











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Uruguay is located in South America. It measures 176,215 km 2. According to the latest census, it has 3,286,314 inhabitants, 94.7% of which lives in urban centers. Overall density is 18.6 inhabitants/km2, and the literacy rate is 98.5% 1. Natural population growth is 0.19% and life expectancy is 81.2 years for women and 73.7 years for men 2. The birth rate is 13.4 per 1,000 inhabitants and mortality is 9.5 per 1,000. The human development index is 0.790 3 and the unemployment rate is 8.4 % (4. The gross domestic product is $59,918 million 5, with significant weight on agricultural exports. Administratively, the country is divided into 19 departments.
Description of the problem: A new government took office on March 1 of this year, and the first cases of COVID-19 were detected on March 13.That is when the government began taking certain steps to discourage large numbers of people from gathering in places such as businesses with large spaces, large sporting events, movies, theaters, and cultural events. The government’s March report also mentioned polyclinics, and proceeded to close them. In-person classes were also suspended at all educational levels, including universities.
Another social measure for mitigating the situation was short-term aid for those with formal employment, issued by the State Department of Social Security. These measures were relaxed in order to benefit the largest number of people, thereby encouraging them to stay home.
Several social programs were also expanded, including food programs, while civil society primarily took up organizing the distribution of food baskets and donated cooked food (“ollas populares”), which are more plentiful in places where the population is better organized.
In parallel, the health system began the phase of assessing its available infrastructure and material and human resources across the country.
With regard to health insurance, 1.6% of the population lacks public or private comprehensive coverage 6.
The government quickly contacted a group of renowned scientists to voluntarily serve as consultants.
Since Uruguay is a small country, the issue of scale made it difficult to obtain the tests needed for the diagnostic stage. As a result, the National Research Agency, through public appeals, has financed projects involving researchers from the University of the Republic and the Pasteur Institute 7, in order to contribute to the country’s installed capacity with highly trained and qualified human capital. These actions have notably increased the diagnostic testing capacity without depending on international providers.
In early May, in a matter of days, it was possible to administer over 1,000 tests daily. This was one of the goals that the system determined to be necessary for better understanding community transmission and which interrelated groups of people were being impacted the most.
With regard to health system resources, most of the intensive care resources are in metropolitan areas, where over 60% of the country’s population resides. While north of the Negro River, both human resources and installed capacity are the scarcest, especially in the public sector.
Surveillance System
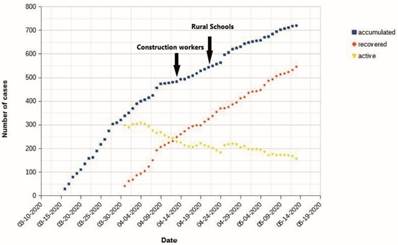
Regarding the temporal distribution of the cases that have been reported by the epidemiological surveillance system, Figure 1 presents the frequency of accumulated, recovered, and active cases between March 13 and May 13. While this represents two months, we can say that recovered cases increased while the curve of active cases did not greatly increase during this period.
As of May 13, there were 719 total accumulated cases, considered an indicator of health since this represented 0.022 % of the population.There have been 19 total deaths to-date, representing 2.6% of known cases of infection.
Of the detected cases of infection, 14% corresponds to health workers, with 1 death. Eighty percent of the reported cases of health workers occurred within one month of detecting the first cases.
A total of 30,209 tests has been performed to-date, representing 9.2 per 1,000 inhabitants.
A comparison with other countries in the region of COVID-19 mortality rates (with the same end date as the Uruguay data, May 13), per 100,000 inhabitants, shows: 6.2 in Brazil, 2.2 in Chile, 0.8 in Argentina, 0.6 in Uruguay, and 0.17 in Paraguay.
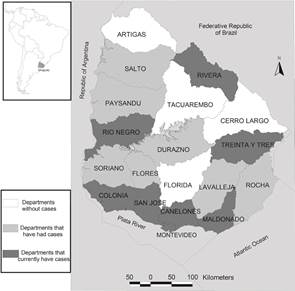
Cases have been reported in 15 of the 19 departments (Figure 2 ).
Lifting of Social Distancing
The first two steps taken to begin lifting social distancing were restarting construction work on April 13 (45,000 workers) and opening rural schools on April 22 (optional attendance), except for the most populated departments with a larger number of cases (Canelones and Montevideo). Currently, few students are attending.
As seen in Figure 1, the curve did not change in spite of these two events, which also resulted in the simultaneous increase in related activities.
Primary Health Care
One month after the first notifications, primary care physicians expressed concern that checkups for people with chronic illnesses were being neglected, and because primary care is the level of care that should be provided to the majority of those infected, but many of those centers were closed.
A new challenge for environmental health
Just as this pandemic presents us with a planetary problem, the authors believe that we are facing this problem due to how environmental conditions are managed, and that this will continue.
The first part of this text described COVID-19 cases during the first two months and the impact on Uruguay, as well as early measures to mitigate the problem. Given the importance of the problem and the strategy that has been used in the country, in this article, the authors want to highlight what they consider to be the true causes of this problem, in order to understand the material bases underlying it. Without this recognition, we will not have elements for acting on the causes, but will only be able to lessen the consequences.
We are witnessing one more manifestation of how anthropocentrism compromises the environmental health of the planet. In reality, we share both a single ecosystem 8 and “one health”.
Many conditions may be contributing to the emergence of a new virus. Those that are usually found are population density and particular practices by those populations. 9 There is also a growing trend in the emergence of RNA viruses 9.
Zoonoses have been increasing due to intensive human land use practices, which along with growing urbanization processes are slowly blurring the interface between humans and domestic and wild animals 10), (11. Host habitats have been recognized as domestic, peridomestic, and sylvatic 11.
Human exposure is less common in sylvatic habitats, but this is changing with environmental degradation and human intrusión 11.
Based on these considerations, the source of this new virus, as well as earlier ones, has progressively been identified as intensified extraction activity, with their significant transformations of wild ecosystems and the global environment 12), (13. Along with these modifications of environmental systems, urbanization models with large concentrations of populations in limited spaces have been increasing and expanding14. These processes produce ongoing re-territorialization of the global population, with different local manifestations 15. In brief: farming populations move to cities, upper and upper-middle classes move to new urban zones on the outskirts of cities, working populations concentrate in highly dense urban population zones, and populations with scarce resources live under precarious urban conditions in areas where the environmental quality is not adequate for human living 16.
These are complex phenomena, and, identifying the determinants of emerging pathogens requires an inter-disciplinary approach -biological, ecological, economic, and social 17.
Cultural elements are relevant to the appearance of zoonoses in peridomestic environments 11. Changes in ecosystems have been found to create conditions for sylvatic species to be introduced into peridomestic environments, facilitating the spread of these diseases. This spread is also related with a lack of socio-economic resources, poor-quality water for consumption, inadequate housing, and particular conditions such as floods 11. It is important to consider all of these factors, since they contribute to effective contact between human populations and fauna species that generally have not interacted, leading to the development of zoonosis 11.
In this way, intermediate hosts appear among humans 18, transmitting the infectious agent, as is known to happen with civets that transmit SARS-CoV to humans 19, while bats are recognized as the source of this spread 19.
The conservation of ecosystem biodiversity is a natural mechanism for preventing effective contact11.
Nevertheless, at the global scale, the discussion has centered more on the effects of the pandemic and wagering on an effective control mechanism, giving no priority to the analysis of the causes of the emergence of new zoonoses and the possibility of reversing those causes. In that regard, reports over recent months suggest that the structure of health systems and the possibility of implementing measures for their functioning seem to be the key to establishing effective measures for controlling the emergence and expansion of the virus among populations in highly dense regions.
Conclusions
Detected cases represent 0.022% of the country’s population, and deaths represent 2.6% of detected cases.
Since it is accepted20 that the number of asymptomatic or paucisymptomatic cases is important, mortality from COVID-19 is compared with other countries in the region, finding Uruguay to be lower than Brazil , Chile and Argentina, with Paraguay having the best indicator.
In Uruguay, health care workers represent 14% of detected cases, while 4.4% was reported in China 21. That report indicates that new cases no longer occurred once the health care workers were advised of the situation and adopted adequate protection measure 21. The same may be happening in Uruguay, since 80% corresponds to the first month in which the first cases were detected.
The multiple dimensions of the problem need to be understood, including the epidemiology, and also ecology and the multiple levels at which interactions between living beings develop, and how they relate with each other 11.
Though much less frequent, there are those who still argue, even today, that a strategy could be to eradicate some species that is carrying the infectious agent. However, illnesses should actually be understood as natural processes. With the elimination strategy, new species could appear along with other pathogens or parasites that fill the empty niches that would be left behind 11.
Public health should take action and facilitate control and management strategies based on the framework of “one health” and with knowledge about ecology and epidemiology 11.
Increase mobility of human populations, accelerated and unorganized settlements across the world, overexploitation of natural resources, and decreased wildlife areas are factors that are going to continue to contribute to the emergence of diverse diseases 11. This requires collaborative, interdisciplinary, and interinstitutional action. Furthermore, a perspective that enables recognizing this as an environmental health problem, related with global environmental change, would discourage point solutions created in each region by whomever governs them. Preventing new epidemics with these characteristics requires working on broad-based strategies that support environmental stewardship, with the understanding that the key is knowing that what is to be preserved is “one health.”
If we fail to go beyond symptoms and do not act on the causes, this will become another one of the situations to which we will have to become accustomed.

