











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
Introduction
Lipomas are soft tissue tumors derived from mature adipocytes, first described by Bauer in 1757, which are macroscopically and radiologically indistinguishable from normal adipose tissue; epidemiologically, they are the most frequent injuries derived from soft tissues in adult patients, with a slight predominance in male patients1.
Location in the GI tract is infrequent and generally asymptomatic, which can be detected incidentally during surgery, colonoscopy, or autopsy2. Lipomas are often solitary lesions of submucosal origin found in the proximal colon and typically measure less than 2 cm in size, with a maximum diameter of 8.5 cm reported in the literature3). Despite new techniques for radiological diagnosis, the gold standard continues to be a histopathological evaluation that leads to the precise diagnosis of this entity; the manner of removal depends on the manifestation of the case and could result in elective or emergent removal4.
The article reports the case of a female patient who spontaneously expelled part of a giant submucosal lipoma via the rectum and required a secondary laparoscopic resection of the entire surgical specimen.
Case description
A 42-year-old female patient with no significant pathological history consulted for a clinical condition of one year of evolution that had worsened in the previous 12 hours. It was characterized by non-radiating colic-type pain in the mesogastrium, without mitigating or aggravating factors, whose intensity was 5/10 on the visual analog scale. It was accompanied by the expulsion of a soft, non-fouling, yellowish mass through the rectum (Figure 1).

Source: Authors’ archive.
Figure 1 Lipoma expelled rectally with well-defined walls and no signs of bleeding.
Therefore, the patient attended the emergency department. During the interrogation, she reported a condition of intestinal intussusception ten months ago of unknown cause, which self-resolved and required hospitalization for three days. Considering this and the abdominal pain, a contrast-enhanced abdomen CT was requested, describing a lipomatous-type lesion at the ascending colon level (Figure 2).

Source: Authors’ archive.
Figure 2 CT image showing, in different sections, a radiolucent tumor with well-defined edges in the right colon.
In this context, the general surgery service evaluated the patient and suggested a total colonoscopy. It showed a raised, sessile, mamelonated, subepithelial lesion of approximately 6 cm in diameter at the right colon level near the cecum, which occupied one-third of the lumen of the colon (Figure 3).
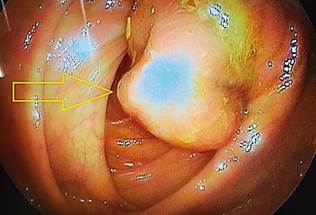
Source: Authors’ archive.
Figure 3 Endoscopic view of a subepithelial lesion occupying one-third of the colon’s lumen.
The final pathological diagnosis of the spontaneously expelled specimen was a lipoma measuring 7 × 5 × 4 cm and weighing 117 g. A medical meeting was held with the gastroenterology and general surgery team, where they determined to perform a laparoscopic resection of the residual lesion, taking into account the history of intussusception less than one year ago and the reports in the literature, which will be addressed in the discussion of this article. A laparoscopic segmental colectomy-type procedure with end-to-end anastomosis was performed using mechanical staplers with negative margins. The patient remains asymptomatic one year after the procedure.
Discussion
Colonic lipomas are benign tumors of mesenchymal origin whose manifestation is exceptional. They are consolidated as the most common benign colonic tumor, only preceded by adenomatous polyps5. Its incidence ranges between 0.2% and 4.4%, with a predominance in the female sex; the age of onset is, on average, between 40 and 50 years. Regarding its location, the most frequent location is the right colon, which represents 65% to 75% of all cases6,7.
Other authors, such as Rogy et al., published a series of cases evaluated over ten years in referral centers and found that lipomas represented 0.3% of colorectal diseases in general and 1.8% of benign colon tumors, with a greater frequency in women, in the right colon, and solitary in 90%; the remaining 10% corresponded to multiple manifestations8.
Generally, these lesions are asymptomatic; however, 30% of large lesions will cause symptoms, especially when they measure more than 2 cm; the most common manifestations include abdominal pain, rectal bleeding, and changes in bowel movements9,10. It should be noted that abdominal pain may be secondary to permanent intestinal intussusception, and the lipoma serves as the head of the intussusception. At the same time, rectal bleeding could be explained by ulceration of the mucosa that covers the lipoma. Unusual complications of colonic lipoma include obstruction, intussusception, perforation, and severe bleeding11.
The clinical significance of lipoma is the high probability of being confused with malignant neoplasms of the colon due to similar characteristics in clinical manifestations; however, no malignant changes associated with this type of lesion have been reported12.
Concerning the diagnosis, the radiolucent characteristics of the fat mean that these tumors can be visualized by CT of the abdomen and barium enema, which makes it clear that it has a low sensitivity to tumors smaller than 1.5 cm; still, the diagnosis is fundamentally endoscopic, which can visualize a fatty, ovoid-looking mass with a specific elastic capacity to return to its initial shape after being pinched with a clamp (pillow sign)8. Since it is below the normal mucosa, a lesion biopsy is not recommended due to the low diagnostic yield. On the contrary, it increases the risks of bleeding and perforation. The gold standard for diagnosing colonic lipoma is based on histopathological diagnosis13.
Treatment varies according to the lesion size; in lesions smaller than 2 cm, endoscopic en bloc resection can be considered; however, surgical resection is recommended in those with a diameter greater than 2 cm due to the risk of existing perforation since fatty tissue is a poor electrical conductor and can increase the risk of complications in endoscopic resection. Usually, lesions with complete resection do not recur, and the procedures are curative. This controversial analysis occurred between the gastroenterology and general surgery teams when choosing the surgical procedure for the patient. Lipomas are benign tumors with null degeneration, so resection is justified to prevent or treat complications8,14,15.
The spontaneous expulsion of a lipoma rectally is rare and practically anecdotal; the mechanism of self-dissection of a lipoma is unknown. It is believed that in pedunculated lipomas, the pedicle could suffer strangulation and subsequent necrosis, causing its detachment. Another way would be the ulceration of the mucosa that covers the lipoma and its exit into the colonic lumen16.
Conclusion
It is important to emphasize that, although the literature is emphatic in taking 2 cm as a cut-off point to choose between endoscopic versus laparoscopic resection, the endoscopic experience curve is currently increasing, which will undoubtedly lead to new consensuses that expand this diameter to attempt more advanced resections. However, in this case, considering that the lesion measured 6 cm, no one on the endoscopic team considered they had the expertise to perform it. If we add the 6 cm of the colonic lesion plus the spontaneously expelled 7 cm, it measures 13 cm, making this case the most giant colon lipoma reported to date.

