











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink
Introduction
Zika infection arrived in Colombia in October 2015 and quickly became an epidemic in most of the country1-4. Due to its association with microcephaly2 and other adverse effects in children and pregnant women, including "Zika syndrome"3, alarm was widely sounded and the Ministry of Health and Social Protection even recommended pregnancy avoidance until the epidemic was over5,6. This could have been useful in areas with adequate sexual and reproductive health services. In the case of Colombia, several studies indicate that access to these services is low and their quality is poor, especially for indigenous and Afro-descendant populations6,7. An increase in the use of hormonal contraceptives in Colombia has not been noted8, and many known obstacles and delays in accessing to abortion services, although they are legal in Colombia when the life is not viable due to foetal malformations9. In addition, sexual and reproductive health services are more available in health centres in higher socioeconomic regions10. Problems related to the adequacy and content of prenatal care compared to quality standards persist in the country, especially among vulnerable populations, exarcerbating inequities in access and quality of sexual and reproductive health care for women. A national study in endemic and non-endemic vector-borne regions shows that between 23.4% and 37.4% of pregnant women received comprehensive care, with unequal quality of care among pregnant women who received health insurance through subsidies11.
In endemic vector-borne regions, it was found that in 13 municipalities of the region, 36% of pregnant women reached the number of controls scheduled according to the norm, and this percentage decreased in the third trimester of pregnancy. In addition, only 53.2% received adequate prenatal care, and the administrative procedures required by the facilities were the main barriers for not attending prenatal care. Some studies analyzed adherence to prenatal care in seven low-complexity hospital using clinical records. Poor compliance was found in obstetric risk classification, laboratory tests, detection of alarm signs, remission and counter-remission of pregnant women12,13.
In this context, the Zika epidemic was a "natural experiment" that allowed observing the performance of health services in times of social crisis and scientific uncertainty. The aim of this study was to evaluate prenatal care during the outbreak of Zika virus infection in endemic and non-endemic vector-borne regions in Colombia.
Methods
A descriptive study was conducted, supplemented by interviews (mixed study) (14. The rationale for including the qualitative component was to explore some more intimate details of the experiences of women from endemic regions with vector-borne diseases while receiving health care. First, the pregnancies and prenatal care of women who lived in a vector-borne disease-endemic area (Cesar department), where cases of Zika infection occurred, were compared with those who lived in a region whose characteristics did not contribute to the spread of infection (Boyacá department). The fieldwork was conducted in 2016.
Women who were pregnant or whose pregnancy ended in the three months preceding the fieldwork and who received attention in the health institutions involved in the study were invited to participate in the study. The lists of possible participants were obtained from hospital registries in both regions. A total of 84 pregnant women participated, 40 of whom were from Aguachica, Río de Oro, La Gloria, and Gamarra in the department of Cesar. These women were selected through the local health system and had contracted Zika during the epidemic. These women were cited to the local hospital to know their actual condition during that time, to ask them about their knowledge of Zika, and to inform them about the study. The women who consent to the study, signed the consent at that moment. This region has always been a dengue-endemic area15. It is located between 50-200 metres above sea level (MASL) and the average temperature is 28-36°C. Aguachica, with 93,917 inhabitants, of which 84.7% live in urban areas, had a maternal mortality rate of 46.95/100,000 live births and a neonatal mortality rate of 6.57/1,000 live births in 2014. The percentage of live births whose mothers received four or more prenatal checkups was 92.32% in 201316.
The remaining 44 women were from a control region (the municipalities of Mongui and Topaga in the department of Boyaca), located at approximately 2,900 MASL, where the temperature ranges from 8 to 16°C. Monguí has a population of 4,982, 43% of whom live in rural areas. There were no cases of maternal mortality during the period 2005-2017. In 2017 neonatal mortality was zero, and the percentage of live births whose mothers received four or more prenatal examinations was 97.67%17. Both groups of women received prenatal health services at least once from their municipalities, where they were contacted for their participation in this study. The women control (Monguí) were selected for convenience according to the number cases. Information collected included sociodemographic data such as socioeconomic status (one, two, three, four, five, or six strata, with one being the lowest), social security affiliation (subsidized, contributory, or SISBEN), and marital status (single, married, open partnership or separated), as well as variables related to reproductive health such as previous pregnancies, and variables related to prenatal care during the previous pregnancy, including reasons and difficulties related to becoming pregnant, months of pregnancy at the start of prenatal care examinations, number of prenatal care visits, and activities performed by the physician. Information was also collected on diagnostic images ordered and performed, information provided by health institutions and insurers about Zika and its prevention, pregnancy outcomes, and complications at delivery and postpartum. The focus was on the changes in prenatal care that health care workers had made as a result of the infection.
To evaluate prenatal health care, indicators based on the model by Morestin et al. (18 were developed to assess the quality of obstetric care, incorporating the dimensions for evaluating the quality of care of Donabedian: structure, process and outcome. Morestin et al. inventoried the components of quality of obstetric care from the literature. They organized them into these three categories, creating a comprehensive conceptual framework in which every item is a potential criterion for evaluating obstetric care quality. These categories follow a logical sequence: available resources (e.g., obstetric care protocols) put into action lead to activities (physician-patient relationship and episode of care) that lead to outcomes (the consequences of services for patients) (18.
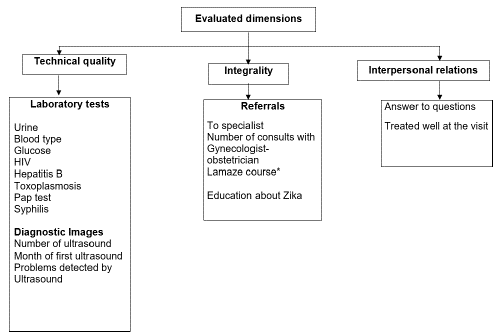
This study assessed the interaction process, which includes the technical quality of the program and interpersonal relationships. The scope of the program was assessed based on the process of care (Figure 1). Mode of delivery classified maternal outcome, and fetal outcome was measured by fetal complications noted, including those caused by Zika. To determine the maternal health of both populations, maternal complications were also compared between groups, regardless of their association with Zika.
*The goal of Lamaze is to build a mother's confidence in her ability to give birth.
The indicators were based on the same variables. The only difference was the comprehensiveness indicator for the Zika education program, which was evaluated only for the women from Cesar. However, to evaluate the fulfilment of each indicator, the women from Cesar were considered pregnancies at high obstetric risk due to Zika infection, regardless of the presence of any other risk condition, and the women from Boyacá were defined as a pregnancy group not exposed to Zika. The content of prenatal care was evaluated in terms of compliance with Colombian Resolution 412, which in 2000 established guidelines for prenatal care according to the classification of pregnancy risk. All the procedures mentioned in this resolution are covered by the benefit plans provided by Colombia's subsidiary and contributory health systems.
Depending on the distribution observed, the variables were described with percentages or measures of central tendency and dispersion. Chi-square, Fisher's exact, Student's t, and Mann-Whitney U tests were used to compare the characteristics of pregnant women from the vector-borne diseases-endemic region with those from the nonendemic region. As part of the supplemental qualitative component of the study, eight women from the endemic area with a Zika diagnosis were included. Interviews were conducted in the regional hospital in Aguachica, Colombia, where they received care during their pregnancy.
A phenomenological approach was used, that allowed everyday life experiences to be described from the perspective of actors19,20. In this case, the aim was to delve into topics that might be sensitive for pregnant women. Five participants were under three months of gestation, two of them had their newborns diagnosed with microcephaly, and one participant's baby died at birth. This woman was diagnosed with Zika infection in her fifth month of pregnancy, and problems with the baby were detected during ultrasound in her sixth month of pregnancy. The ages of the participants ranged from 19 to 33 years. Of the eight women, two were in their first pregnancy, five in their second pregnancy, and one was pregnant for the fourth time. The majority were diagnosed with Zika infection in the fifth month of pregnancy.
Interviews lasted approximately 45-60 minutes and were conducted by a psychologist to appropriately address content that might be sensitive to participants. Topics covered in the interviews were knowledge and perceptions of Zika during pregnancy and expectations about how information should be handled. Interviews were audio recorded, with the consent of the participants, and later transcribed. Matrices were used for the information analysis, given the number of interviews. Two categories were established a priori: knowledge about Zika and quality of care, which aimed to further explore the findings obtained with some elements of the quantitative component of the study. Because the present study reached saturation of the contents studied with eight women, there was no need to increase the sample size in accordance with the concept of theoretical saturation21-23. This study was approved by the Ethics Committee of the Fundación Cardiovascular de Colombia. All women in this study provided written informed consent.
Results
The Table 1 shows the characteristics of the pregnant women in the study. The socioeconomic level was low for most women (Cesar 82.50%, Boyacá 64.29%). A predominance of participants from Cesar (50%) was enrolled in the contributory health care system, and the majority from Boyacá (75%) were enrolled in the subsidized health system (p<0.008). The majority of both groups reported their marital status as a free partnership, followed by married, and then single. More women in Cesar (67.50%) had prior pregnancies than in Boyacá (56.82%), with more prenatal examinations there, although the difference was not statistically significant. The average number of visits to prenatal care during the previous pregnancy was 7 for both groups. The women in Cesar (22.50%) and Boyacá (27.27%) reported using some type of contraceptive when they become pregnant. Women from Cesar knew more about the Zika epidemic than the women from Boyacá (p<0.06). Some of the women in Cesar (45%) and Boyacá (20.45%) had already started prenatal care visits before the Zika epidemic was declared (p<0.020). In both municipalities, they started attending prenatal care visits when they learned they were pregnant. However, it is worth noting that 47.73% of the population of Boyacá began prenatal care visits months after learning they were pregnant. Difficulty starting prenatal exams was experienced by 13.89% of the women in Cesar and 18.18% of women in Boyacá (p<0.762).
Table 1 Characteristics of pregnant women participating in the study according to Zika infection region in Colombia in 2016 (n=84).
*Fisher’s exact; † Mann-Whitney U Test.
yWomen who, according to the Identification System of Beneficiaries of SISBEN-State subsidies, meet the requirements to receive health insurance, although they have not yet enrolled.
Table 2 shows the results of the indicators of technical quality of prenatal care. In Boyacá, a better fulfilment of the technical quality and scope of the program was observed compared to Cesar. Regarding the technical quality of the program, laboratory tests showed better fulfilment of blood type analyses (p=0.003) and vaginal smears (p=0.077) in Boyacá, lower fulfilment of syphilis tests in both groups, and better fulfilment of paraclinical tests in Boyacá. The first ultrasound was performed in the third month of pregnancy, on average, and more problems were detected by ultrasound in Cesar. The women in Cesar had an average of three ultrasounds, and the women in Boyacá had two. It is worth noting that the number of ultrasounds and the level of complexity varied according to the risk classification assigned to each woman at their prenatal exams.
Table 2 Some indicators of the technical quality of prenatal care reported by pregnant women in endemic (Aguachica) not endemic (Mongui) in Colombia in 2016 (n= 84).
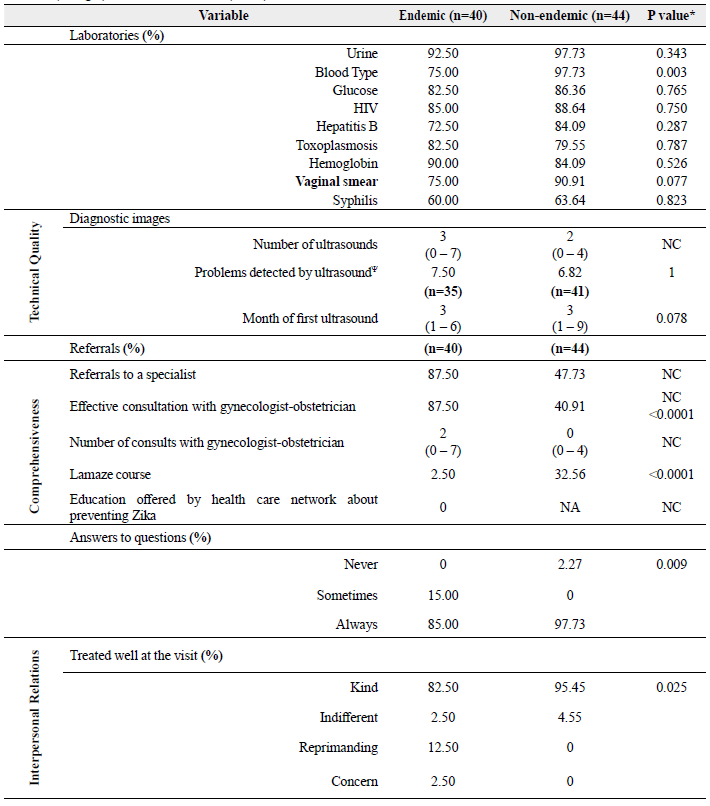
NC: Not comparable; Aguachica is high risk.
ΨThird-level (specialized) ultrasounds for an adequate diagnosis of fetal anomalies were not performed in Aguachica.
Regarding the indicators of the program's comprehensiveness, more women attended the unique course in Boyacá (p<0.0001). In Cesar, more women were referred to gynaecology and consulted by gynaecologists. However, these results are not comparable to those of the women in Boyacá, since the protocol for pregnant women established in 2000 (Colombian Resolution 412) varies according to the risk classification. The women in Cesar had no education about Zika. The interpersonal relationship indicator showed adequate responses to those questions for both groups (p=0.009), and the relationship was mostly good (p=0.025).
About the maternal outcome indicator, vaginal birth was most common in Boyacá, and caesarean section was most common in Cesar among patients who had already given birth at the time of the interview. Miscarriages were found only in Cesar. The women in Cesar had more complications associated to pregnancy, although the difference was not statistically significant (p=0.11). Regarding the fetal outcome indicator, no fetal anomalies were found in Boyacá, while complications (20%) in fetus health were registered in Cesar, including those Zika-associated.
As suspected a priori, there were differences between regions, but not always significant (p<0.05). Therefore, research on pregnancies in the endemic region was explored with qualitative methods. Results on knowledge about Zika infection and associated quality of care are presented below. Knowledge about Zika. For most informants, the media was essential for learning about Zika, particularly television news programs. At the same time, they perceived the information provided by physicians and health professionals to be limited or contradictory (Table 3).
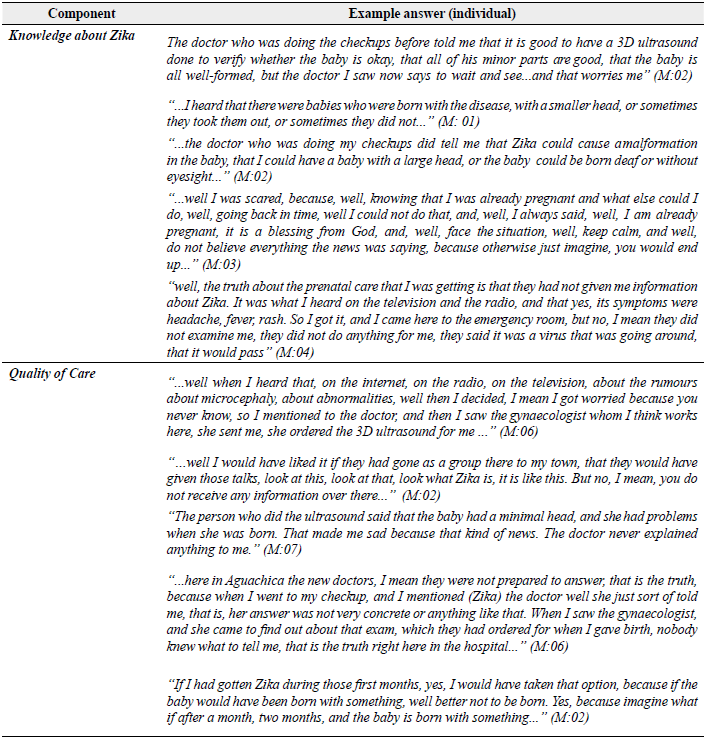
For most women, what they had learned about Zika came from women in the community who shared their knowledge. It was summed up as a disease caused by a mosquito bite, similar to Chikungunya, and its effects on the baby include some malformations such as microcephaly. In some cases, it led to the interruption of pregnancy. Those who received information from physicians indicated that they were informed about some of the adverse effects on the baby. However, the information varied, including malformations of the head, some of which were not accurately identified as microcephaly, which was understood by some to mean "small head," "large head," or "head larger than the body," developmental problems, and visual and auditory effects. The most serious complication that most informants heard about was the presence of microcephaly with a poor prognosis of survival. However, this depended on the medical care provided and the home care.
The information received through informal sources caused anxiety and fear when the disease was diagnosed. As the pregnancy progressed the women's feelings were minimized by some of the physicians who treated them. Phrases such as "it's nothing" "everything is going fine," "do not listen to what they tell you," "everything is normal, I am the doctor and I am telling you that it is normal" conflicted with what they heard around them, such as "doesn't it scare you? Look at the children who have been born like this...," "No, look at what the child gets out of it," and "children are being born deformed," among others. Some also acknowledged that the communication media may have exaggerated the situation, causing panic among pregnant women. Some of the recommendations heard on television were not to get pregnant, to wear clothes that protect against mosquito bites and to use mosquito nets in bedrooms and to use mosquito repellent. They also felt reassured knowing that Zika infection only had an effect when the women were in the first trimester of pregnancy. Moreover, they mentioned that thanks to information from the communications media, they sought medical attention when having fever, chills, headache, and pain in the bones and body in general. However, they were not always told that it was a Zika infection. They were treated with acetaminophen and sent home (Table 3).
Quality of care
The participants considered healthcare providers' interventions to be minimal, and they received very little support or feedback regarding their concerns. In this context, they mentioned having to ask physicians for certain additional examinations (mainly 3D ultrasounds) that they had heard from other women or the media that were important, because physicians did not automatically order those exams. In some cases, doctors did not consider those exams to be necessary; therefore, some of the concerned women chose to pay for the exams themselves. Moreover, while some insurers did approve 3D ultrasounds, the women had to go to another city, which was considered expensive or risky since it required highway travel. Nevertheless, the women who could obtain more examinations reported feeling calmer and less anxious regarding their pregnancy (Table 3).
In general, the women perceived the health services as not having enough knowledge about the disease and not well organized when the Zika outbreak occurred. They would have expected more help and guidance on the issue from experts such as doctors, paediatricians, or someone in charge of health services. Ideally, they would have gone to where the women reside, considering that the majority live in areas far away from the health institutions where they need treatment. During those visits, they would have liked them to explain the disease in detail, the adverse effects on their babies, the recommendations and the alternatives that exist in their situation.
In the case of women whose babies had already been born at the time of the interview and had some sequelae, they reported they had not received enough information about the disease and future complications. It is worth mentioning that the women who had complications during their pregnancy and were referred to Bucaramanga perceived the health care to be better than women who received care in or near Aguachica, Cesar. They highlighted the knowledge of the professionals, being able to access exams, and better hospital infrastructure.
Regarding one of the alternatives when faced with an adverse diagnosis, the possibility of terminating the pregnancy, nobody reported having received information related to this or exploring this possibility with the doctor who treated them. Some women mentioned having thought about interrupting their pregnancy, but were satisfied they did not because regardless of how their babies would have been born, it was not correct; it contradicted their principles. If their doctor had suggested it, they would not have accepted; however, other women would have considered this option given the difficulties with which their babies could have been born.
The women compensated for the lack of guidance and support from the health services by establishing networks with other pregnant women. Through these networks, they built supportive bonds by sharing their everyday experiences and how to manage the pregnancy. They also exchanged information regarding what was new about managing the pregnancy and the presence of Zika, which contributed to wellbeing.
Discussion
The Zika virus resulted in worldwide alarm because of the impact of fetal transmission and its consequences, particularly microcephaly. This led to optimizing prenatal exams to detect cases and possible adverse fetal outcomes, and to adopt preventive measures to decrease the risk of infection during pregnancy. The findings show that no education regarding Zika was received from health institutions, at least in the endemic region. The quality of the care prenatal was better that at endemic region. It is possible that the quality is not related to the type of health security, but rather due to inadequate information in regions of high risk of zika. This could have contributed to an increased vulnerability of pregnant women and suggests deficiencies in the health care network's response to this epidemic. Moreover, this lack of education is relevant given the sexual transmission of the disease, which makes the epidemiological behaviour of this arbovirus different24.
While there were a similar number of medical visits in both regions, fulfilment of prenatal care recommendations were greater in the non-endemic area. This may have been influenced by the place of residence (rural or urban), affiliation status with the health system, and desired pregnancy, among other factors25. Regarding the technical quality of the prenatal exams, this was better in the non-endemic region, which clearly contradicts the access and coverage recommendations for prenatal and sexual and reproductive health services that were issued during the epidemic, among others26. It is probably that other factors as level educations, can have an additional risk in the care prenatal.
While laboratory tests during pregnancy were similar in the two regions, the limited search for infections during pregnancy is noteworthy and demonstrates an essential opportunity for improvement in both regions. Monitoring of syphilis was similar to what has been described in various world regions27. In addition, during the Zika epidemic, reports of the occurrence of toxoplasmosis remained the same, which is a differential diagnosis for this new congenital infection28. Equally important is the lack of blood tests for cytomegalovirus, which is very important to the differential diagnosis of congenital Zika; therefore, a policy should be implemented to perform this in endemic regions29.
The experience of women who received prenatal healthcare in the endemic region during the epidemic was characterized by misinformation and imprecise information, most of which came from various sources unrelated to the health sector. Likewise, support and follow-up were significantly deficient. Therefore, the communications media played an essential role in the information that the women obtained about Zika and its possible effects on their children, particularly television news programs.
These findings demonstrate that health teams lacked knowledge about how to handle the information, which generated confusion and fear among the women and uncertainty regarding adverse effects on their babies. This indicates a lack of interdisciplinary management during the epidemic, which has been shown to improve the quality of life of women30. The anxiety experienced by women was primarily associated with the fear of having children with microcephaly. Therefore, it would have been desirable for pregnant women in endemic regions to have psychosocial support31.
Studies of how health services responded to the Zika crisis have shown that deficiencies in diagnostics, follow-up of pregnant women infected with the disease, and the implementation of information and communications strategies did not help to mitigate the impact of the crisis or decrease health risks for the population in general32. Nevertheless, this study was able to delve deeper into these problems thanks to having a comparison group and complementing quantitative findings with semi-structured interviews.
The problems with prenatal care reported in this study are consistent with much broader analyses of the Zika crisis, which have indicated that weak health systems have not met the challenges that the Zika virus has placed on them. The response by various systems to the crisis has shown how organizing the health care network, training human resources, education, communications, and the epidemiological surveillance system all play a crucial role in confronting and mitigating crises33.
This study has different limitations. The number of participants is small and is not representative of Colombia or departments included in the study; it only reflects the care received by the women participating in the study. Additionally, only volunteers participated in the study, selected by convenience sampling from a list of patients seen by hospital obstetric services. However, the comparison of regions did allow observing differences in care that may be manifestations of different health service providers.
This corresponds more to the focus of the study that sought to deepen, the quality of care provided during the Zika epidemic. With the interviews, the detection of deficiencies in healthcare services that are not possible to identify with only quantitative approximations was possible. Although Zika epidemics occurred in the Americas between 2015 and 2017, Zika is still an endemic, and even new epidemics can be seen shortly34-36. Other possible limitations was interview women (qualitative report) in endemic regions.
Conclusions
In conclusion, while the obstetric risk from exposure to the Zika epidemic was higher for pregnant women in the endemic region, our findings indicate deficiencies in the technical quality of prenatal care. These likely were not attributed to the Zika crisis itself, but rather, it may be systematic given that half of the pregnant women had already started prenatal care when the epidemic was declared. Therefore, the Zika crisis revealed the weaknesses reported in terms of access to laboratory tests, information, and clinical and epidemiological follow-up. This work demonstrates not only low fulfilment of laboratory tests covered by social security, but also the demands that pregnant women place on health staff in terms of needing to conduct specialized exams or procedures to detect possible effects on babies. Reproductive health services need to be strengthened, given that future Zika outbreaks in this region are possible. In a future epidemic, health personnel should be trained on how to properly disseminate information to patients and evaluate the impact on bio-physical-social results.

