











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Superior mesenteric artery (SMA) syndrome has been referred to by different names, Wilkie’s syndrome, aorto-mesenteric compass syndrome, cast syndrome, chronic duodenal ileus syndrome, and arteriomesenteric duodenal occlusion syndrome. When the angle is < 25°, it is defined as the compression of the third portion of the duodenum between the abdominal aorta and the superior mesenteric artery (SMA)1-9. This syndrome is a rare cause of intestinal obstruction, with an estimated 0.1% to 0.3% incidence1,2. The abdominal aorta and SMA normally form an angle between 38° and 65°. Since the duodenum and left renal vein are located within the mesenteric angle, both types of compression may occur. Predisposing factors are associated with the decrease in the mesenteric fat pad between the aorta and the superior mesenteric artery, which reduces the angle and distance between the two. These conditions -congenital or acquired, are associated with significant weight loss, including situations of hypermetabolism (trauma and burns), dietary conditions (anorexia nervosa and malabsorptive diseases), and conditions causing cachexia (AIDS, cancer, paraplegia)1-13.
Because the clinical picture is variable, there is often a delay in diagnosis. The most typical clinical manifestations include reports of postprandial epigastric pain, nausea, vomiting, and early satiety with weight loss1-11. When SMA and Nutcracker syndrome coexists, hematuria, mainly microscopic, and proteinuria may appear when left renal vein stenosis is significant, which causes venous hypertension10-14. There are no currently validated clinical diagnostic criteria; thus, imaging studies may confirm a suspicion5-10. Conservative treatment has been proposed as the first line of action, in which nutritional support seeks to recover the mesenteric pad. Frequently, failure in therapy determines the need for surgical intervention, with high success rate reports in the literature1-13.
Case presentation
A 25-year-old man from the United States. He repeatedly consulted for a clinical picture of a 1-year evolution of postprandial abdominal pain and distension, nausea, vomiting, and distension, contributing to a 30 kg weight loss. In several admissions to the hospital due to intestinal obstruction -which responded to medical treatment, laboratory tests were performed to rule out infectious, autoimmune, hematological, and neoplastic diseases. Additionally, upper and lower endoscopy, video capsule endoscopy, abdominal scan, abdominal magnetic resonance imaging (MRI), and diagnostic laparoscopy studies were performed without obtaining significant findings on a possible etiology. He received nutritional support and pharmacological treatment as part of his medical treatment. However, his symptoms did not improve.
In March 2020, he consulted our outpatient gastroenterology unit in Cali, Valle del Cauca. During anamnesis, the patient mentioned a history of infectious gastroenteritis 1 year before on a trip to San Andres, with subsequent weight loss. At admission, secondary cachexia to weight loss could be evidenced without alteration in the hemodynamic state. New endoscopic studies were performed that showed no evident alterations. While in the endoscopy recovery room, he required a transfer to the emergency department because he developed acute abdominal pain and oxygen desaturation. Within the examinations performed, the CT enterography showed dilation of the colon and small bowel loops. The sagittal reconstruction showed a decrease in the aortomesenteric angle and compression of the third portion of the duodenum and compression of the left renal vein (Figure 1). The upper digestive tract radiography showed a filiform passage of the contrast medium in the third portion of the duodenum toward the distal (Figure 2).
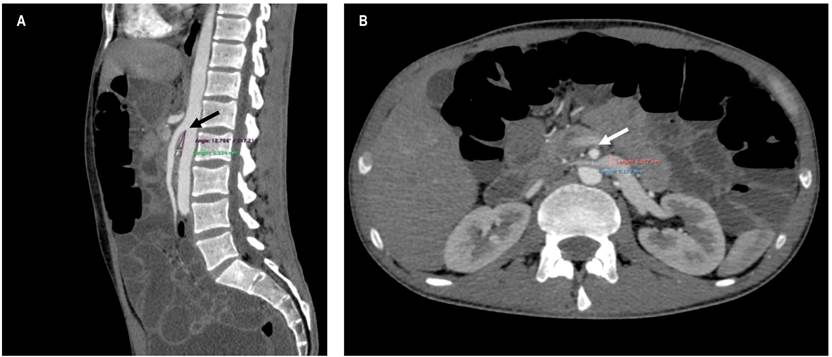
Figure 1 Abdominal CT scan. A. The reconstruction in the sagittal plane shows the narrowing of the aorto-mesenteric angle, 12,786°, with a reduced aorto-mesenteric length of 5334 mm (black arrow). B. The reconstruction in the axial plane shows the compression of the left renal vein with a ratio of the anteroposterior diameter of the compressed vein over the enlarged compressed vein (6927 mm/2179 mm = 1179) (white arrow).
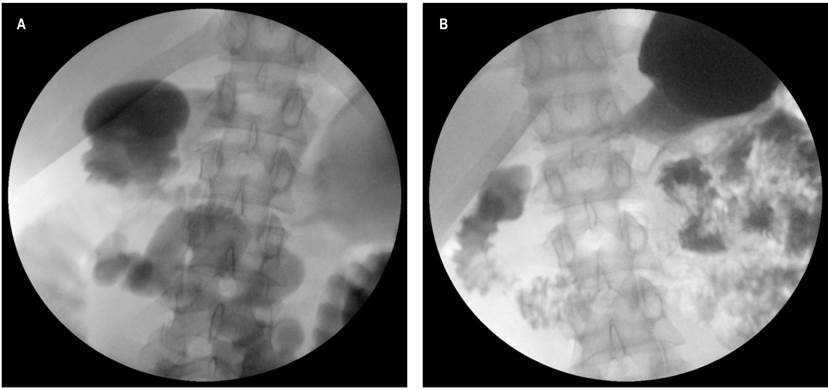
Figure 2 Gastroduodenal series. Radiographic imaging show proximal dilatation of the duodenum (A), with a significant compression in the midline of the third portion of the duodenum (B).
After confirming the diagnostic impression, enteral nutritional supplementation was started with poor response, persisting with nausea, vomiting, abdominal pain, bloating and early fullness, and oral tolerance. The patient underwent surgery because he did not show any improvement signs. Thus, a transmesocolic duodenojejunostomy was performed 40 cm from the ligament of Treitz. There, large retroperitoneal lymph nodes found in the procedure were sampled, which in a subsequent pathological study showed reactive lymphadenopathy and follicular and sinus hyperplasia.
The patient’s postoperative recovery was initially torpid, showing edema of the duodenojejunal anastomosis, which was treated with an endoscopic advancement of an enteral tube -distal to the anastomosis. Thus, the patient experienced a gradual symptom remission and gained 3 kg and progressive oral tolerance in the first month, resulting in the removal of the nasojejunal tube. As a result, the patient could return to the United States, and 9 months later, he has not reported any gastrointestinal symptoms. He is in good health condition and reported a 12 kg weight gain.
Discussion
Boerneus first described the SMA in 1752 through findings in a necropsy11. Around 1842, SMA was considered a cause of duodenal obstruction by Carl Freiherr von Rokitansky due to aorto-mesenteric compression1. Regarding its etiology, Soutclern associated lordosis with duodenal stasis; Kundrat asserted that incomplete duodenum obstruction was due to the compression of the mesentery root. In 1900, in post-mortem studies, Robinson found that the mesenteric vessels caused the compression of the duodenum, with dilation of its proximal portion1,11. It remained an unknown disease until 1927 when Wilkie reported 75 cases and would henceforth bear his name1.
So far, SMA is known as a rare disease, and the bibliography corresponds to case reports. Different manifestations have been reported; however, patients typically report chronic gastrointestinal symptoms, abdominal pain, nausea, belching, excessive vomiting of bilious content or partial digestion, postprandial discomfort, and early satiety1-13, as our patient showed in time. It also required treatment for multiple episodes of subacute intestinal obstruction and weight loss, characteristic of the disease as reported in the literature2,6,8. Studies have reported that SMA syndrome can be associated with compression of the left renal vein. When such cases show symptoms, hematuria is the most common one -not found in our patient10-14.
In the first half of the twentieth century, there were no clear diagnostic criteria, and indications for treatment were limited, so the final results were not as desired. In the 1960s, aortic angiography combined with a contrasted gastroduodenal series began to take place in an attempt to determine the obstruction site10. It was until the 2000s that case studies began to define imaging in patients with a suggestive clinical picture1-10. Abdominal CT is currently considered the gold standard for diagnosing SMA. It has a sensitivity and specificity rate close to 100%.4-8
The MSA is known to form an angle of approximately 45° with the abdominal aorta and the third portion of the duodenum2,9. Recent reports agree that factors that abruptly reduce the aorto-mesenteric angle to less than 25° can generate clamping of the third portion of the duodenum. This is the first diagnostic imaging criterion1,2,6-8. Other findings include an upper aortomesenteric distance less than or equal to 8 mm, the duodenum fixed by the ligament of Treitz, or an anatomical variant of the MSA syndrome6. The CT enterography of our reported case showed a 12.8° angle with a 5.33 mm distance -meeting these criteria (Figure 1).
Conservative treatment is the initial management option. Mobilization and positioning in the left lateral decubitus or the prone decubitus after meals to control postprandial symptoms, correcting hydro electrolytic alterations, and parenteral nutritional supplement focused on recovering the aortomesenteric fat pad1. Previous reports have shown that the likelihood of improvement with non-surgical therapy significantly decreases after the second unresponsive week1-13. Over the past year, the patient has received medical treatment for his symptoms and episodes of subacute bowel obstruction without full and lasting relief.
In 1908, Stavely performed the first successful surgery for Wilkie’s syndrome at Johns Hopkins Hospital11. Since then, several procedures have been used, including Treitz ligament division (Strong’s operation), gastrojejunostomy; subtotal gastrectomy and Billroth II gastrojejunostomy; duodenojejunostomy and anterior repositioning of the duodenum1. Nowadays, the preferred method is duodenojejunostomy, which in our case, resulted in a complete resolution of the symptoms and progressive weight gain1-13. Over the last 10 years, progress in the surgical technique has been made, and there are successful reports of short-duration laparoscopic duodenojejunostomy without complications12,13.
Regarding the left renal vein compression, left renal vein transposition may be considered in cases of kidney failure, orthostatic proteinuria, persistent varicocele or hematuria, or non-response to conservative therapy. In asymptomatic cases -like our patients, conservative therapy is the first line of treatment.
Conclusion
Wilkie’s syndrome is a low-frequency disease that should be considered a differential diagnosis in patients with weight loss and subacute bowel obstruction presenting abdominal pain, nausea, belching, and bulky vomiting. Medical imaging confirms clinical suspicion, and abdominal tomography is the gold standard. Initially, conservative therapy may be considered, but most cases will require surgical therapy with laparoscopic duodenojejunostomy, which achieves recovery rates even greater than 80%.

