










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista de la Universidad Industrial de Santander. Salud
versão impressa ISSN 0121-0807
Rev. Univ. Ind. Santander. Salud vol.47 no.2 Bucaramanga maio/ago. 2015
Perception of the older adults
regarding the practise of physical
activity and healthy eating
Rodrigo de Rosso Krug1, Aline Rodrigues Barbosa1, Estela Aita Monego1, Ana Lúcia Schaefer Ferreira de Mello1,
Vivian Francielle França1
1. Universidade Federal de Santa Catarina. Florianópolis, Brasil
Correspondence: Aline Rodrigues Barbosa Address: Departamento de Educação Física - Centro de Desportos, Universidade Federal de Santa Catarina —Campus Trindade — Florianópolis, SC — Brasil.
Email: aline.r.barbosa@ufsc.br. Phone: +55 48 37219368
Received: August 26 of 2014 Approved: March 3 of 2015
Suggested citation: Rosso Krug R, Rodrigues Barbosa A, Aita Monego E, Schaefer Ferreira de Mello AL, França VF. The perception of the older adults regarding the practice of physical activity and healthy eating. Rev Univ Ind Santander Salud. 2015; 47(2): 115-124.
RESUMEN
Objective: To understand the perception of regular physical activity and healthy eating among the older adults. Methods: This descriptive study (qualitative approach) included 36 older adults (69 to 91 years) residents in a rural community in southern Brazil. A semi-structured interview was used and the information were recorded, transcribed and interpreted (content analysis technique). Results: The following categories of analysis were identified: a) facilitators and barriers for the practising PA, b) benefits of regular PA, and c) healthy eating habits-consumption of food (beneficial and harmful for health). Facilitating factors were related to social interaction, motivation, willpower, practise enjoying, having company, and being encouraged. Barriers perceived were diseases, physical limitations, pain, lack of willingness and age. The PA benefits were wellbeing, pain reduction, increased willingness, treatment and disease prevention. Fruits, vegetables, vitamin D, calcium, and water were cited as important to health. The consumption of foods rich in fat and sugars was associated with the occurrence of diseases. Conclusion: Personal aspects, of coexistence and motivation, are factors cited as facilitators for the practise of physical activities, while the barriers are related to health, unwillingness, and age. Health promotion strategies may be multidisciplinary and should consider personal aspects, of coexistence, motivation and health. Strategies should focus on the benefits of regular PA and healthy eating.
Keywords: Aging; Health Behavior; Motor Activity
La percepción de las personas mayores sobre la
actividad física y la alimentación saludable
RESUMEN
Objetivo: Estudiar la percepción de las personas mayores en la actividad física (AF) regular y la alimentación saludable. Métodos: El estudio (cualitativo, descriptivo) fue realizado con 36 ancianos (69-91 años) residentes en una comunidad rural en el sur de Brasil. Las entrevistas fueron grabadas (cuestionario semi-estructurado), transcritas y analizadas utilizando la técnica de Análisis de Contenido. Resultados: Se identificaron 3 categorías de análisis: a) los factores que facilitan y las barreras para la práctica de AF; b) los beneficios de la AF regular y, c) dieta saludable: el consumo de alimentos buenos y malos para la salud. Los factores facilitadores fueron la fuerza de voluntad, disfrutar de la AF, tener compañía y recibir incentivos. Los ancianos consideraron como barreras las enfermedades, limitaciones físicas, dolor corporal, falta de voluntad, el aumento de la edad. Los beneficios citados fueron el bienestar, la reducción del dolor corporal, aumento de la disposición, tratamiento y prevención de enfermedades. Los adultos mayores consideraron las frutas, verduras, vitamina D, calcio y agua importantes para la salud. El consumo de grasas y azúcares han vinculado a enfermedades y restricciones en la dieta. Conclusión: Los aspectos personales de la convivencia y la motivación son considerados como facilitadores de la actividad física, mientras que las barreras están relacionadas con la salud, la falta de deseo y la edad. Estrategias para la promoción de la salud deben ser multidisciplinarias, considerar los aspectos personales de la vida, la motivación y la salud, centrándose en los beneficios de la AF y la alimentación saludable.
Palabras clave: Envejecimiento; Conductas saludables; Actividad Motora
INTRODUCTION
Human aging is a process of progressive and differential degradation resulting from the interaction of endogenous and exogenous factors throughout life. Changes with the advancement of age do not follow a chronological age and occur at different rates in relation to biological, psychological, or sociological aspects. Much of the decline associated with aging may be a result of individual lifestyle rather than a particular and inevitable characteristic of that process1. In this context, physical activity and nutrition stand out as significant modifiable risk factors for chronic non-transmissible diseases2.
The progressive reductions related to biological aspects, as well as psychological and social changes resulting from human aging, contribute to the low level of physical activity among older people3. In addition, biological and physiological changes in the digestive system, the occurrence of chronic diseases, and social and psychological factors may impact dietary habits and nutrient demand4,5.
According to a national survey conducted by the Ministry of Health in the 26 Brazilian state capitals and the Federal District, 73.1% of people over the age of 65 are physically inactive6. Physical inactivity may lead to reduced functional capacity, loss of quality of life, increase in diseases, obesity, and mortality7.
The eating habits of the older adults are associated with their health condition. A balanced and varied diet rich in fruits and vegetables and low in saturated fat, meat, dairy products, refined grains, and sweets is important in meeting nutrient needs and preventing or controlling chronic diseases8.
In the health-promoting action, it is important to consider physical activities that older people enjoy as well as facilitating factors, perceived barriers, and benefits of regular physical activity and healthy eating. These points can help in developing and supporting strategies that facilitate this population's adherence to physical activity and adoption of healthy eating habits. The older adults are a specific group and may have different perceptions or difficulties in their daily lives that hinder the incorporation of healthy eating habits.
In this sense, the present study aimed to understand the perception of regular physical activity and healthy eating among the older adults in a rural community in southern Brazil.
PARTICIPANTS AND METHODS
This is a descriptive study with a qualitative approach. This study is part of a home-based epidemiological survey('The effectiveness of physical activity and nutrition actions for older adults of the municipality of Antônio Carlos, Santa Catarina') carried out with a representative sample of older adults (60<-79 years; n = 343) and all oldest (n = 134) residents in the municipality of Antônio Carlos, Santa Catarina, southern Brazil (n = 477).
In the present study, the sample consisted of 36 older adults (8 men) between 69 and 91 years old who participated in social groups. The number of participants was defined by the criterion of data saturation. The technique used to collect information was a semistructured interview (2011). The interview consisted of guiding themes related to the general objective of this study, namely the identification of regular physical activity, factors that limit or hinder regular physical activity, factors that contribute to or motivate physical activity, benefits of regular physical activity, eating habits, and health.
The interviews were recorded and transcribed for later analysis. The information collected in the interviews was interpreted following the content analysis9 technique, which includes three stages: a) pre-analysis, b) exploration of the material, and c) treatment of the result.
In pre-analysis (Stage 1), a 'superficial reading' of the raw data was initially performed, hypotheses were formulated, and the indicators to be used in the next stage were defined. Indicators were defined as the factors that contribute to or limit the performance of regular physical activity and the perceived benefits and aspects of healthy eating.
The second stage, exploration of the material, comprised the operations of codifying and categorizing the textual content. The raw data (units of analyses) were transformed into themes. For the composition of categories, themes were sorted by similarity or differentiation. The exploration continued with the ordering of themes, according to how they were revealed in the textual content. This stage was carried out separately by two researchers. The first carried out the process manually and the second using the programme ATLAS Ti.
In the third stage, treatment of the results, inferences and interpretations were drawn on the alreadyprocessed data by qualitatively analysing the themes and categories that constituted the perception of the older adults with regard to regular physical activity and healthy eating.
The research was approved by the Ethics Committee on Human Research at the Universidade Federal de Santa Catarina (Process No. 189/09).
RESULTS
The majority of the participants were literate (n = 30), worked in agriculture (n = 29), and lived with others (n = 33), did not work at the time of the interview (n = 34). According to the older adults, walking and dancing were the physical activities more practised for leisure. In the words of older adults:
- "(…) eu caminho pela estrada quando eu tenho tempo (…)uns duzentos metros de rua (…)" [Interview 12]; "(…) caminhar faz bem, eu caminho bastante, desço morro, subo morro (…)[Interview 10]; "Eu caminho, o médico disse que tem que caminhar, tem que fazer todo dia, pra bom, eu acho legal.[Interview 23]; "É, eu faço caminhada todo dia direto[ Interview 7];"(…) eu faço caminhada uma hora por dia.[Interview 15]; "(…) tinha um tempo que eu andava na estrada, mas fizeram o asfalto, e então me dava labirintite e daí eu caia (…), ai então eu falei pra o meu médico, daí sabe o que ele disse? Ele disse que eu fizesse em casa, ligasse a televisão ou o rádio, uma música bonita, e ficasse ali dançando uma hora toda (…) e isso eu tô fazendo, todo dia." [Interview 34].
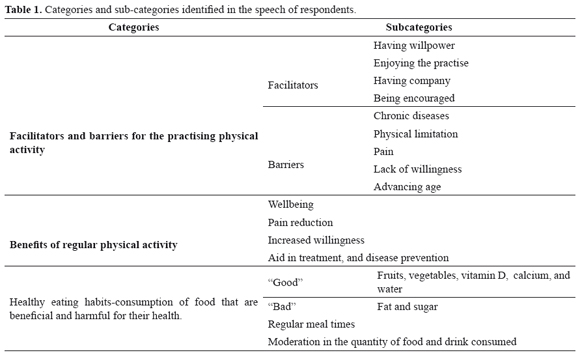
The following categories of analysis were identified in the study: a) facilitators and barriers for the practising physical activity, b) benefits of regular physical activity, and c) healthy eating habits-consumption of food that are beneficial and harmful for their health. The content of the categories and subcategories are shown in Table 1.
The facilitating factors that were mentioned were personal, related to social interaction, and motivation, with having willpower, enjoying the practise, having company, and being encouraged as sub-factors. For example, some participants stated:
- "(…) se não tem vontade não pode fazer nada." [Interview 3]; "(…) quem quer fazer tem que ter a força de vontade prá fazer[Interview 5]; "Se não tiver vontade também não faz.[Interview 8];"(…) se você não tem vontade você não vai fazer." [Interview 15]; "Tem que ter vontade." [Interview 21]; "É, a gente tem que ter a força de vontade, senão a pessoa logo cansa, não faz mais.[Interview 34]; "Precisa ter força de vontade, porque precisa força de vontade pra tudo, tem que ter vontade de faze, se esforçar.[Interview 36].
- "(…) eu acho também que fazer contra o gosto da gente não adianta, tem que gostar do exercício que faz.[ Interview 26]
- "(…) tem que ser em turma, sozinha eu não, não faço." [Interview 17].
- "(…) se alguém incentivasse, parece que era um pouco melhor pra fazer." [Interview 7]; "(…) sem ser incentivada, a gente não faz tanto (… )'não faz certinho, é porque a gente esquece às vez, como faz". [Interview 24]; "A gente tem bastante ajuda aqui, da nossa coordenadora, ela ajuda bastante, e aí a gente vai praticando, vai fazendo." [Interview 32]
Willpower
Enjoying the practise
Having company
Being encouraged
The barriers perceived by respondents were also personal, including health-related issues (diseases, physical limitations, pain) as well as lack of willingness and age. For example, in the words of some older adults:
- "(…) eu não consigo fazer, por causa do meu coração, eu não posso me esforçar, eu tenho problema no coração, e já me deu um AVC, um lado do rosto tá paralisado, essa mão tá paralisada, aí eu não posso me esforçar." [Interview 5]; "Eu fazia todas as atividades, mas daí eu peguei hepatite, e fiz tratamento, fiquei doente um ano, mas agora eu não consigo mais (…)" [Interview 8]; "Eu faço, só que eu não posso fazer muito esforço, por causa do coração, mas eu fazia sempre, bem!" [Interview 15]; "(…) eu ando um pouco, vou de apé pra igreja, até lá embaixo na volta, só quando dá, porque eu tenho problema nos dois joelhos, tenho problema na coluna, que não posso operar (…)" [Interview 29]; "(…) eu não posso porque eu tenho platina no braço, platina na perna, (…) mas eu gosto sim, eu trabalho o dia todo, faço o que posso fazer (…)" [Interview 12]; "Não faço, nem todas, com a minha coluna eu preciso saber, eu tenho que cuidar o que eu faço, eu tenho bico de papagaio, tenho desvio de coluna." [Interview 32]; "A gente levanta de manhã com o braço doendo, tem muita dor nesse braço também, eu acho que chama bursite, não sei o que é isso, mas eu não tomei remédio pra isso, ainda, vamos ver o que o médico vai dizer agora." [Interview 29]; "Eu ando um pouco antes de meio-dia, uma voltinha em redor de casa, longe não posso ir (…) mas quando chego em casa, aí sinto meio dor no corpo (…)" [Interview 30].
- "Tem pouca vontade, depois fico cansada, outro dias às vezes nem vou mais, mas vou, andando, vivendo assim." [Interview 30]; "(…) eu andava muito de bicicleta, andava bastante, mas ultimamente fico muito cansada, não dá." [Interview 8]
- "(…) a gente é um pouquinha relaxada, nem todo dia a gente tá com aquela, sabe, porque a gente tem essa idade (…)" [Interview 36]; "(…) com essa idade, a gente não tem mais aquele pique de caminhar (…) porque a minha idade já tá pesando (…)"
Health-related issues
Lack of willingness
Age
The respondents were able to perceive several benefits of physical activity. The subcategories revealed were as follows: wellbeing, pain reduction, increased willingness, aid in treatment, and disease prevention. For example, some older adults stated:
- "(…) dá mais energia!" [Interview 1]; "(…) a gente fica mais disposto, caminha melhor (…)" [Interview 2].
- "(…) se eu fico uma tarde sentada sem fazer exercício eu fico toda dolorida." [Interview 17]; "(…) dói as pernas, e eu tenho varize, com o exercício eu acho que alivia um pouco as pernas." [Interview 22].
- "(…) de manhã, quando eu levanto eu faço exercício no meu quarto, porque daí eu me relaxo, faço um monte (…)." [Interview 36].
- "Ah, se não fizer exercício dá doença sim." [Interview 9]; "(…) se a gente fica encarangado tudo quanto é doença aparece." [Interview 15]; "(…) eu assisto muito o Jornal e tem os médicos que falam que tem que fazer exercício pra não ter doença." [Interview 16];"É bom pro coração, é bom para os músculos, para tudo é bom, e quando não faz pode dar algum problema de saúde." [Interview 26]; "(…) se não fazer pode dar doença né." [Interview 28]; "O sangue circula melhor quando faz." [Interview 31]; "Pode contrair doenças, se não se esforçar, se ficar de molho pode contrair." [Interview 32].
Wellbeing
Pain reduction
Increased willingness
Aid in treatment, and disease prevention
The perception of the respondents in relation to eating habits incorporated the classification of 'good' and 'bad' foods for health. The older people valued fruits, vegetables, vitamin D, calcium, and water as important to health. In the words of some participants:
- :"tem que comer verdura (…) fruta, tudo né." [Interview 12]; "(…) nós comemos muito light, muita verdura, lá em casa não tem um dia que nós não tem duas, três qualidade de verdura na mesa, e colhido orgânico, lá em casa no quintal." [Interview 15]; "(..) um dia eu como salada, alface e coisa, outro dia eu como uma banana (…)" [Interview 30]; "(…) eu como, é laranja, (…) verdura eu como muito, eu como aquela verdura crua, couve né, e é brócole, é tudo que é de verdura né, é isso vai por cima da comida, depois eu pico e passo por cima da comida, cruzinho né, e isso tá me ajudando bastante." [Interview 34]; "Ah eu sempre cuido, como bastante salada, como verdura, eu cuido o que que eu como." [Interview 31]; "(…) eu estou me alimentando, pro meu corpo, eu me sinto bem, é a banana, é o abacaxi, é bastante fruta, bastante verdura, no quintal eu colho pra mim." [Interview 32]; "(…)quando a gente era mais nova, a gente comia tudo assim, que a gente gostava né, agora a gente já escolhe as coisas que tem mais, né, que tem mais vitamina D né." [Interview 34]; "Porque eu sofro de osteoporose , né, então eu tenho comer muita coisa, muita coisa que tem, como se diz, cálcio." [Interview 35]
The consumption of foods rich in fat and sugars was associated with the occurrence of diseases, as stated by some respondents:
- "É, a gente tem que cuidar muito o que a gente come, porque eu cuido muito, não como gordura, nada, e essas coisas assim, eu cuido o máximo, prá não dar doenças." [Interview 5]; "(…) tem alguma coisa às vezes que a gente tem que cuidar na comida prá sentir bem, porque a gente, as vez, diz olha gordura não faz bem pra saúde comer essas coisas, então a gente evita né, come as coisas que a gente acha que faz bem." [Interview 10]; "(…) a comida que provoca colesterol, uma coisa assim, já principalmente quem tem esses problemas tem que cuidar com isso, tem que cumprir a dieta." [Interview 24]; "(…) nós tamos cuidando do sal, tamo cuidando da gordura, como a gente escuta na televisão (…)." [Interview 3]; "(…) desviar mais a gordura, essas coisas, mais pra salada." [Interview 16]; "A gente tem que evitar muita coisa, gordura né." [Interview 19]; "tem que diminuir os doces, eu tò muito no doce." [Interview 9].
Furthermore, the notion of healthy eating included the need to maintain regular meal times and moderation in the quantity of food and drink consumed. In the words of some older adults:
- "(…), a gente trabalha na roça (…), então aí sabe como é que é, não tinha hora certa, e isso tudo eu sinto que prejudicava a gente, eu, um dia me deu uma gastrite, no estômago, foi só o negócio de jantar, almoçar, fora de hora." [Interview 2]; "(…) tudo quanto é doença, tudo quanto é mal que vem, entra pela boca (…)". [Interview 32]; "Então, alimentação, eu tenho que diminuir a minha alimentação." [Interview 2] ; "É, pelo que a gente tá vendo, as vez já era melhor se a gente tivesse umas coisas mais leve pra comer, aí a gente mora longe, daí eu saio, eu vou comprar umas coisas que é mais leve." [Interview 32].
DISCUSSION
The testimony of the participants showed that walking and dancing were the most popular activities. This result was expected, as walking can be practised freely without specific professional advice, and dancing is a part of the meetings of the municipality's social groups. These two modalities can lead to physiological, social, and cognitive benefits10,11. Walking has positive effects on muscle strength, blood pressure, lower limb pain, arthrosis and arthritis, physical fitness, and aesthetics and results in an increase in willingness, wellbeing, and mood10. In addition, walking contributes to socializing11, as it is one of the physical leisure activities that is practised the most by the older adults in different communities12,13. According to the review study of Keogh et al.14, there is evidence that dance can improve older individuals' aerobic power, balance, agility, walking speed, flexibility, and lower limb muscular strength and endurance.
Facilitators and barriers for the practising physical activity
The results showed that the facilitating factors for the practise of physical activity were having willpower, having company, being encouraged, and enjoying activities. Willpower is related to the motivation to adhere to the regular practise of physical activity15 and may be affected by the individual's health. It is appropriate to recommend and offer specific alternative forms of physical activity that can motivate individuals with different health conditions to begin and sustain physical activity16.
Other studies have also identified that having company (sociability) and enjoying physical activity are motivating factors in the practise of physical activity11,17. Performing physical activities with company or in groups can motivate involvement in physical activities and improve social involvement and coexistence among friends11,18. Increasing sociability is an important point to be considered in proposing physical activity programmes, since the loss of social involvement is a problem in aging, especially after retirement.
For the participants in this study, receiving incentives facilitates the practise of physical activity. The encouraging people, who practise, have practised, or do not practise, can facilitate regular physical activity19,20. Positive reinforcement can make older individuals feel that their efforts are valued, and they will be more likely to continue practising physical activity21.
The presence of any disease, physical limitation, or pain was the barrier cited by the respondents and is consistent with the literature19,22. The prevalence of nontransmissible chronic diseases is a common condition in the older individuals. In Brazil, only 22.6% of the people who are 60 years or older, do not have any type of chronic disease23. It is important to note that having a chronic disease says nothing about the disease's seriousness or stage. People can live with certain diseases without being chronic patients. The problem is when the disease impairs the performance of daily activities24. Physical limitations usually result from chronic diseases and may lead to functional restriction and disability3. An individual with poor health will likely practise less physical activity than an older person in a better state of health15,18. Regular physical activity improves health and reduce overall risk of musculoskeletal pain and disability1,3.
Pain is a subjective and personal feeling dependant on the individual's sociocultural, psychological, environmental, and family characteristics. Although it is a limiting condition, pain is not a consequence of aging25. Physical demand, intensity, and fitness level of the individual or even the presence of a health problem, such as arthritis, can lead to some pain when performing physical activity. However, the practise of enjoyable and safe physical activity is possible for most individuals. When proposing physical activity programmes, the physical condition of each individual should be considered, while offering different activities at different fitness levels.
The results also revealed that age and lack of willingness were other perceived barriers. Unwillingness is a barrier for practising physical activity that is consistently observed in studies involving the older participants18,26,27. While it may be argued that this is an excuse for not practising physical activity, this barrier (psychological or emotional) exits for the person living it16. It is important that the measures aiming to promote physical activity, in addition to seeking to identify the causes and patterns of unwillingness, explain that physical activity itself may increase this willingness and that activity does not need to be strenuous to bring about health benefits27.
Although reduced levels of physical activity with advancing age is a common condition observed everywhere in the world28, aging should not become a barrier to the practise of physical activity. This reduction is partly due to the natural decline in the functions of biological and physiological parameters, which affects their 'motivation' to practise physical activity29. Other factors such as reduced muscle mass and presence of disabling diseases, which hinder joint movements3, contribute to this reduction.
Benefits of physical activity
According to the perception of the respondents, welfare, pain reduction, increased willingness, and aid in the treatment and prevention of diseases are benefits of physical activity. The sense of wellbeing can be considered an intrinsic motivation (i.e. the execution of the activity results in satisfaction with having executed it)21. The regular practise of physical activity increases the production of beta-endorphins and biogenic amines that act on the nervous system, producing pain relief and feelings of wellbeing, and improve the individuals' self-esteem30. Any activity that increases blood flow for a sustained period will release endorphins and relieve pain31.
The therapeutic and preventive role of physical activity is well established in the literature. According to several review studies7,32,33, regular physical activity reduces the risk and/or progression of cardiovascular disease, stroke, diabetes, hypertension, cancer, arthritis, arthrosis, osteoporosis, chronic obstructive pulmonary disease, chronic renal failure, anxiety, depression, and dementia. Furthermore, physical activity can improve cholesterol and high-density lipoprotein levels, control hyperglycaemia, and reduce the risk of cancer and functional limitations, among others.
Healthy eating
The perception of the respondents in relation to healthy eating identified fruits, vegetables, vitamin D, calcium, and water as important to health, and food sources of fat and sugars were associated with the occurrence of diseases. The need to maintain regular meal times and moderation in food and beverage intake was also perceived.
The consumption of fruits and vegetables is associated with reduced risk of major chronic degenerative diseases34,35 because of the supply of vitamins, minerals, antioxidants, and dietary fibre. In 2004, the World Health Organisation2 suggested an increase in fruit and vegetable consumption as part of the Global Strategy on Diet, Physical Activity, and Health. In Brazil, the food guide created by the Ministry of Health (10 steps for healthy eating in older adults ) recommends daily consumption of at least three servings of vegetables as part of meals and three or more servings of fruits daily8. Despite the recommendations, data from the Brazilian Consumer Expenditure Survey (Portuguese acronym POF) 2008—2009 show that less than 10% of the Brazilian population achieves the recommended intake of fruit and vegetables36.
Water consumption, mentioned by the older adults as essential to health, is a habit that should be encouraged. The older adults have a decreased thirst sensation, and the frequent use of diuretics makes these individuals more susceptible to dehydration and changes in fluid balance4. The recommended intake of at least two litres (six to eight glasses) of water per day is also part of the 10 steps for healthy eating in older adults8.
The respondents perceived fat intake as bad for health. Unhealthy or 'bad' fats are saturated and trans fat. While saturated fats are found mainly in products of animal origin, industrialised foods are the source of trans fat. Excessive consumption of saturated and/or trans fat can lead to dyslipidaemia and cardiovascular and brain diseases2. The nutritional recommendations encourage the removal of visible fat from meat and poultry skin before processing as well as reducing fatty food consumption to, at most, once a week8.
Vitamin D and the mineral calcium were mentioned as important in preventing osteoporosis. The combination of calcium and vitamin D has been the primary treatment for osteoporosis, although other minerals and hormones are involved in the pathophysiology of bone loss. Inadequate calcium intake can lead to loss of bone mineral density, predisposing the patient to an increased risk of fractures and osteoporosis37. In Brazil, according to data from POF 2008—2009 36, calcium was one of the nutrients with the highest percentage of inadequacy in older adults of both sexes. Vitamin D is involved in the metabolic pathway of calcium, and its supplementation has been associated with increased bone mineral mass38.
According to the respondents of the present study, it is necessary to reduce the consumption of 'sweets'. POF data (2008—2009) showed that the consumption of sugar among the older adults was low, as was the consumption of sandwich cookies, but individuals from rural areas showed higher per capita acquisition of sugar. The consumption of honey and added sugar, although low, was higher among the older adults compared to other age groups investigated36. Changes in taste buds with advancement of age4 may be responsible for this characteristic of adding sugars. The recommendations8 suggest that the consumption of sugary foods, including soft drinks, processed juices, cakes, sweet and sandwich cookies, desserts, sweets, and candy should be restricted to twice a week.
FINAL CONSIDERATIONS
Based on the reports, it is clear that the participants identify several benefits of the regular practise of physical activity, and relate it to health and wellbeing. Personal aspects, of coexistence and motivation, are factors cited as facilitators for the practise of physical activities, while the barriers are related to health, unwillingness, and age. That is, the results suggest that the personal and socio-cultural aspects affect the practice of physical activity, as well as health status. Therefore, knowing your population is essential to understanding their practical experience in a range of lifespan physical activities 39.
According to the perception of the participants, healthy diet is focused on the need for care in everyday life because of the relationship with diseases. However, no reference was made to salt consumption, an important factor in relation to hypertension, the most prevalent disease in the older adults of Antônio Carlos40.
The perception of the participants provides a variety of information related to physical activity and healthy eating. The type of research (qualitative) does not allow us to say to what extent the perceived factors actually inhibit or facilitate the behaviour of the older adults and does not identify the real benefits of physical activity and healthy eating. These should be checked by means of longitudinal studies. However, the results suggest the need for greater dissemination of information about the importance and benefits of physical activity and healthy eating for the older individuals. The results were used to develop a guide to physical activity and healthy eating for the older adults that was distributed to all individuals (≥ 60 years) in the municipality. Furthermore, the information was presented and discussed with the staff involved with primary health care in the municipality as part of the proposal of strategies to promote physical activity and healthy eating for older adults. We believed that the information may be useful to health professionals to propose strategies to promote physical activity and healthy eating. An approach to physical activity and healthy eating promotion should recognize and targeting the societal values and cultural perspectives that extend beyond health41. The facilitating aspects should be focused, and the barriers can be discussed in order to mitigate them.
ACKNOWLEDGMENTS
The research was supported by the Brazilian National Council of Technological and Scientific Development (CNPq- Process 478073/2009-7).
REFERENCES
1. Schroll M. The main pathway to musculoskeletal disability. Scand J Med Sci Sports 1994; 4(1): 3-12. [ Links ]
2. World Health Organization (WHO). Global strategy on diet, physical activity and health. Genebra: World Health Organization; 2004. [ Links ]
3. Von Bonsdorff MB, Rantanen T. Progression of functional limitations in relation to physical activity: a life course approach. Eur Rev Aging Phys Act 2011; 8(1): 23-30. [ Links ]
4. Ahmed T, Haboubi N. Assessment and management of nutrition in older people and its importance to health. Clin Interv Aging 2010; 5(8): 207-216. [ Links ]
5. Saka B, Kaya O, Osturk GB, Erten N, Karan MA. Malnutrition in the elderly and its relationship with other geriatric syndromes. Clin Nutr 2010; 29(6): 745-748. [ Links ]
6. Brasil. Ministério da Saúde. Vigitel. Vigitel Brasil 2010: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2011. [ Links ]
7. Mechling H, Netz Y. Aging and inactivitycapitalizing on the protective effect of planned physical activity in old age. Eur Rev Aging Phys Act 2009; 6(2): 89-97. [ Links ]
8. Brasil. Ministtério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Alimentação saudável para a pessoa idosa: Um manual para profissionais de saúde. Brasília: Editora do Ministério da Saúde, 2009. [ Links ]
9. Bardin L. Análise de Conteúdo. Lisboa, Portugal: Ed. Porto LDA; 2009. [ Links ]
10. IH Jonsdottir, L Rodjer, E Hadzibajramovic, M Borjesson, G Ahlbor Jr. A prospective study of leisure-time physical activity and mental health in Swedish health care workers and social insurance officers. Prev Med 2010; 51(5): 373-377. [ Links ]
11. Meurer ST, Benedetti TRB, Mazo GZ. Teoria da autodeterminação: compreensão dos fatores motivacionais e autoestima de Interviews praticantes de exercícios físicos. Rev Bras Ativ Fís Saúde. 2011; 16(1): 18-23. [ Links ]
12. Inácio FR, Salvador EP, Florindo AA. Análise descritiva da prática de atividade física no lazer de Interviews residentes em uma região de baixo nível socioeconômico da zona leste de São Paulo, SP. Rev Bras Ativ Fís Saúde. 2011; 16(2): 150-155. [ Links ]
13. Hughes JP, McDowell MA, Brody DJ. Leisure- Time Physical Activity among US Adults 60 or More Years of Age: Results from NHANES 1999- 2004. J Phys Activ Health 2008; 5(3): 347-358. [ Links ]
14. Keogh JWL, Kilding A, Pidgeon P, Ashley L, Gillis D. Physical benefits of dancing for healthy older adults: a review. J Aging Phys Act. 2009; 17(4): 479-500. [ Links ]
15. Reichert FF, Barros AJD, Domingues MR, Hallal PC. The role of perceived personal barriers to engagement in leisure-time physical activity. Am J Public Health. 2007; 97(3): 515-519. [ Links ]
16. Toscos T, Consolvo S, McDonald DW. Barriers to physical activity: a study of self-revelation in an online community. J Med Sys 2011; 35(5): 1225- 1242. [ Links ]
17. Freitas CMSM, Santiago MS, Viana AT, Leão AC, Freyre C. Aspectos motivacionais que influenciam a adesão e a manutenção de Interviews a programas de exercícios físicos. Rev Bras Cineantropom Desempenho Hum. 2007; 9(1): 92-100. [ Links ]
18. Moschny A, Platen P, KlaaBen-Mielke R, Trampisch U, Hinrichs T. Barriers to physical activity in older adults in Germany: a cross-sectional study Int J Behav Nutr Phys Act. 2011; 8(121): 1-10. [ Links ]
19. Cassou ACN, Fermino R, Añes CRR, Santos MS, Domingues MR, Reis RS. Barriers to physical activity among Brazilian elderly women from different socioeconomic status: a focus-group study. J Phys Activ Health 2011; 8(1): 126-132. [ Links ]
20. Eiras SB, Silva WHA, Souza DL, Vendruscolo R. Fatores de adesão e manutenção da prática de atividade física por parte de Interviews. Rev Bras Ciênc Esporte. 2010; 31(2): 75-89. [ Links ]
21. Korkiakangas EE, Alahuhta MA, Husman PM, Keina¨nen-Kiukaanniemi S, Taanila AM, Laitinen JH. Motivators and barriers to exercise among adults with a high risk of type 2 diabetes - a qualitative study. Scand J Caring Sci. 2011; 25(1): 62-69. [ Links ]
22. Galea MN, Bray SR, Ginis KA. Barriers and facilitators for walking in individuals with intermittent claudication. J Aging Phys Act. 2008; 16(1): 69-84. [ Links ]
23. Instituto Brasileiro de Geografia e Estatística (IBGE) Síntese de indicadores sociais - Uma análise das condições de vida da população brasileira Rio de Janeiro: IBGE; 2010. [ Links ]
24. De Lepeleire J, Heyrman J. Is everyone with a chronic disease also chronically ill? Arch Public Health. 2003; 61(1): 161-176. [ Links ]
25. Dellaroza MSG, Furuya RK, Cabrera MAS, Matsuo T, TrelhaC, Yamada KN. Caracterização da dor crônica e métodos analgésicos utilizados por Interviews da comunidade. Rev Assoc Med Bras 2008; 54(1): 36-41. [ Links ]
26. Lees FD, Clark PG, Nigg CR, Newman P. Barriers to exercise behavior among older adults: a focusgroup study. J Aging Phys Act. 2005; 13(1): 23-33. [ Links ]
27. Chen Y-M. Perceived barriers to physical activity among older adults residing in long-term care institutions. J Clin Nurs. 2010; 19(3-4): 432-439. [ Links ]
28. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012; 380(9838): 247-257. [ Links ]
29. Nair KS. Aging muscle. Am J Clin Nutr. 2005; 81(5): 953-963. [ Links ]
30. Deslandes A, Moraes H, Ferreira C, Veiga H, Silveira H, Mouta R et al. Exercise and mental health: many reasons to move. Neuropsychobiology. 2009; 59(4): 191-198. [ Links ]
31. Scheef L, Jankowski J, Daamen M, Weyer G, Klingenberg M, Renner J et al. An fMRI study on the acute effects of exercise on pain processing in trained athletes. Pain 2012; 153(8): 1702-1714. [ Links ]
32. Blair SN, Morris JN. Healthy hearts - and the universal benefits of being physically active: physical activity and health. Ann Epidemiol. 2009; 19(4): 253-256. [ Links ]
33. Hamer M, Chida Y. Physical activity and risk of neurodegenerative disease: a systematic review of prospective evidence. Psychol Med. 2009; 39(1): 3-11. [ Links ]
34. Mirmiran P, Noori N, Zavareh MB, Azizi F. Fruit and vegetable consumption and risk factors for cardiovascular disease. Metabolism. 2009; 58(4): 460-468. [ Links ]
35. Boffetta P, Couto E, Wichmann J, Ferrari P, Trichopoulos D, Bueno-de-Mesquita HB et al. Fruit and vegetable intake and overall cancer risk in the European prospective investigation into cancer and Nutrition (EPIC). J Natl Cancer Inst. 2010; 102(8): 529-537. [ Links ]
36. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa de orçamentos familiares 2008- 2009: análise do consumo alimentar pessoal no Brasil. IBGE, Coordenação de Trabalho e Rendimento. Rio de Janeiro: IBGE; 2011. [ Links ]
37. Khajuria DK, Razdan R, Mahapatra DR. Drugs for the management of osteoporosis: a review. Rev. bras. reumatol. 2011; 51(4): 372-382. [ Links ]
38. Grimnes G, Joakimsen R, Figenschau Y, Torjesen PA, Almås B, Jorde R. The effect of high-dose vitamin D on bone mineral density and bone turnover markers in postmenopausal women with low bone mass-a randomized controlled 1-year trial. Osteoporos Int. 2012; 23(1): 201-211. [ Links ]
39. Pérez Samaniego V, Devis Devis J. La promoción de la actividad física relacionada con la salud. La perspectiva de proceso y de resultado. Rev Int Med Cienc Act Fís Deporte. 2003; 3(10): 69-74. [ Links ]
40. Fares D, Barbosa AR, Borgatto AR, Coqueiro RS, Fernandes MH. Fatores associados ao estado nutricional de Interviews de duas regiões do Brasil. Rev Assoc Med Bras. 2012; 58(4): 434-441. [ Links ]
41. King AC, King DK. Physical activity for an aging population. Public Health Rev 2010; 32 (2): 401- 426. [ Links ]
