











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Proctalgia fugax is defined as recurrent, inconsistent episodes of stabbing rectal pain not associated with defecation for three months. Episodes can last seconds to 30 minutes, disrupting daily activities and waking the patient at night. Once organic pathologies such as inflammatory bowel disease, fissures, thrombosed hemorrhoids, and prostatitis, among others, have been ruled out, a functional pathology must be studied1. Manometry is a diagnostic test that measures pelvic floor muscle function and is helpful in proctalgia fugax. However, results may vary between patients and healthy people and between centers without being standardized2-5.
Moreover, the rectoanal inhibitory reflex (RAIR) should always be observed in anorectal manometry. This reflex is vital since it is modulated by the myenteric plexus of the autonomic nervous system and produced by the release of nitric oxide and vasoactive intestinal polypeptide. Its absence remains the main element for diagnosing Hirschprung’s disease on manometry. Nonetheless, it is also possible not to find it or to find it incompletely in patients with post-circular myotomy and low anterior resection of the rectum6.
Proctalgia is chronic anal pain with an organic or functional origin. Any organic pathology must be ruled out before considering a case of proctalgia fugax. It is believed that anal sphincter spasms, compression of the pudendal nerve, and psychological factors such as anxiety and obsessive-compulsive disorders are related to its appearance. Although some situations, such as sexual intercourse, defecation, emotional stress, or menstruation, can trigger pain, it is not established7. The diagnosis is based on the Rome IV criteria, which require recurrent episodes of anorectal pain unrelated to defecation and lasting only seconds to minutes. Before diagnosis, it is necessary to exclude other causes through tests such as digital rectal examination, laboratory studies, sigmoidoscopy, magnetic resonance imaging (MRI), and transrectal ultrasound (TRUS)4.
Current evidence regarding manometric findings in these patients is not very clear. Some reports show that biofeedback on patients with dyssynergic defecation simultaneously improves the symptoms of proctalgia fugax. The present study aims to approach the manometric characteristics in a sample of subjects with proctalgia fugax and estimate the presence of dyssynergic defecation through anorectal manometry.
Materials and methods
Study design and data extraction
This cross-sectional descriptive observational study included 316 patients with symptoms of proctalgia fugax undergoing anorectal manometry for any indication between 2018 and 2020.
Eligible adult patients had to have complete information on year of birth, age, sex, and active clinical follow-up at each study institution and anorectal manometric evaluation.
Data collection
Information was gathered over four years on different dates in the various hospitals included in the study. Medical records and anorectal manometry results were used as primary sources of information. Sociodemographic and clinical variables such as age, sex, and functional parameters at the anorectal level were collected.
Technical aspects
During the anorectal manometry scan, several parameters are measured to evaluate the function of the gastrointestinal tract. These include anorectal resting pressure, measured over 20 seconds and extended to one minute if ultraslow waves are detected. The maximum voluntary contraction pressure is also measured through three maneuvers of 20 to 30 seconds with 30 seconds of rest between them. Additionally, extrinsic nervous integrity is assessed with a cough maneuver performed with and without 50 mL of air in the balloon. The defecatory maneuver carried out with three attempts and with and without 50 mL of air in the balloon at 30-second intervals is also evaluated. Finally, the RAIR and rectal sensitivity are examined during distension of the rectal balloon, with increments of 10 to 20 mL2.
Definitions
A condition suggestive of proctalgia fugax was considered as a case with a history of recurrent episodes of anorectal pain unrelated to defecation and lasting only seconds to minutes, according to the Rome IV criteria, and which, by medical criteria, had been organic causes were excluded through tests such as digital rectal examination, laboratory studies, sigmoidoscopy, MRI, and TRUS1.
Statistical analysis
The database was created in Excel version 2019. Missing data were filled in with new reviews of data sources, analyzing only complete data at the end. Data were processed using the social science program SPSS version 25.0. We used the median, range, standard deviation, and minimum and maximum values for the descriptive analysis of quantitative variables and absolute and relative frequencies for qualitative variables.
Ethical considerations
The study’s design considered the requirements in the Declaration of Helsinki, version 2013, and Resolution 8430/1993 issued by Colombia’s National Ministry of Health. It was deemed risk-free research, guaranteeing the confidentiality of the information collected. Informed consent was not necessary in its implementation. No records contained sensitive information about the patient’s identity. This research was reviewed and approved by the research ethics committee of each participating institution.
Results
Three hundred sixteen patients were included, predominantly women (65%), with a median age of 45.2 years, a minimum age of 18, and a maximum age of 78 years (Table 1), all with symptoms of proctalgia fugax according to the Rome IV criteria.
Table 1 Baseline characteristics of the patients (n = 316)
| Number of patients (n = 316) | |
|---|---|
| Parameter | Value |
| Age, median (range), years | 45.2 (18-78; DE: 28.3) |
| Sex | |
| Male, n (%) | 98 (31) |
| Female, n (%) | 218 (69) |
Table prepared by the authors.
Manometric parameters
At a manometric level, we found 50% normal pressure, 46% hypotonia of the anal sphincter, and 4% hypertonia; the voluntary contraction test was normal in 76% and abnormal in 24%. A pattern of dyssynergic defecation was documented in 5% of patients, and the most frequent was type I, followed by type III (Figure 1).
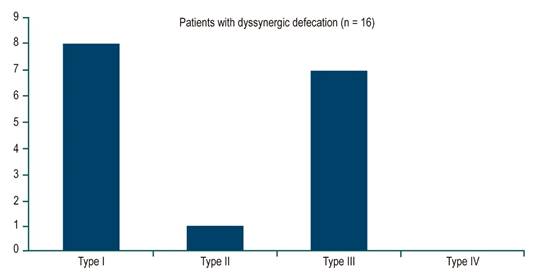
Figure 1 Frequencies of dyssynergic defecation patterns in patients with proctalgia fugax (n = 16). Figure prepared by the authors.
Regarding other parameters, we identified a RAIR in all patients, alteration in the sensory threshold in 42%, and abnormal balloon expulsion in 70%. There was an agreement between the findings of the basal pressures of the anal sphincter by manometry and the subjective report of the digital rectal examination by the head nurse who performed the procedure.
Discussion
When analyzing the variables, it would be expected that proctalgia be associated with elevated levels of resting pressure and contraction of the anal sphincter. Still, only 4% of patients (mostly women) showed hypertonicity; 50% were normotonic, and 46% were hypotonic. This finding suggests that proctalgia is not necessarily related to an elevated and sustained basal contracture of the sphincter nor an alteration in voluntary contraction since most patients in this study had average values.
The diagnosis of proctalgia fugax relies on the symptomatic characteristics and the exclusion of other pathologies as the cause of pain. Physical examination, rectoscopy, and anoscopy results are usually normal in these patients. TRUS and MRI findings are typically normal, although hypertrophy of the internal anal sphincter (IAS) has been recorded in some cases. Anorectal manometry can detect increased tone of the IAS with a paroxysmal lack of relaxation8-10.
Furthermore, dyssynergic defecation is a lack of synchronization between abdominal contractions and the functioning of the anal sphincter, together with insufficient relaxation of the IAS and a paradoxical contraction of the striated sphincter muscles during defecation9,11,12.
There are four types of dyssynergic defecation8,13:
Type I is when the individual can produce adequate intrarectal pressure and pushing force, but there is no anal relaxation; in fact, there is an increase in anal sphincter pressure.
Type II is when the individual cannot produce adequate pushing force, and there is an increase in anal sphincter pressure.
Type III is when the individual can produce adequate pushing force, but anal sphincter relaxation is absent or incomplete with insufficient decrease in anal sphincter pressure.
Type IV is when the individual can produce adequate pushing force, but anal sphincter relaxation is absent or incomplete and has a worse response to biofeedback therapy.
In our study, the manometric findings do not reveal a defined pattern, and this is reflected in this group of patients, in whom the pressure, contraction, and sensory threshold tests are non-specific. Their values may vary in any direction. However, regardless of the cause of this symptom, a pattern of dyssynergic defecation in 5% of patients suggests a correlation with proctalgia fugax. Therefore, two points stand out about the relationship between these two entities: First, the most frequent types of dyssynergic defecation found were types I and III; in both situations, an adequate defecatory effort is generated (increased intra-abdominal pressure). Still, in the former, there is a paradoxical contraction of the anal sphincter. In the latter, the relaxation of the anal sphincter is incomplete or absent, which confirms a non-anatomical functional alteration in the outflow tract or defecatory mechanism, resulting in an abnormal balloon expulsion test in 70% of patients. Second, the RAIR is positive in 100% of patients with proctalgia, and the first sensation or sensory threshold is expected in 58% of patients, indicating that the myenteric innervation and reflex arcs of the lower motor neurons are intact and that the problem is poor muscle coordination in the outflow tract.
Because the most frequent pattern scores in the present study were types I and III, it can be correlated with the data obtained in another study. The literature also mentions that a typical pattern involves an increase in intrarectal pressure accompanied by anal sphincter relaxation. A study of 100 patients using a robust 6-sensor manometry system identified four patterns of functional defecatory disorders (FDD). Two patterns, types I and III, describe dyssynergic defecation. The type I pattern is characterized by an elevation of intrarectal pressure (≥ 45 mm Hg) and anal pressure, reflecting contraction of the anal sphincter. The type III pattern is characterized by an increase in intrarectal pressure (≥ 45 mm Hg) with absent or insufficient relaxation (< 20%) of the anal sphincter. Inadequate propulsion (intrarectal pressure < 45 mm Hg) may be associated with paradoxical contraction (type II pattern) or insufficient relaxation (< 20%) of the anal sphincter (type IV pattern). A test performed a month later showed that the abnormal patterns could be reproduced in 51 of 53 patients9,10.
On the other hand, to treat proctalgia fugax, the literature usually relies on techniques that reduce the pressure of the IAS. The main option is conservative treatments, although no permanently curative results have been observed. These conservative treatments include warm water baths, topical 0.2% glyceryl trinitrate, salbutamol inhalation, local anesthetic block, or injection of botulinum toxin into the anal sphincters. In case of thickening of the IAS and high pressures at rest, considering limited internal anal sphincterotomy is suggested5.
Finally, the study has some limitations that should be noted, including its retrospective nature based on information reviewed from medical records of patients treated in an outpatient setting, which may have affected data accuracy. Due to the scarcity of information in the study, exposure information is subject to measurement error.
Conclusion
The data obtained in the present study suggest that proctalgia is not related to the sphincter’s elevated and sustained basal contracture but to the alteration in voluntary contraction since most patients have typical values.
The RAIR is present in 100% of patients with proctalgia fugax, and the first sensation or sensory threshold is normal in 58% of patients. The preceding indicates that the myenteric innervation and the reflex arcs of the lower motor neurons would be intact and that the problem is possibly poor muscle coordination in the outflow tract. However, we suggest that more studies be conducted to continue providing a scientific basis for the relationship between proctalgia fugax and dyssynergic defecation.

