34.
In our report, 46.7% of patients with NASH cirrhosis were overweight (2 overweight patients, 48 obese patients). Although this association could be even higher due to the retrospective nature of our study, about 33% did not have a BMI record, which could underestimate the prevalence in this cohort. In addition, some findings showed that 80.37% of these patients had DM2, correlating the results of Giraldo-Montoya et al., who reported that 85.7% of their patients with NASH cirrhosis had diabetes10. Lower rates of dyslipidemia were found in our registries.
Regarding the prognosis of the disease, 51.1% of the global cohort was in Child-Pugh class A, unlike the study by Giraldo-Montoya et al10, in which the majority corresponded to class B and C of the Child-Pugh, indicating that our population was diagnosed in earlier stages of the disease. Therefore, the findings offer a closer view of the general population’s expected behavior.
Concerning the decompensation frequency, higher rates were found (both in the overall cohort and in the NASH cirrhosis cohort) when compared with the studies by García et al30 and Escorcia et al11 that were also performed in outpatient hepatology centers. Although they were lower when contrasted with the study Giraldo-Montoya et al10 conducted on hospitalized patients, as expected.
Some studies have shown an apparent discrepancy in the risk of decompensation at 5 years between the different causes of advanced chronic liver disease. Alcoholic cirrhosis showed the highest rate of decompensation35. NASH cirrhosis ranks only below this, with a risk of decompensation at 5 years of 23.6 ± 7.8%35. Statistically, our study did not show significant differences (p = 0.05).
This study reveals an increase in the diagnosis of NASH cirrhosis in our country. This phenomenon may be related to the increased prevalence of reported overweight and obesity and the current awareness of the disease.
Due to the retrospective nature of our study, it was impossible to describe all the patients according to their BMI, which was a crucial datum, as stated in the discussion. However, this study’s strength is that our trial was not conducted in a high-complexity hospital. Instead, this clinical trial took place in an outpatient hepatology care center, which offers a closer view of the general population.
Conclusions
Our results point to NASH cirrhosis as an emerging cause of advanced chronic liver disease in our environment.
In the future, the design of strategies aimed at reducing the burden of liver disease in Colombia should prioritize specific and comprehensive actions for patients with NAFLD, ensuring the rational and practical use of available resources.

