











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Intestinal failure is the reduction of intestinal function that requires intravenous supplementation of macronutrients, water, or electrolytes, to the extent that the intestine does not achieve the minimum absorption to maintain health or growth1. Acute intestinal failure can have a frequency of 15% in patients with critical illnesses or during the perioperative period of abdominal surgery2, while chronic intestinal failure can have a prevalence of close to 2-4 cases per million inhabitants3. Although rare, it dramatically impacts the patient and their family, and if left untreated, it results in death4-6.
In the latter lies the need not only to consider the vision of the treating team in terms of quantitative variables but also to know the patient’s view of our environment beyond analogous scales, demonstrating a significantly reduced quality of life compared to the healthy population4,7. This work aims to understand the meaning of coping with the intestinal failure condition in our setting. It allows for an approach to the appreciation of the patient as a person and not as a disease, in addition to implementing strategies that facilitate coping with the disease and strengthen support networks that positively impact the reentry of these people into society.
Materials and methods
The research was conducted from a hermeneutic approach using grounded theory techniques such as open, axial, and selective coding8. The study population included patients older than 18 with a diagnosis or history of intestinal failure, treated by the intestinal rehabilitation group of Hospital Pablo Tobón Uribe since 2005, who agreed to participate and signed the informed consent. The exclusion criteria were critical condition, altered consciousness, or mental incapacity to answer the interview. Twenty semi-structured interviews were conducted with 20 participants (Table 1), eight of them in the company of their relatives at the discretion of the interviewees. With prior authorization, they were recorded not to lose information for analysis. Psychological support was also available, given the possibility of exacerbating stressful processes in remembering the situations experienced. In none of the cases was this support required.
Table 1 Consequences include adaptation to intestinal failure as the possibility of getting one’s life back
| Patient | Age | Sex | Year of onset of symptoms | Year of diagnosis | Functional classification** | Admission to intestinal rehabilitation | Pathophysiological classification | History | Longer hospitalization | Transplant candidate |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 36 | M | 2011 | 2011 | III | 2011 | Short intestine | Trauma | One year | Yes |
| 2 | 21 | M | 1997 | 2011 | III | 2009 | Short intestine | Recurrent peritonitis | Two months | No |
| 3 | 47 | F | 2008 | 2010 | II-III | 2017 | Short intestine | Surgical complication | One month | No |
| 4 | 61 | M | 1982 | 1982 | II-III | 1982 | Short intestine | Ischemia | 100 days | No |
| 5 | 47 | F | 2010 | 2014 | II-III | 2014 | Extensive mucosal disease | Crohn’s disease | Three months | No |
| 6 | 65 | M | 2010 | 2010 | II-III | 2010 | Intestinal fistula | Colonic volvulus | Six months | No |
| 7 | 41 | M | 2018 | 2018 | III | 2018 | Intestinal fistula, short intestine | Trauma | 15 days | No |
| 8 | 35 | M | 2015 | 2015 | II | 2016 | Extensive mucosal disease | Immunodeficiency | 15 days | No |
| 9 | 19 | F | 2019 | 2019 | II-III | 2019 | Intestinal fistula, short intestine | Ischemia | 6.5 months | No |
| 10 | 63 | F | 1986 | 2007 | I | 2007 | Short intestine | Multiple peritonitis | Three months | No |
| 11 | 56 | M | 2012 | 2012 | I | 2013 | Short intestine | Multiple peritonitis | 4.5 months | No |
| 12 | 41 | F | 1998 | 2018 | I-II | 2020 | Extensive mucosal disease, mechanical obstruction | Crohn’s disease | Two months | No |
| 13 | 37 | M | 2007 | 2017 | II-III | 2018 | Intestinal fistula, disease | Toxic megacolon, multiple peritonitis, idiopathic | Two months | No |
| 14 | 41 | F | 2019 | 2019 | II-III | 2020 | Intestinal fistula | Intestinal obstruction | Four months | No |
| 15 | 62 | F | 2014 | 2014 | I | 2019 | Mechanical obstruction, intestinal fistula | Neoplastic | Eight months | No |
| 16 | 68 | M | 2017 | 2017 | I-II | 2021 | Intestinal fistula, short intestine | Neoplastic | One month | No |
| 17 | 35 | F | 2007 | 2007 | I-II | 2008 | Short intestine | Ischemia | 1.5 months | No |
| 18 | 57 | M | 2021 | 2021 | I | 2021 | Intestinal fistula, short intestine | Ischemia | One month | No |
| 19 | 28 | F | 2016 | 2021 | III | 2021 | Intestinal dysmotility | Idiopathic | Six months | No |
| 20 | 39 | M | 1993 | 1993 | III | 2017 | Intestinal fistula, short intestine | Multiple peritonitis | One year | No |
**Functional classification: time when the patient required parenteral nutrition. I: weeks; II: months; III: years. Table prepared by the authors.
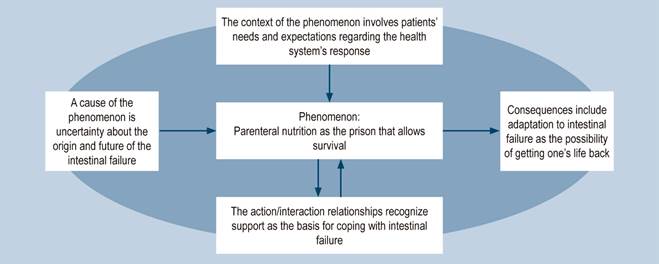
The sampling was initially selective and theoretical in search of variations between the concepts until reaching theoretical saturation (when the new data collection no longer provided additional information)9. The analytical process was carried out with the coding and categorization techniques of the grounded theory. First, the faithful transcription of interviews was completed, from which the codes or first abstractions on the text were identified line by line to inductively group them into descriptive categories, properties, and dimensions for theoretical saturation10. Second, through axial coding, descriptive categories were related, and a phenomenon was detected, describing a context, its causes, action and interaction relationships, and consequences in the paradigm matrix typical of grounded theory (Figure 1).
The analytical process was systematic and interactive between stories, formulated codes, the abstractions that gave rise to the constructed categories, properties, and dimensions, all with the scientific literature reviewed during the research. Triangulation was carried out between researchers, the assumptions from which the researchers started were previously defined, and the analysis limitations were recognized11.
This study was endorsed by the research and ethics committee of Hospital Pablo Tobón Uribe (Minutes 18/2015). Following Colombian regulations, the research proposed in this paper was classified as “risk-free”12.
Results
Parenteral nutrition as the prison that allows survival
The diagnosis of intestinal failure causes either anxiety, fear, and devastation or relief and joy. Feelings depend on experiences, expectations, knowledge, and the ability to assess the implications of the diagnosis. Attention immediately turns to treatment, in which parenteral nutrition plays a fundamental role. The perception of receiving parenteral nutrition is associated with weight gains and losses. It can mean well-being and life or represent a prison for being “handcuffed” to the machine. Management of intestinal failure involves changes to which the person adapts over time.
“(Parenteral nutrition) was for survival […] It’s the hardest thing a human can live because you are tied to one place that you can’t ever leave. It is as if you lost your freedom. It is a jail” (28-year-old woman).
Parenteral nutrition cycling is the opportunity one longs to reach for greater freedom. The news of the withdrawal of treatment may produce joy and be an omen of intestinal recovery. In other cases, it is assumed with fear due to difficulties in reaching goals, previous decompensation, and doubts about maintaining weight. Withdrawal can be abrupt in acute cases, while it is done more cautiously in chronic cases.
“I encouraged myself. If others had to be connected to a machine for 24 hours, I only had to do it for 12” (47-year-old woman). “They let me have it (parenteral nutrition) three days a week, but we were afraid. The doctor was very distrusting, precisely because of the whole process I had already gone through” (41-year-old woman).
Recovery from intestinal failure requires maintaining requirements orally. Suspension of oral feeding when hungry and thirsty can be a challenging experience, in which thinking revolves around food only, and recovering it is a reason for great joy. Conversely, overcoming the fear of eating can be difficult when eating has been associated with intolerance symptoms.
“(Suspension of oral feeding is) hard. I almost went crazy. Those carts passed by distributing the meals to each room and smelled [...] [I was] all year [alone in] a room. No, I wouldn’t have endured it with another person there. Ha! I would have stolen food from them, um, because in the first surgery, I couldn’t [...] drink anything or eat anything either. It was hot, and I got very thirsty. So, in the (shared) room, there was a mango juice drink (of another patient). I went to the bathroom and quietly grabbed the juice and drank it (laughs), and I got scolded” (39-year-old man).
Intestinal transplantation may be an alternative in selected patients to manage intestinal failure. The news of the possibility of an intestinal transplant can cause joy because of the hope of eating again, having greater freedom, and a better quality of life. In other cases, the possibility may be received with bewilderment, anxiety, sadness, stress, or fear due to the implications and risks of complications. The information provided by health personnel in a timely and complete manner is essential to weigh the possible risks and benefits amid uncertainty.
“They told me, ‘Patient,’ you’re going for surgery (for the transplant), and I was happy to know that I was going to [...] be with my family again, to eat again, to walk again, to go out. It filled me with great happiness” (34-year-old man).
The intestinal transplant protocol can be long, while the call to attend surgery is unexpected. The transplant can provide more freedom and a better quality of life, but in other cases, complications recur, freedom is lost again, and it may be necessary to withdraw the transplant. However, the hope for a new attempt may persist.
“The transplant means a better quality of life because one has more freedom [...] I no longer have to think, ‘I have to be at such time at home because I have to be put in a device to feed me.’ Instead, having the intestine implies more freedom. You can eat, you can walk. What happened to the intestine? My body rejected it many times [...] The transplant changed my life, but I spent more time in the hospital than at home [...]. In my experience, with the transplant, there are many infections, many complications, many medications” (34-year-old man).
Patients’ needs and expectations concerning the health system’s response
Patients depend primarily on the public health system for health care, where there are difficulties dispensing drugs or supplies, causing disappointment, sadness, anger, and fear of not achieving health care and its consequences. Patients fight for and insist on the continuity of the service through administrative or legal means.
“It’s very tough because she has a catheter, but I have to get all the supplies to clean her myself” (mother of a 28-year-old woman).
Similarly, health care is mediated by the health team-patient relationship. The patient expects to be listened to without dismissing their needs, notions, and contributions to treatment as the person who lives with the diagnosis and has knowledge from experience. Even in the face of uncertainty and unfavorable prognoses, the patient expects to hear an explanation about their condition and management alternatives and to have their needs met with diligence and empathy. Difficulties in the relationship between the health team and the patient impact care, which arise from the failure to meet expectations: from lack of skill and negligence in physical and emotional care to lack of communication and apathy. In addition, the monotony of health care and exhaustion have a negative influence. A deteriorated relationship results in impotence, anger, despondency, mistrust, and poor adherence. On the contrary, an adequate connection between the patient and the health team gives rise to trust, satisfaction, consolation, and hope, thus favoring management.
“When you arrive at the emergency room, they first say, ‘ha, this one is coming to get some morphine […]’. They did not believe me. I told the nurse, ‘If you empty the reservoir, it will immediately fill with blood […].’ When she withdrew it, I was bleeding heavily, and she immediately ran to look for a surgeon” (37-year-old man).
Moreover, health care can be an economic challenge. Costs are high, while income is declining due to the labor impact of intestinal failure and treatment. Patients may need to work despite limitations, apply for disability pensions, try cost-cutting strategies, or financially depend on their families.
“I had to drive with Uber to cover the drugs the EPS (healthcare operator) did not give me for the fistula. So, I had to work during the day, arrive for the TPN (total parenteral nutrition) at night, and get up early to continue working after I was disconnected. While I am retired, my pension is a minimum wage” (39-year-old man).
Uncertainty about the origin and future of intestinal failure
Intestinal failure is marked by the onset of symptoms that lead to the search for diagnosis and treatment. It can be brief but sometimes significantly slow. Patience is required, but time sometimes breeds exhaustion and deterioration. The disease is accompanied by the uncertainty that runs between hope and fear. Finally, the diagnosis of intestinal failure allows initiation of treatment but may cast doubts regarding the etiology and prognosis. Judgments about the future can deprive patients of hope and inhibit them from moving forward.
“I have had Crohn’s disease since 1998 when some symptoms started, but the diagnosis was clarified, and I started biological therapy in 2016” (41-year-old woman).
“The gastroenterologist told me, ‘She’s never going to eat again. Don’t you ever give her a spoonful of food again [...]’, I left crying. We left because he said, ‘There’s nothing to do. That’s it.’ I went home, but I was eager to continue fighting for her” (mother of a 28-year-old woman).
Hospital stays can become frequent and prolonged. The experience of hospitalization for some is just a change of bed. For others, it is a break from the challenges of daily life. In other cases, it can be overwhelming due to loneliness, isolation, the discomforts it brings, and the suspension of oral feeding while others eat. The need for hospitalization is acknowledged, but home is longed for.
“My lips were dry, cracked. I remember an ad for one (soft drink) that was taken out of a freezer, and gosh! I couldn’t even speak” (65-year-old man).
“I have to be with this bag and empty it. Sometimes the smell is not pleasant [...]. Some patients did tell the nurses (they complained) about the smell and discomfort” (41-year-old woman).
Support as the basis for coping with intestinal failure
The support network arises from affection. It manifests itself in accompaniment, comfort, motivation, understanding, adaptation to the way of life, and addressing needs. It is crucial to cope with intestinal failure, particularly when the patient depends on others for their care. The lack of family support can contribute to deterioration and cause sadness, loneliness, isolation, and a feeling of abandonment.
“He said a few words to me, ‘XX (the wife), you are my cane. If you fall, I fall [...]’, If (you) have no one with you, that’s worse than the disease” (68-year-old man and his wife).
The experience as a companion is challenging, especially in prolonged hospitalizations, due to insufficient space to rest and the need to continue with one’s own life while accompanying the patient. Patients may consider the caregiver’s position more complex than their own and prefer to be visited only to avoid a more negative impact on their relatives. Family members join efforts to cushion the impact and assimilate management. Learning helps them gain independence from health personnel.
“My youngest son dropped out of college. He stayed with me for six months, day and night, by my side” (65-year-old man).
Patients and their caregivers can also support each other, share lessons and experiences, and provide emotional support and assistance in support groups or social media, to the point of making new friends. Although the comparison with other patients gives us a better perspective on their condition, it is understood that each person has individual circumstances. Patients sometimes want to give back to society, prevent the suffering of others, and help in the research of intestinal failure.
“I started making Tik Tok videos of my life. Then, people from the United States, Germany, Spain, Ecuador, Peru, and Argentina began to write that they had also suffered from this condition. I met many people. We learned, and they learned” (28-year-old woman and her mother).
Adaptation to intestinal failure as the possibility of getting one’s life back
Intestinal failure and its treatment can mean carrying out activities that change or interrupt projects and make you question the future, impacting the emotional sphere and vice versa. You feel pain, sadness, and frustration, and sometimes you reach depression with suicidal attempts. Professional and family support is essential.
“I had two suicide attempts. I was very depressed” (39-year-old man). “My and my wife’s projects are to have children, but it has been difficult because they have told us to be aware of genetics” (35-year-old man).
Body image changes due to weight loss, ostomies, fistulas, hernias, and scars. Although this can take a backseat to health or being a source of pride as proof of the process undergone, it may also produce sadness, impotence, and shame. Clothing and other cosmetic changes, such as surgical reconstructions, are made. The improvement of body image engenders motivation and well-being.
“Let my mom tell you (cries) [...]”. “She was a girl with a gorgeous body. Now with these bags and scars [...], we hope the surgeons do everything they can to fix her tummy. More than anything, we want her fistula to close […], as there are things that become irrelevant” (41-year-old woman and her mother).
The family is no stranger to the diagnosis. The diet, the activities, the coexistence, roles, the care of children, the projects, and even the city of residence change. Each member is impacted differently. There may be distancing in family relationships, sadness, frustration, fear, anguish, anger, and exhaustion. Patients sometimes feel guilty and try to lessen the family impact; they comfort, encourage, and try not to worry them. The family may come together out of love to face challenges or distance themselves to avoid them.
“I got disappointed [...]. I had a relationship then, and the person I was with left me... Of course, he would not put up with someone in this situation, but many people also came into my life. Sorry! (cries)” (47-year-old woman).
Intestinal failure brings labor and academic difficulties due to the time required for health care and living with an open abdomen, fistulas, and symptoms that limit activities. Some patients find support in the work environment when the employer understands the need for leaves, medical recommendations are followed, and working conditions are facilitated. In other cases, there is no consideration from bosses or colleagues. Despite trying to adapt by carrying supplies, implementing assistants, and finding spaces to care for their symptoms, the disease and its treatment result in job suspension, dismissals, resignations, or abandonment. Disrupting academic or work projects can impact income and independence and cause sadness and feelings of inferiority. Finally, patients may recognize the need to take a disability pension, which entails difficulty.
“When I already had a fistula, my first job was outside the city. I had to go into the ravines to wash the fistula, and peasants would stare at me. The bosses decided to leave me here in Medellín, but suddenly, I was in a meeting and shat myself” (39-year-old man).
Social life changes. Sometimes patients find understanding, assistance, and support among friends. They also adapt to continue to be socially active. However, in other cases, they may encounter rejection and cruel or reckless comments. The lack of understanding about the condition, added to the limitations, can lead to ending social activities with confrontations, sadness, impotence, and loneliness.
“We walk, and she keeps hiding behind us because she does not want anyone to see her. People start looking at her or nudging each other, which has ended up in fights” (mother of a 28-year-old woman). “I had more or less 20 to 25 bowel movements a day. I barely set foot in a mall because once I went to the restroom and heard people saying, ‘It stinks in here!’ That’s horrible, knowing that you must get out and show your face” (61-year-old man).
Intestinal failure and its treatment can be a long, complicated, up-and-down, life-changing experience. Patients sometimes wish to change their current situation, to have acted differently, or not to have experienced the disease. They feel exhausted, guilty, and helpless, affecting their self-esteem. Some try to face the condition with optimism, resistance, and patience, but sometimes hope is lost. The patient is motivated by the desire to live, religion, children, family, and friends and learns from their care and to live with intestinal failure daily, changing their value system and how they see life and death. Recovery allows resuming activities, projects, relationships, freedom, and hope.
“Life has taught me. I maintain my ostomy and carry my things. Anyway, life taught me” (65-year-old man). “I live very happily. I think God allowed me to be born again, live, enjoy, help many people, and see life differently” (47-year-old woman).
Discussion
The feeling of incarceration at home associated with TPN, as a central phenomenon in coping with the diagnosis, coincides with other qualitative research13,14 in which TPN is consistently associated with loss of mobility and the need for staying at home and making adjustments in daily life, resulting in negative feelings toward the diagnosis and its management13,14. Other authors highlight that home care for administering parenteral nutrition was associated with the perception of greater rigidity in treatment13.
The literature highlights that withdrawal at least one night a week is positively associated with and impacts well-being by resuming social activities and allowing patients to feel free and normal for a night15. Negative feelings are related to the risk of decompensation and not directly to the withdrawal of treatment. Nonetheless, the authors also cite the sensation of fatigue, hunger, and subsequent dehydration, which was not mentioned by the participants in our research15.
About food, research found contradicting perceptions14. The need for food and inappetence and, oppositely, the restrictions on oral feeding and hunger significantly affect patients, as demonstrated by another study in which oral intake was an independent risk factor impinging on the quality of life16.
The alternative to parenteral nutrition in selected cases is intestinal transplantation. As our patients perceived, transplantation is associated with a better quality of life; however, long-term survival is a latent concern17,18, which reinforces the idea of parenteral nutrition as a treatment that, despite providing a lower quality of life, represents the possibility of survival17.
In addition to TPN, hospitalizations can be frequent and prolonged. Some studies describe them as positive because they signify a break from daily difficulties. Still, the perception of being hospitalized as a vital stressor detrimental to life19 predominates, an assessment with which our interviewees agree.
Furthermore, the support network is essential15. It can come from the partner, family, friends, other patients, and even health personnel13,15. The literature suggests that the loss of independence varies according to the health condition, which denotes the feeling of loss of control, adding to the difficulty of asking for help13,14. A correlation has been found between support and scores on the hospital anxiety and depression scale, in which patients who perceived less support had higher levels of negative affect20. Support between patients has been shown to improve scores on quality of life and depression and decrease the incidence of catheter-related infection21. An innovative option is telemedicine support groups, where patients and their families interact in real-time21, and other tools on social media19.
Patients treated with home TPN experience a lower quality of life than the general healthy population and other patients with chronic diseases16,17, which may be related to the negative impression of the diagnosis, the frequency of TPN administration, the restriction in the participation of activities considered valuable and routine13-15, and the etiology of the disease. In the case of intestinal failure secondary to surgical complications, the patients reported a poorer quality compared to other causes22.
Body image is also influenced by intestinal failure and its treatment. In other research, patients mentioned concern about the appearance of the catheter13,14,19, the presence of an ostomy, and the need to hide changes in body image with changes in clothing that, in turn, would allow management13,14,19. Changes in body image increased self-consciousness, adversely affected self-esteem, and caused a loss of confidence that pushed them to reduce social interactions and, thus, increase isolation13,14, as happened with our interviewees.
The authors underline patients’ transition from sadness, frustration, worry, anger, anxiety, discouragement, and even depression to joy and hope15,19. In a study of 85 patients, 56% had clinical levels of anxiety or depression20. In another study, the use of antidepressants was correlated with the volume of parenteral nutrition, so patients with a high volume (three times greater) used antidepressants23. Besides, patients with poor support networks and of working age are more vulnerable to psychological impact20.
From the patient’s perspective, other research has identified the impact at the family level due to their limitation in carrying out activities, difficulty maintaining their role at home, exclusion, feelings of guilt, and concern for relatives distressed by the patient14,15,19. On the family side, 23% of family members reported a moderate to severe subjective burden on the domestic assistance scale24. Among the predictors that negatively influenced the perception of burden is the health condition of the relative of the patient with intestinal failure and the support received from health services24.
Inability to continue working, dismissal, and the need to reduce working hours are frequently reported in the literature13,14, a finding replicated in this research. This is corroborated by lower employment rates after starting TPN, especially in patients with intestinal failure secondary to surgical complications25. The consequences in the workplace have been associated with a negative impact on finances and, more significantly, anxiety and depression15,20, which could be related to the perception of work as a goal, an identity, forced socialization, and a reason to get up in the morning14.
A study with 196 patients found that the time and frequency of infusion, the duration of treatment, the social benefits of employment, the absence of benefits or pension, the intention to work, and age were significantly associated with return to work. The reasons for seeking employment after starting parenteral nutrition were the desire to contribute to society (48%), financial needs (20%), and social aspects (17%)25.
From the patient’s view, others have found different results: the refusal of home visits at night to not interfere with home health care and the impact of TPN on the ability and willingness to socialize due to exhaustion and stress produced by social situations13,14. A study mentioned limitations in movement, primarily due to the presence of an ostomy13. Similar to our findings, another study reported that friends’ lack of understanding of the condition puts friendship to the test15.
Research has referred to teaching care in the hospital but also has pointed out the particular learning of each patient and the adaptations in their personal, family, work, and social spheres for which hospital training is insufficient13. Patients must balance their lives to cope with intestinal failure and parenteral nutrition, sometimes making intestinal recovery possible and freeing them from the limitations imposed by diagnosis and management15.
As limitations, we recognize that the emerging categories might not achieve the same depth since not all researchers have social sciences qualifications.
Conclusions
Facing intestinal failure implies the need for parenteral nutrition, which is perceived as a prison that paradoxically allows survival. The health system does not fully attend to the needs and expectations of patients with intestinal failure, creating uncertainty about the disease’s origin and future. Intestinal failure and its treatment disrupt personal, family, and work life. Social rejection is marked. Family and close people’s support is vital to adapt and revalue life.
Recommendations
Further research is needed on strategies to improve the independence of patients with intestinal failure in managing parenteral nutrition while maintaining safety and effectiveness. Emphasis should also be placed on forming and maintaining safe support networks for the patient and proper psychological assistance.

