











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
In the last decades, neuroendocrine tumors (NETs) have been diagnosed more frequently through the implementation of colonoscopy and complementary imaging studies in gastrointestinal diseases. They have distinctive histological, biological, and clinical characteristics1. These tumors originate in neuroendocrine cells from the endoderm along the mucosa and submucosa of the gastrointestinal tract1. They can synthesize and secrete monoamines, peptides, and hormones and transmit and receive nerve signals2. Lubarsch discovered these tumors in 1888. Later, Obendorfer named these tumors carcinoid (carcinoma-like). Nowadays, they are known as neuroendocrine tumors (NETs) according to their etiology, behavior, and location3,4.
NETs constitute 0.5% of all malignant cancers and 2% of malignant tumors in the gastrointestinal tract2. They have an incidence of approximately 0.86 per 100,000 inhabitants, frequent in Black males and more prevalent in the Asian population4-7. Rectal NETs account for 18% of total NETs and 27% of gastrointestinal NETs5.
Clinical presentation is nonspecific. Rectal bleeding, functional gastrointestinal disorders, abdominal pain, and carcinoid syndrome may be present in 10% of cases6,7. However, nearly half of the patients are asymptomatic and are diagnosed in screening colonoscopy or other colorectal pathology studies7-9. They are usually found as single small polypoid tumors, metastatic disease is rare, and tumor size and invasion determine the prognosis of the disease10-13.
In the latest digestive tumor classification edition (fifth edition, published in 2019) of the World Health Organization (WHO), the classification of well-differentiated NETs or poorly differentiated neuroendocrine tumors with small cell and large cell subtypes remains14. Histological classification is based on the mitotic and Ki-67 indexes recorded at tumor hot spots. During cell division, the Ki-67 protein is found in the cell nucleus. The proportion of Ki-67-positive tumor cells (Ki-67 index) correlates with cell proliferation, clinical course, and prognosis2,14-16. The 2019 WHO NET classification is described in Table 1.
Table 1 Classification of Neuroendocrine Tumors, WHO, 201916
| Ki-67 Index (%) | Mitotic index/10 HPF | |
|---|---|---|
| Well-differentiated neuroendocrine neoplasms | ||
| Grade 1 (Low) | < 3 | < 2 |
| Grade 2 (Intermediate) | 3-20 | 2-20 |
| Grade 3 (High) | > 20 | > 20 |
| Poorly differentiated neuroendocrine neoplasms | ||
| N/A (no numerical assignment: high grade) | > 20 | > 20 |
HPF: high-power fields; N/A: not applicable. Taken and adapted from: Lloyd RV, Osamura RY, Kloppel G, Rosai J. WHO Classification of Tumors of Endocrine Organs. 5th edition. WHO; 2019.
In general, well-differentiated tumors are low or intermediate-grade tumors. Well-differentiated high-grade NETs are less frequent but have a better prognosis than poorly differentiated NETs, a fundamental classification to know the course of the disease and define the most appropriate treatment for the patient1,12-14. Below is a case of a neuroendocrine tumor as a polyp in the rectum.
Case presentation
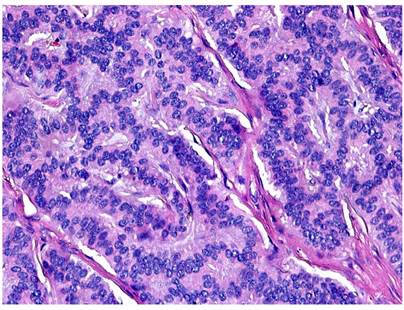
This is an 88-year-old female patient with a medical history of hypertension, hyperlipidemia, type II diabetes mellitus, breast cancer in remission, and grade I internal hemorrhoids. She sought medical assistance for a long-standing clinical picture characterized by constipation with no other gastrointestinal symptoms. The patient underwent a colonoscopy where a polyp was evidenced in the upper third of the rectum, 12 cm from the anal edge of 2 cm in diameter (Figure 1). A polypectomy was performed, and a sample was sent for pathologic study, which reported morphologic findings compatible with a well-differentiated neuroendocrine tumor. Tumor size was 1 cm in greatest dimension, submucosal location, and lateral and deep negative resection margins for tumor involvement (Figures 2 and 3). Immunohistochemistry staining showed a well-differentiated neuroendocrine tumor with a low mitotic rate with Ki-67 < 1%. Outpatient follow-up with colonoscopy check-up in 1 year was indicated.
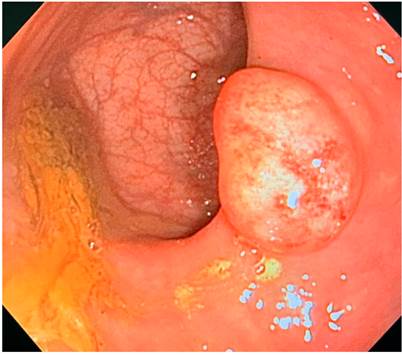
Figure 1 Colonoscopy image showing a neuroendocrine polyp in the upper third of the rectum, 2 cm in diameter.
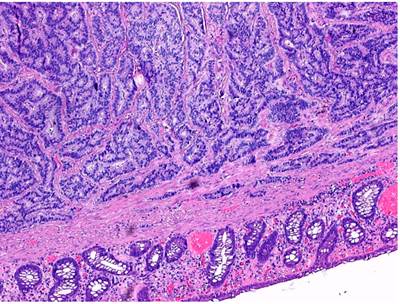
Figure 2 The colonic cut shows a submucosal lesion with an organoid pattern (4x). Hematoxylin and eosin (H&E) stain.
Discussion
In recent years, the diagnosis of rectal NETs has increased thanks to colonoscopy as a screening method for colon cancer and the implementation of other imaging studies of the gastrointestinal tract5. In a British cohort of 13,061,716 patients who were screened with fecal occult blood, 259,765 of the participants obtained abnormal results, and 216,707 screening colonoscopies were performed; 146 patients were diagnosed with NETs, and it was evidenced that the diagnostic rates per 100,000 colonoscopies were 29 rectal, 18 colonic and 11 ileal NETs17.
There is a tendency to delay the diagnosis of all types of NETs, which can take up to 5 years, related to their asymptomatic clinical presentation17,18. The vast majority (93%-100%) of rectal NETs are < 1 cm in size at diagnosis, limited to the submucosa, well-differentiated, and generally have a benign clinical course14,19.
The risk of metastatic disease of NETs increases with tumor size, which is up to 60%-80% when the tumor is ≥ 2 cm20. Tumor size > 10 mm and muscle and lymphovascular invasion are independently associated with an increased risk of metastasis20,21. However, there is a higher detection of the disease in the early stages related to a lower risk of metastasis. A retrospective study that evaluated 48 patients showed that stage I tumors (TNM) accounted for 78.8% and were the most frequent. At the same time, distant metastases had a lower incidence22, which is related to the findings of a recent systematic review in which it was evidenced that only 5% measured more than 20 mm at the time of diagnosis(20.21). Endoscopic ultrasound and magnetic resonance imaging (MRI) are used to evaluate the tumor’s exact size, extension into the rectal wall, and the condition of the perirectal lymph nodes, facilitating better treatment selection and improving the complete resection rate10.
Various endoscopic procedures can be used in rectal NET resection, including conventional polypectomy, endoscopic mucosal resection, and endoscopic submucosal dissection10,19. According to the European Neuroendocrine Tumor Society consensus, well-differentiated rectal NETs below 1.5 cm without invasion of muscularis propria or lymph node involvement can initially be treated endoscopically10,20. Transanal excision should be considered when the margins of endoscopic resection are positive19. The distance between the tumor and the anal canal and the potential of the tumor to cause an obstruction should be considered when choosing the most appropriate treatment19-21. When there are positive locoregional lymph nodes or invasions of the muscularis propria, more radical methods such as excision with low anterior resection or abdominoperineal resection should be chosen20,21.
According to the European Neuroendocrine Tumor Society (ENETS), patients should be monitored after the complete resection of rectal NETs, as described in Table 2.
Table 2 Follow-up and surveillance indications per tumor size and grade according to ENETS6,10,14,21
| Size | Grade | Follow-up |
|---|---|---|
| < 1 cm | 1-2 | No surveillance needed |
| < 1 cm | 3 | Annual colonoscopy for 5 years |
| 1-2 cm | N/A | Colonoscopy, ultrasound, and MRI at 12 months, then colonoscopy every 5 years |
| > 2 cm | 1-2 | Colonoscopy and annual MRI for 5 years |
| > 2 cm | 3 | Colonoscopy and MRI every 4 to 6 months for the first year, then annually for 5 years |
N/A: not applicable; MRI: magnetic resonance imaging; ENETS: European Neuroendocrine Tumor Society.
Rectal NETs have the best overall survival of all gastroenteropancreatic NETs, largely due to the high incidence of small rectal NETs with no evidence of invasion and an excellent long-term prognosis21,23.
Localized rectal NETS (T1, N0, M0) have a 5-year survival of 98%-100%, while those with regional (N1) and distant (M1) metastases have a 54%-74% and 15%-37% survival, respectively5,23,24.
We stress the importance of performing regular endoscopic screening in selected patients, detecting and diagnosing the presence of NETs early to avoid complications related to advanced stages of the disease and, thus, reducing morbimortality rates. When evaluating polyps of the gastrointestinal tract, the diagnosis of NETs should be considered a possibility, and its characteristics should be considered to define prognoses and follow-up.
Conclusion
Thanks to the incursion of colonoscopy as a screening method for colorectal cancer, the diagnosis of rectal NETs has increased. The risk factors that may lead to their appearance are still unknown due to the lack of large epidemiological studies. In general, at the time of diagnosis, tumors are mostly less than 1 cm, well-differentiated, and can be found in polypoid form, as in our case, which gives patients a better long-term prognosis. Given their smaller size, they can be treated endoscopically without any risk. However, histological classification, size, and location must be considered to define the need for more radical treatments. Rectal NETs have better overall survival than all NETs. It is important to continue population screening through endoscopic studies for early detection and treatment of these tumors.

