











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
The venous thromboembolic disease has positioned itself as a condition of interest in public health, given its high morbidity and mortality, particularly the one related to unusual sites that pose a diagnostic and therapeutic challenge1. Thus, it should be specified that splanchnic thrombosis refers to that located in the portal, mesenteric, or splenic vein or the hepatic venous flow; they are generally uncommon and occur in the context of hereditary thrombophilias (21%), infectious or inflammatory disorders, neoplasms, or liver cirrhosis. It has nonspecific manifestations, abdominal pain being the most common symptom (50%), followed by gastrointestinal bleeding and ascites2,3.
Thrombophilias have been frequently related to venous thromboembolic disease. These can be classified as primary when they are hereditary, as in the case of sticky platelet syndrome, and secondary if they are associated with an acquired risk factor such as the Janus kinase 2 (JAK2) mutation4, documented in up to 32.7% of patients with splanchnic venous thrombosis(3).
Classically, this mutation has been associated with Philadelphia chromosome-negative myeloproliferative neoplasms (MPN) such as polycythemia vera (96%), essential thrombocytosis (55%), and primary myelofibrosis (65%)5. The latent condition of this type of neoplasia refers to the sole identification of the JAK2 mutation without peripheral alterations such as cytopenias and with normal erythropoietin levels. Recognizing it is becoming increasingly important given the clinical spectrum that will give rise to the natural evolution of the disease6.
Besides MPNs, it is crucial in thrombosis of unusual sites to consider other etiologies such as sticky platelet syndrome, an autosomal dominant disease characterized by abnormal platelet aggregation. For its diagnosis, a platelet aggregometry with epinephrine and adenosine diphosphate (ADP) must be performed; the platelets are exposed to low concentrations of these substances, assessing the response against standard parameters for the test7. It has been associated with arterial (21%) and venous (13%) thrombotic events, generally recurrent; its manifestation can be related to any state of hypercoagulability, the most frequent being factor V Leiden mutation8.
A case of splanchnic thrombosis is presented below as the initial manifestation of latent MPN associated with sticky platelet syndrome.
Clinical case
A 38-year-old woman was admitted to the emergency department due to a clinical picture of sudden onset. It was characterized by acute pain with visceral nociceptive features, initially located in the epigastrium with subsequent generalization and radiating to the bilateral lumbar region, with an intensity of 9/10 on the visual analog scale (VAS) for pain. She had no extenuating or exacerbating factors. The clinical picture was associated with sweating, nausea, and vomiting of food content. The patient referred to it as the first episode of this type of symptomatology. She had no relevant pathological, family, gynecological, or pharmacological history, and the symptom systems review was negative. On physical examination, her blood pressure (BP) was 100/50 mm Hg and heart rate (HR) 99 beats per minute (bpm). She exhibited abdominal distension and diffuse pain on palpation, predominantly in the upper abdomen, with no signs of peritoneal irritation.
Due to the sudden-onset pain characteristics, it was deemed sensible to rule out a vascular origin, for which a contrast-enhanced abdominal tomography was performed, showing thrombosis of the portal vein without cavernous transformation. An endoscopy of the upper digestive tract was performed, finding large esophageal varices of 7 mm in diameter, tortuous from 27 cm to the Z line, with maximum insufflation occupying more than a third of the lumen of the esophagus. On the surface of the varices, cherry-red spots classified as F3 and cardinal varices were observed, and the esophageal varices were ligated. However, the abdominal pain persisted, and laparoscopy was considered. Serohemorrhagic fluid and ischemic jejunal loop were found in a segment of 20 cm to 5 cm of the ligament of Treitz, with no necrosis, mesenteric venous engorgement, and preserved pulses.
The content was aspirated, and no additional surgical procedure was considered. Subsequently, we decided to perform an abdominal angiography, revealing thrombosis of the splenic and mesenteric veins and intrahepatic portal vein with collateral circulation and physiological splenorenal shunt associated with splenomegaly and permeabilization of the left gastric vein (Figure 1). Anticoagulation was indicated with low molecular weight heparin (LMWH) and a non-selective β-blocker.
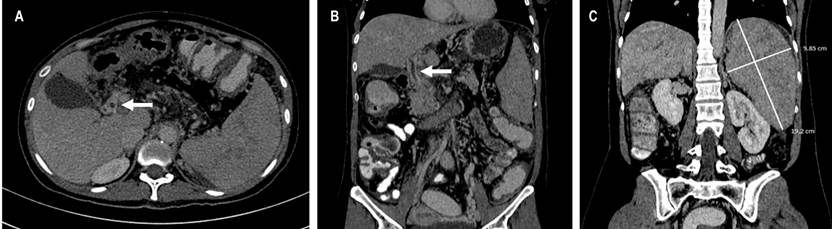
Figure 1 A. There is no adequate opacification of the portal vein (white arrow). B. Portal vein, multiple serpentine vascular images going to the hepatic hilum are observed in its course, suggesting portal hypertension (white arrow). C. Splenomegaly (white line).
Since the leading causes of thrombosis in these sites are thrombophilias, relevant tests were performed (Table 1). Only one JAK2V617F mutation was identified, and the blood count showed findings related to mild anemia. Thus, erythropoietin (EPO) level tests were requested, which were within normal parameters, leading us to consider a latent MPN.
Table 1 Paraclinical tests performed during the patient’s hospitalization
| Tests | Patient value | Reference value |
|---|---|---|
| Factor V Leiden mutation | Negative | Negative |
| Prothrombin gene mutation | Negative | Negative |
| Antithrombin III | 87.2% | 75%-125% |
| Protein C | 77.2% | 65%-140% |
| Protein S | 65.2% | 52%-118% |
| Homocysteine | 9.11 | 5-12 µmol/L |
| Flow cytometry for PNH | Negative | Negative |
| JAK2V617F mutation | Positive | Negative |
| Factor VIII | 74.9 | 50%-150% |
| Factor IX | 54.5 | 50%-150% |
| Factor XI | 58.2 | 50%-150% |
| Erythropoietin | 14.3 | 4.3-29 |
| D-dimer | 100 | 0-500 µg/mL |
| LDH | 169 | 140-280 U/L |
| Lupus anticoagulant | Negative | Negative |
| Anticardiolipin |
|
|
| Anti-β2-glycoprotein 1 antibodies |
|
|
| Antinuclear antibodies | Negative | < 1:80 |
| Complete blood count | Leukocytes:
|
|
Hb: Hemoglobin; PNH: Paroxysmal nocturnal hemoglobinuria; IgG: Immunoglobulin G; IgM: Immunoglobulin M; MCV: Mean corpuscular volume.
In addition, platelet aggregometry was performed, revealing hyperaggregation at two concentrations with both ADP and epinephrine (Figure 2) classified as type 1 sticky platelet syndrome (SPS). Once she showed clinical improvement, anticoagulation was indicated in an off-label or unapproved manner with rivaroxaban 20 mg/day.
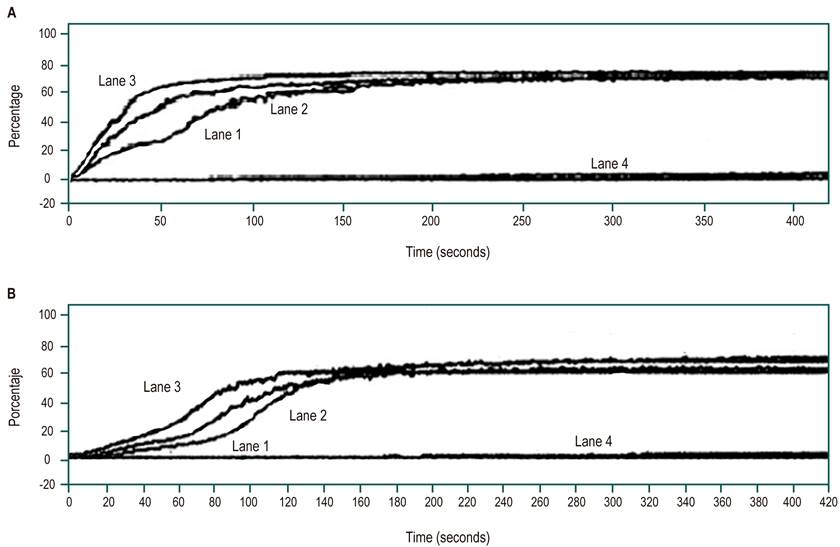
Figure 2 A. Platelet aggregation study with ADP compatible with sticky platelet. Lanes: 1: No platelet hyperaggregation with ADP at a concentration of 2.3 µM; 2: Platelet hyperaggregation with ADP at a concentration of 1.2 µM; 3: Platelet hyperaggregation with ADP at a concentration of 0.6 µM; 4: Negative control with 0.85% saline solution (SS). B. Platelet aggregation study with epinephrine compatible with sticky platelet. Lanes: 1: No platelet hyperaggregation with epinephrine at a concentration of 11 µM. 2: Platelet hyperaggregation with epinephrine at a concentration of 1.1 µM; 3: Platelet hyperaggregation with epinephrine at a concentration of 0.6 µM; 4: Negative control with 0.85% SS.
Discussion
We present the case of a young adult female patient who had sudden abdominal pain as an initial manifestation, one of the symptoms that creates the most confusion in an emergency department due to the multiple differential diagnoses of this condition. The sudden appearance is alarming due to the possible related etiologies, among which visceral perforations or vascular alterations (rupture or ischemia)9 stand out. Given the preservation of vital signs and absence of peritoneal irritation, contrast-enhanced abdominal tomography was performed first, showing thrombosis in the portal vein and, subsequently, splanchnic venous thrombosis was confirmed using angiotomography (unusual site of thrombosis). Other causes, such as gynecological ones, can be ruled out. It is crucial to remember that this is the most frequent symptom in this type of pathology3.
In patients under 40 years of age with splanchnic thrombosis, searching for primary thrombophilias such as factor V Leiden mutation, prothrombin, antithrombin III, protein S and C deficiencies, homocysteine, sticky platelet syndrome, and secondary thrombophilias such as syndrome chronic antiphospholipid and MPN is essential to define long-term therapeutic strategies10. Other alterations such as PNH must be ruled out, which takes on significant relevance. Its identification is an independent factor for mortality11, ruled out by peripheral blood flow cytometry.
The patient in the clinical case had two conditions that increased the risk of venous thrombotic events, such as the JAK2 mutation in the context of latent MPN and sticky platelet syndrome4-8. Notably, its prevalence is quite rare, so this would be one of the first cases reported with this association.
Regarding the treatment of splanchnic thrombosis, it is based on early anticoagulation to improve vessel recanalization and avoid complications; however, the risk of bleeding is high, especially in patients with esophageal varices5. In recent years, the efficacy of rivaroxaban vs. warfarin in resolving thrombosis (86% vs. 45% for warfarin) and improving late recanalization with no recurrence of thrombotic events and no bleeding episodes has been proved12. A prospective cohort from the Mayo Clinic, where the safety of direct-acting oral anticoagulants (DOAC) was evaluated, included 63 patients with unusual thrombosis, primarily women (63%). Non-inferiority was noted in the risk of recurrence of thrombotic events and bleeding with DOACs (rivaroxaban and apixaban) compared to LMWH13. The first-line treatment for sticky platelet syndrome is aspirin14. In the present case, given the evidence of factors that increased the risk of recurrent thrombosis, we decided to start indefinite anticoagulation as an off-label or unapproved measure with a direct factor Xa inhibitor (rivaroxaban 20 mg/day). Nonetheless, due to the high risk of bleeding in this patient caused by esophageal varices and a lack of clinical trials evaluating dual therapy together with aspirin, its use was not considered in this context. With this therapeutic approach, the patient has had an outpatient follow-up for 15 months and has not presented with new symptomatic thrombotic episodes.
Conclusion
When evaluating acute abdominal pain of sudden onset, the correct application of semiology is critical to identify the patient who requires medical or surgical management. Besides, it is necessary to rule out vascular origin as a causal factor. The proper use of diagnostic aids such as abdominal tomography helps exclude or confirm potential etiologies, considering the age group and clinical manifestation. Venous thrombosis of unusual sites, such as splanchnic thrombosis, is a low-prevalence entity, which poses not only diagnostic but also a therapeutic challenge for the clinician due to its manifestation and associated pathologies such as primary (platelet syndrome sticky) and secondary (latent MPN) thrombophilia. All of the above is relevant when establishing an effective treatment, in this case, anticoagulation, improving the patient’s prognosis and quality of life.

