











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
Muscular performance (MP) refers to the muscle's capability to produce maximal force, to produce force quickly and to produce submaximal force throughout the entire range of motion (muscular work); these three major characteristics of muscle contractility are all necessary for activities of daily living1. Maximal voluntary force (isometric peak torque) has been, and it still is the most valid and reliable muscular performance variable studied in response to exercise, muscle damage and recovery1-4. To our knowledge, time to maximal force and muscular work in response to muscle damage induced by lengthening contractions (LC) have not been reported yet, despite its functional significance in documenting the progress of muscular recovery.
It is well documented that the clinical symptoms of delayed onset muscle soreness (DOMS), defined as the mildest type of muscle injury due to exercise -stiffness, soreness, tenderness and swelling- are accompanied by a reduction of the muscle's capacity to produce maximal voluntary force and the inability to carry out certain functional movements such as walking, up and down stairs or sportive performances2,5-9. This could be attributed to the inflammatory response, metabolic fatigue, excitation-contraction coupling failure and to the disruption of structural proteins in muscle fibers9,10. However, the study of the functional impact of DOMS has been limited to the description of the decline and recovery of peak torque in an isometric and isokinetic contractions; thus, the DOMS impact in muscular work and time to peak torque has not been examined yet.
Therefore, the purpose of this study was to describe the changes induced by a session of LC on isometric and isokinetic peak torque, muscular work, time to peak torque and DOMS under two conditions (Maximal Dynamic Contraction (MDC) and from standing to sitting position) in healthy and physical active young men.
Methods
Design
A quasi-experimental study was conducted, where the comparisons were performed among measurements within each individual. After the written inform consent was given, four visits to the laboratory were made by participants, before the exercise session (TO), 48h (T1) and 96h (T2) post-exercise. During the first visit to the laboratory, demographic information as well as anthropometric measurements (height, body mass and body mass index -BMI) were acquired. For determined creatine kinase activity (CK) a resting blood sample was picked up, and the baseline measurements of MP and DOMS were completed (TO). Between 24h to 48h after the first lab visit, the participants performed the unilateral (dominant lower extremity, assessed by kicking a ball) lengthening contractions exercise session. Blood sample was collected, and measurements of MP and DOMS were conducted at T1 and T2, following the same procedures as in TO. Thus, the dependent variables regarding MP were isometric and isokinetic peak torque (Nm), time to peak torque (s), and work (J) of knee extensor, and intensity of DOMS (mm). The independent variable was the measurement moment (TO; T1; T2).
Participants
Twenty healthy men (18-25 years of age), physically active, classified in category 2 (moderate) by the International Physical Activity Questionnaire (IPAQ) in the short form, were recruited to voluntarily participate in this study11. To be eligible to participate, the individuals must have had a BMI within normal range (18.5 and 24.9 kg/m2) and had achieved a total physical activity between 600-1500 MET-min/weeks. The physical activity level was determined using the IPAQ scoring system11. Subjects were excluded if they had circulatory or metabolic diseases, acute trauma in any of their lower limbs, local or systemic infection, engaged in regular muscle strengthening or endurance training of the lower limbs >6 month12. Any therapies known to attenuate the inflammatory response were not advised (non-steroidal anti-inflammatory medications, statins, heat or ice therapy).
All volunteers were informed of the procedures and potential risks associated with their participation in the study and gave their written informed consent. This study was approved by the local Institutional Review Board for Human Research o and conforms to the international standards concerning the use of human subjects as exercise science research participants13.
Measurements
Participants were positioned on the isokinetic dynamometer to setup the seat settings throughout testing and LC exercise (Humac Norm isokinetic dynamometer, CSMI, Boston, Massachusetts, USA). To isolate the knee extensor, movement at the shoulders, hips, thigh, and ankle were restrained with straps provided by the manufacture. The participants were instructed to keep their arms crossed on their chest during the protocols.
MP measurements were determined during a maximal isometric contraction, defined as isometric peak torque (IPT) and time to peak torque (TPT); and during a maximal isokinetic concentric contraction, were isokinetic peak torque (KPT), muscular work (MW) and TPT14. DOMS was assessed with visual analog scale (VAS) under two conditions.
Muscular performance assessment protocols
The muscular performance assessment protocols used in this study was previously published by Warren et al. (4 and Alemany, et al. (5. Each participant performed two testing protocols, isometric and isokinetic contractions. The isometric contractions protocol, performed at 60° of knee flexion, with 0° representing full extension on the dynamometer, consisted of 5 maximal voluntary contractions, each maintained during 5s, with a minute rest between trials. IPT and TPT was reported as the average of the of the last 3 contractions5. For the isokinetic testing protocol, the lever arm of the dynamometer was programmed to extend the participants knee from a start position of 120° of flexion to full extension, at a velocity of 60°/s. 5 maximal concentric contractions were performed with a minute rest between trials; the variables KPT, TPT and MW were reported from the repetition at which the highest torque was elicited. Subjects were encouraged to achieve a maximal contraction during all the attempts. Before data collection, a pilot was conducted to determine intra-rater reliability of the MP variables (n=10); each participant was assessed twice on 2 separate days with 8d lapse between the measurements. Based on previous studies interpretation of the Intraclass Correlation Coefficient (ICC) (15,16, isometric variables achieved an ICC from moderate to good (IPT=0.8; TPT=0.7); isokinetic variables achieved an ICC from moderate to excellent (KPT=0.6; MW=0.6; TPT= 0.8).
Intensity of perceived delayed onset muscle soreness
Intensity of their overall quadriceps muscular soreness was measured using VAS4 ; this scale has been established as a appropriate method for assessing DOMS, being sensitive to changes on pain perception16. The VAS software program developed by the Neurobehavioral Research Laboratory and Clinic (NRLC) was used to collect pain intensity score17.
Immediately after the MP protocols subjects were instructed to click on a 100mm line at the point that were best represented their overall quadriceps muscular soreness perceived during the MDC. The pain intensity during a functional activity was assessed from standing to sitting position. Subjects were instructed to descend slowly following the beats of a metronome calibrated at 30 bits/min with the upper limbs crossed over the chest, to achieved the final position sitting on the chair with their knees at -90°. Immediately after, the subjects marked the intensity of DOMS. The minimum clinically significant change in pain is considered to be 13mm17,18,19.
Session of Lengthening Contraction
The session of LC for knee extensor used in this study was previously published by Delgado-Díaz, et al. (20, where the speed and mode of contraction were selected based on previous studies demonstrating the effectiveness of this protocol to generate an acute inflammatory response5,7.
Following a general warm-up, participants were positioned in the dynamometer, following the setup determined at T0. For the LC, the lever arm of the dynamometer was programmed to extend the leg to 30° of knee flexion (where 0° is full extension) to 120° of flexion, thus allowing 90° of excursion.
Participants were then asked to contract their quadriceps against the level arm resistance; they did not contract during the concentric phase of the movement. During the active phase, investigators provided verbal encouragement for the participants to complete and exert maximal force during each contraction. The exercise session consisted of 20 sets of 10 reps with 1 min rest between sets. Thus, participants performed a total of 200 unilateral muscle-lengthening contractions of the quadriceps femoris at 120°/s.
Blood analysis
Blood samples ( 10 mL) were drawn from the anticubital vein region of the arm, following standard protocols. Blood samples were drawn at T0, T1 and T2, before any procedure. Immediately after collection, samples were centrifuged for 15min to separate the plasma into aliquots and CK activity was analysed using CK-NAC-liquiUV reagent (HUMAN Gesellschaft fur Biochemica und Diagnostica, Germany). Each sample was analyzed in triplicate as standard procedure7.
Statistical Analysis
Descriptive, parametric, and non-parametric statistical analyses were performed with StataCorp2013. Stata Statistical Software: Release 13. Appropriate statistical assumptions (normality and homoscedasticity) were tested before hypothesis testing for each variable; CK activity level and DOMS during the functional activity had no normal distribution, DOMS was transformed to its Log to be included in the statistical models. Descriptive statistics were used to summarize population characteristics and dependent variables data.
A null hypothesis rejection was set at p<0.05 for all measurements, continuous data are presented as mean±standard error (SE), whereas ordinal data (physical activity and CK activity level) are presented as median±inter-quartile range (IQR). Comparisons among time points were performed by a simple regression analysis20,21, using T0 measurements as reference to determinate the effect of the session of LC in MP and intensity of DOMS; coefficient(P), 95 % confidence interval(CI) and p-value are reported. Based on the simple regression results, an additional multiple linear regression with standard least-squares procedures was used to study the relationship between MP variables and the change of DOMS intensity after exercise, adjusted by TO measurements. The change of DOMS during a maximal dynamic contraction (T1-TO) was included in the regression model. The adjusted coefficient of determination R2, corresponding to the percentage of variation explained by a best-fit regression line was used to measure how the variation of the change in DOMS intensity explains the variation of each muscular performance variable.
Results
All subjects finished the study with no complications; mean age of 21±0.34 years, activity level of 988.4±73.21 MET-min/wk, BMI of 23.24±0.29 Kg/ m2. Muscle damage was verified in all participants by a significant growth in CK activity levels post-exercise from 173.5±152.5 IU/L at TO, to 361±204 IU/L at T1 (p=0.003) and to 362.5±1194 IU/L at T2 (p=0.002). Descriptive data of the dependent variables at each time point are presented in Table 1; simple and multiple regression analyses are summarized in Table 2and3, respectively.
Table 1 Description of muscular performance variables and intensity of delayed onset muscle soreness at each time point.
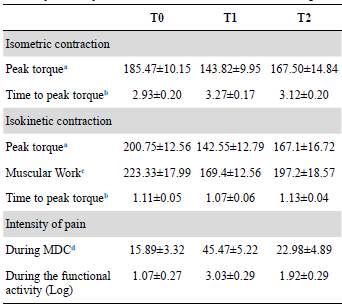
All variables, are reported as mean ± standard error of the mean;
MDC: maximal dynamic contractions.
a Peak torque in Nm.
b Time to peak in seconds.
c Muscular work in Joules.
d Intensity of pain in millimeters.
Table 2 Effects of the session of lengthening contractions on muscle performance and intensity of delayed onset muscle soreness variables (analysis of covariance, using baseline (T0) results as reference).
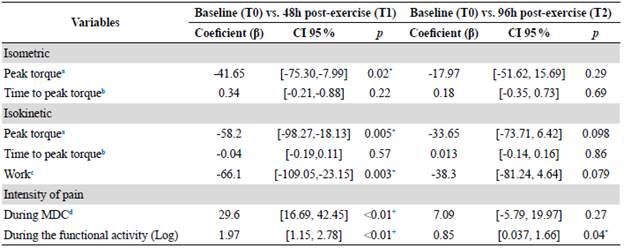
All variables are reported as mean ± standard error of the mean; MDC: maximal dynamic contractions
*p<0.05; +p<0.01
a Peak torque in Nm.
b Time to peak in seconds.
c Muscular work in Joules.
d Intensity of pain in millimeters.
Table 3 Multiple regression analysis using the change in the intensity of delayed onset muscle soreness on muscular performance at 48h post-exercise (dependent variable), adjusted by baseline measurements (T0).

Dependent variable: A DOMS intensity; represents the subtraction of the intensity of delayed onset muscle soreness at T1-T0.
*p<0.05; p<0.01.
a Peak torque in Nm.
b Muscular work in Joules.
Discussion
The main and novel findings of the present study were that lengthening contractions significantly decreases muscular work and peak torque, and induces muscle soreness, which explains 29 % of the decrease in isometric peak torque. To the best of the authors' knowledge, this is the first study to assess the muscle soreness intensity during a functional activity, and its implications in the force production drop after a single session of lengthening contractions.
In our study, all 20 subjects were moderately active and successfully completed the experiment. As expected, a significant increase in CK activity level was detected 48h post-exercise, which did not return to baseline values by the end of the experiment (96h); this data agrees with previous publications that have shown a significant increase in CK levels above 300IU/L in response to unaccustomed lengthening exercise(57), which remains elevated up to 14 days2,18,22. Inter-individuals variability23 in the CK response should also be considered, with one study demonstrating a wide variation for CK activity range (200-2500 IU/L) (6, also seen in the current study.
In response to a single session of LC, isometric peak torque significantly decreased in approx. 23 % 48h postexercise and returned to baseline 96h after the exercise. This drop in force output has been attributed to the fact that exercise at longer initial muscle lengths creates a larger amount of strain on muscle fibers, therefore it induces damage of the muscle microstructure and reduces its capability to generate tension2. Using similar exercise protocols, previous studies report a decrease in isometric peak torque of 20-30 %24.
Similar change was detected in KPT (60%) and MW (-30 % decrease in force and total work). To our knowledge, a unique study has examined the isokinetic muscular performance after an unaccustomed exercise24. Their results show a smaller magnitude (8 %), yet significant, force drop at 48h post-exercise compared to our data. The difference in the change magnitude is likely due to issues related with parameters of the protocol used in studies (range of motion and velocity for testing procedures, and number of muscle contractions of the exercise protocol).
In the present study no differences between baseline, 48h and 96h post-exercise were detected in time to isometric and isokinetic peak torque. Attempts to normalize this variable by peak torque did not provide additional information. To our knowledge, only the study of Molina, et al. (24 has reported changes in time to isokinetic peak torque after muscle damage, whose findings show a decrease of 23 % at 48h post-exercise. Nevertheless, the comparison between our data and this study must be made with caution due to the differences in the characteristics of the exercise protocol. The TPT informs the capacity of the neuromuscular system to recruit the muscle cells, however, should be interpreted as an indirect measurement of power4. For this reason, in future studies it is necessary to include a true describer of muscular power due to the importance of it in the muscle function, mainly within the concept of balance25.
It is well established that unaccustomed muscle lengthening exercise produces damage to muscle tissue. Indirect evidence of damage includes the DOMS that appears 24h after exercise and peaks at 2-3d and subsides at around 8-10d after exercise; these timeline responses in DOMS has also been attributed to the exercise protocol, regarding the type of muscle contractions and velocity1-4. Molina, et al. (24 study shows a significant increase in DOMS of approximately 40mm at 48h after exercise, when compared to baseline, similar data has been previously reported by other authors1-4. Same magnitude of soreness intensity is reported in the current study. Despite the fact that muscle soreness is a well-known and commonly experienced phenomenon, the exact mechanism to explain how it develops and why it is a delay sign is not fully understood yet.
A number of theories have been proposed to explain the pain stimulus associated with DOMS, for instance lactic acid accumulation, muscle spasm, connective tissue damage, ultrastructural muscle damage, inflammation, enzyme efflux1-4,8,22,26. The general consensus amongst researchers is that a single theory cannot explain the onset of DOMS. As a result, the model proposed for Cheung, et al. (26, integrates aspects from other theories, which makes it easier to understand all the possible events that happen in this physiological process. The model works under the assumption that high tensile forces associated with lengthening exercise cause muscle and connective tissue damage in their structure. These events result in the accumulation of calcium and the activation of proteolytic enzymes that degrade the z-line of sarcomeres. It is proposed that in a few hours after, there is a significant elevation in circulating neutrophils and mast cells, starting with histamine and prostaglandin production that sensitizes type III and IV nerve endings to mechanical, chemical or thermal stimulation1-4,8,22,26.
It has been implied that DOMS may result in alterations in muscle performance, mainly in it capacity to produce maximal voluntary force (isometric peak torque) (1-4,8,24,26; our data supports this hypothesis, providing evidence that DOMS intensity explains 29 % of the reduction in force. In addition this results evidence that during the execution of functional activities that involve an eccentric control of the quadriceps as used in this study; DOMS intensity at 48h was significance difference (p<0.01) and can affect the perform of activities of daily living.
The results of this study are delimited to the effects on physical active young men, with no significant fluctuations in hormonal changes that could affect the muscle response to exercise. In conclusion, evidence from the current study suggests that DOMS intensity explain in a significance percentage (-30 %) the decrease in muscle performance, mainly in maximal force. Taking into account the impact of the DOMS intensity in muscle performance should be done when prescribing physical rehabilitation. For this reason, DOMS should be alleviated during the first 48h postexercise through physical and therapeutic exercise modalities with the purpose to avoid a significance decrease in maximal force, accelerate the recovery and limiting the functional impact.
Further studies should investigate the effect of DOMS intensity on the recruitment pattern and the muscular power to have a more comprehensive impact on the muscular performance in order to improve the exercise prescription during the rehabilitation programs.

