











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The indication for a colostomy is varied, yet consistently aims for the prompt closure of the stoma. The perianal region comprises the internal anal sphincter, voluntary striated muscle, external anal sphincter, and the puborectalis part of the levator ani muscle, all of which regulate fecal passage, which are involved in regulating the passage of stool. Furthermore, this region is innervated by the pudendal and inferior rectal nerves, which control sensitivity and muscular activity, and contains connective tissues such as adipose and vascular structures essential for anorectal functionality. Anomalies in these tissues can manifest in symptoms identified through anorectal manometry, including difficult defecation, fecal incontinence, and anorectal discomfort1.
Research indicates that anorectal manometry may forecast the surgical outcomes for anal sphincter repair in fecal incontinence cases, thus influencing colostomy decisions2. Another publication revealed anorectal manometry’s efficacy in evaluating post-surgical continence following colorectal cancer operations, potentially guiding colostomy considerations3. Nonetheless, the variability in preoperative care for these patients poses a challenge in predicting post-stoma removal fecal continence. Ostomy, a surgical intervention that may be temporary or permanent, serves to facilitate elimination (fecal or urinary), nutrition (via food and fluid supply), or oxygenation (through respiratory function maintenance).
The need for colostomy construction often stems from colon obstruction, predominantly caused by either malignant or benign conditions such as obstructive diverticular disease, inflammatory bowel diseases, post-radiation or ischemic colon stenosis. In cases where colon perforation arises from such pathologies, the presence of localized or generalized peritonitis discourages immediate resections and anastomoses. Here, a colostomy, coupled with segment resection, is advised. Colon injury also frequently necessitates colostomy4. Minor, uncontaminated wounds in stable patients might be immediately sutured if addressed within six hours; however, severe trauma, extensive lacerations, devascularized areas, prolonged shock, and concurrent organ damage warrant a colostomy.
Fecal continence does not solely hinge on manometric pressures; patients can exhibit complete continence or experience incontinence despite presenting with low pressure readings. The assurance of anal continence is attributed to the operational synergy of the internal and external anal sphincters, alongside the levator ani muscle, particularly its puborectalis component. A pre-colostomy closure review of these structures’ functionality could enhance the management and outcomes for patients, highlighting the recommendation for anorectal manometry. This diagnostic technique is pivotal for assessing defecation-related issues, such as constipation, fecal incontinence, and functional anorectal pain. Furthermore, it yields invaluable insights during both the preoperative and postoperative phases of surgeries, as well as in evaluating pelvic floor function. Conducting a comprehensive evaluation of the perianal zone’s structure and functionality is crucial for patients exhibiting these symptoms.
Given the significant variability in normal values and the intricate nature of anorectal functions, no singular diagnostic test can encapsulate all the requisite information for an accurate diagnosis and informed treatment decision-making. Anorectal manometry (ARM), through the simultaneous documentation of intraluminal pressure alterations at various levels, facilitates the investigation of anorectal motor activities. This includes both resting states and the simulation of diverse physiological scenarios such as the rectoanal inhibitory reflex, retention efforts, defecation maneuvers, and the Valsalva maneuver. ARM’s capability extends to assessing rectal sensitivity in conjunction with the barostat5, establishing its utility in clinical practice for diagnosing defecation disorders in patients resistant to conventional constipation treatments, evaluating fecal incontinence cases, implementing biofeedback therapy for constipation or fecal incontinence, assessing painful anorectal syndromes, and conducting both preoperative and postoperative evaluations of ileorectal anastomoses. The inclusion of the balloon expulsion test, necessitating equipment capable of rectal balloon distention, further identifies potential candidates for colostomy reversal, particularly those with normal rectal and anal sphincter functions. In such instances, manometry serves as a critical tool in surgical planning, facilitating the selection of appropriate surgical techniques and identifying patients who may benefit from anal sphincter reconstruction6.
The advent of high-resolution and high-definition anorectal manometry has marked a significant advancement in clinical practice in recent years7. These sophisticated techniques, through the employment of proximal circumferential sensors, offer an expanded array of measurement points, enabling a more distinct visualization of rectal and anal pressure fluctuations. The high-resolution and high-definition approach provides a continuous pressure recording capability, offering a more detailed spatiotemporal visualization, unaffected by movements of the pelvic floor.
In light of the absence of Colombian data on the utility of pre-surgical anorectal manometry, this article aims to delineate the manometric findings in patients scheduled for colostomy closure. A cross-sectional study was thus undertaken in two gastroenterology centers within Colombia.
Methods and patient population
Study Design
We conducted a descriptive, observational, cross-sectional study, engaging a cohort of 316 patients who underwent anorectal manometry between 2018 and 2020. Within this cohort, 13 patients were identified as requiring manometry prior to their scheduled colostomy closures across two gastroenterology centers in Colombia.
Data Collection
Data for this study were gathered over a span of two years, from 2018 to 2020, at two Colombian gastroenterology centers participating in the research. Patient medical records and the outcomes of anorectal manometry tests constituted the core data sources. This compilation included sociodemographic and clinical details such as sex and age.
Technical Characteristics
The ManoScan system, provided by Given Imaging, facilitated the ARM procedures. Utilizing a solid-state high-resolution catheter from Medtronic B. V., featuring 10 circumferentially arranged sensors at intervals of 0.6 cm, we employed a disposable ManoShield catheter equipped with an integrated 400 mL rectal balloon. Two of these catheters were inserted within the balloon, situated 3.5 cm above the most proximal of the 10 anal sensors. Placement of the catheter was achieved through the anus in a left lateral position, adhering to a rigorously standardized test protocol. This protocol included assessments for maximum anal compression pressure over three attempts, a 30-second holding capacity across two attempts, defecation efforts (also over two attempts), the rectoanal inhibitory reflex (RAIR), sensation threshold evaluations, and cough reflex tests.
The anorectal manometry explorations examined the following parameters8:
Anorectal resting pressure, recorded over a 20-second duration and extended to at least one minute if slow-wave patterns were detected.
Maximum voluntary contraction pressure, assessed through three 20-30 second maneuvers separated by 30-second rest intervals.
Cough maneuver to assess extrinsic nerve integrity, conducted both with and without 50 mL of air in the balloon.
Defecation maneuver tested through three attempts, both with and without 50 mL of air in the balloon, and 30-second rest intervals.
Anorectal inhibitory reflex and rectal sensitivity, assessed concurrently during gradual rectal balloon distension by increments of 10-20 mL.
Following data acquisition, baseline anorectal manometry readings concerning pressures were analyzed. These encompassed anorectal pressures in resting state, during contraction, and throughout simulated evacuations in the left lateral decubitus position, in addition to RAIR assessments. Metrics such as rectal pressure, rectal pressure increment, anal pressure, anal relaxation, and the rectoanal gradient were evaluated during simulated evacuations. Thresholds for rectal sensation, including first sensation, urge, and discomfort, were also determined. A visual evaluation was conducted to confirm that the increase in anal pressure accurately reflected the contraction’s topography. The balloon expulsion test involved inflating a balloon to 50 mL and observing whether it was expelled within a minute. The protocol and criteria for interpretation remained uniform across all participating institutions.
Statistical Analysis
Data compilation was undertaken using MS Excel 2019. Efforts to address missing data involved revisiting the information sources, leading to analyses solely based on complete datasets. Data processing was conducted using the SPSS software, version 26.0, tailored for social sciences. Quantitative variables were described using median, standard deviation, and the range of minimum and maximum values, while qualitative variables were analyzed based on absolute and relative frequencies.
Ethical Considerations
The study was designed with strict adherence to the ethical guidelines set forth in the 2013 Declaration of Helsinki, Fortaleza, Brazil, and the Colombian National Ministry of Health’s Resolution 8430 of 1993. It was classified as a risk-free research project, ensuring the confidentiality and protection of all gathered information. The nature of the study negated the need for informed consent. Importantly, no patient records contained sensitive identity information. Ethical approval was granted by the research ethics committees of each participating institution.
Results
In a cohort of 316 patients, 13 individuals were identified for manometry prior to their colostomy closure. Predominantly female (69%), the average age within this subgroup was 51.69 years with a standard deviation of 24.18 years. Among them, 8 out of 13 had a history of rectal trauma with associated pelvic injuries, while 5 out of 13 had a previous diagnosis of low rectal cancer. Regarding the type of colostomy, a descending colostomy was performed in 8 out of 13 cases, a sigmoid colostomy in 3 out of 13 cases, and a transanal total mesorectal excision (TaTME) had been carried out in 2 out of 13 cases. Since these patients underwent preoperative evaluations outside the institution, comprehensive medical histories prior to surgery were unavailable (Table 1).
Table 1 Demographic Characteristics of Patients Undergoing Anorectal Manometry (n = 316)
| Number of Patients (n = 316) | Women | Men |
|---|---|---|
| (n = 218) | (n = 98) | |
| Age, median (standard deviation), years | 51.69 (24.18) |
Source: Author’s own research.
Upon assessing the baseline pressures of the anal sphincter (Figure 1), it was revealed that 68% exhibited hypotonia, 16% displayed hypertonia, and 16% demonstrated normal pressures. Voluntary contraction testing yielded abnormal results in 25% of cases, while a pattern of defecation dysfunctions was observed in 30%, all presenting with type III patterns9. RAIR was present in 92% of cases, with abnormal balloon expulsion test results observed in 100% of patients. More than 70% of patients retained their colostomy beyond the first year of its creation, with 30% continuing beyond 36 months. The findings from manometry enabled colostomy closure in 62% of patients exhibiting acceptable continence for both liquids and solids.
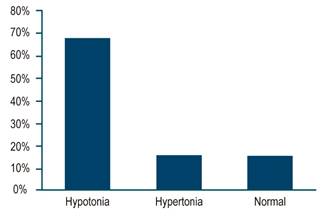
Author’s own research
Figure 1 Baseline Anal Sphincter Pressures in Pre-Colostomy Closure Anorectal Manometry.
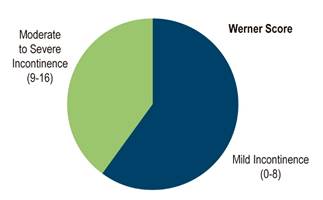
The Wexner score serves as a validated scale ranging from 0 to 20 points, utilized for assessing the severity of fecal incontinence (FI), with 0 representing asymptomatic and 20 indicating complete incontinence10. A threshold of 9 was established to delineate severity, where a Wexner score below 9 denotes mild FI, while a score equal to or above 9 suggests moderate to severe FI8,11.
Upon computing the incontinence index using the Wexner scale (Figure 2), it was found that 60% of individuals exhibited mild incontinence (0-8 points), while 40% presented with moderate incontinence (9-16 points). Remarkably, none of the patients falling into the moderate incontinence category had undergone biofeedback therapy up to the conclusion of data collection. Upon subgroup analysis, among patients under 40 years old (predominantly female), the decision to perform a diverting colostomy stemmed from rectal trauma with associated pelvic injuries. Within this subgroup, manometric assessments revealed a more pronounced decline in pressures, contraction tests, sensory thresholds, dysynergic patterns, and altered balloon expulsion tests compared to patients in an older age bracket, whose ostomies were predominantly indicated for malignant diseases.
Discussion
Manometry stands as the premier approach for assessing continence in those with suspected anorectal alterations. The value of manometric testing lies in its capacity to reduce incontinence risk and inform the correct treatment pathway8,11,12. However, there is an absence of consistent data regarding the efficacy of this examination for patients who are scheduled to undergo colostomies followed by subsequent stoma closure12.
Utilized for appraising pelvic floor disorders affecting the anal and rectal regions, the diagnostic robustness of manometry must be interpreted with caution, as patient and healthy control results may exhibit considerable variability. Normative values can fluctuate across different medical teams since many laboratories set their own reference standards. Variations in resting pressure readings are also attributable to differing methodological approaches. For example, values of 72 mm Hg in men and 65 mm Hg in women have been reported with stationary techniques and microtransducers. Contrarily, other comparable methodologies have yielded readings ranging from 49 ± 3 to 58 ± 3 in women, and from 49 ± 3 to 66 ± 6 in men8,11,13.
The presence of RAIR is imperative to observe during anorectal manometry. This reflex, crucially modulated by the myenteric plexus of the autonomic nervous system and triggered by the release of nitric oxide and vasoactive intestinal peptide, is a key diagnostic marker for Hirschsprung’s disease within manometric evaluations. Its absence, or incomplete manifestation, may also be encountered in patients who have undergone post-circular myotomy and low anterior rectal resection14.
Diverse studies indicate that preoperative maximum compression pressure emerged as an independent predictor for stoma non-reversibility in multivariate analyses. However, preoperative maximum resting pressure and Wexner scores did not share this association15.
It is imperative to recognize that continence impairment in colostomy patients can stem from both the disuse and desensitization of the anal sphincter. Disuse reflects the reduced engagement of the sphincter muscle, while desensitization results from a dysfunctional sphincter due to a disrupted normal defecation reflex. It is widely held that both these factors-disuse and desensitization-can detrimentally affect continence in colostomy individuals. Hence, deployment of anal sphincter rehabilitation techniques is advocated to bolster sphincter function and mitigate fecal incontinence symptoms in colostomy patients16.
Biofeedback, during the temporary stoma period, did not yield symptom improvement. Nevertheless, it was instrumental in preserving sphincter sensitivity and integrity, as well as in curbing the incontinence of liquid stools17. Conversely, the timing of post-colostomy manometry could sway test results. Anorectal function following colostomy is predominantly gauged through manometry, a methodical approach to quantifying the muscular and sensory integrity of the rectum and anal sphincter. Yet, the timing of these measurements can influence the outcomes.
The consensus advises a waiting period of six to eight weeks post-colostomy surgery prior to conducting anorectal manometry. This interval is crucial for scar tissue development and patient adaptation to their modified anatomical and physiological states. Premature manometric evaluations can lead to compromised accuracy due to ongoing inflammation and the body’s ongoing adjustment to post-surgical changes18.
In our cohort, a significant presence of hypotonia at 62%, and a 100% incidence of abnormal balloon expulsion tests were observed, likely a consequence of disuse deconditioning. This finding is in accordance with similar observations noted in the literature. Furthermore, these outcomes suggest that patients have preserved adequate proprioception and voluntary muscular activity. This is evidenced by the fact that 75% of patients had a normal voluntary contraction test and 70% did not exhibit dysynergic patterns, indicating that they maintain effective rectal evacuation capabilities. Sensory-wise, a positive RAIR was present in 92% of the cohort, and a normal sensory threshold was observed in the same percentage of patients, suggesting intact myenteric innervation. A point of concern, however, is that over 70% of these patients, regardless of the initial reason for their colostomy, retained it in situ after one year, and 30% still had it beyond three years. Additionally, colostomy closure was performed in only 62% of patients despite reporting adequate continence for liquids and solids, and interestingly, none had received biofeedback therapy, prompting a reevaluation of the cost-effectiveness of anorectal manometry prior to colostomy closure, especially considering the substantial proportion of patients who did not undergo closure nor receive management for documented manometric changes.
The study does possess limitations, chiefly its retrospective design based on a review of outpatient medical records, which might compromise the data’s integrity. The small sample size subjects the exposure information to potential measurement inaccuracies. Another limitation is the study’s capacity to establish causal links between the variables examined.
Conclusions
Reflecting on the outcomes of this cohort study, one is prompted to question the cost-effectiveness of anorectal manometry prior to colostomy closure given the substantial proportion of patients who continued with an in situ colostomy, and the apparent disconnect between pre-closure manometric data (hypotonia: 68%) and the reported post-closure continence rate of 62%.

