











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
Permalink
I. INTRODUCTION
Dental implants are currently considered the gold standard in the oral rehabilitation of patients due to the high survival rate and patient satisfaction in relation to esthetics, performance, and comfort [1] . Normally the rehabilitation is performed in two stages. Initially, there is a surgical phase in which the implants are inserted into the bone and a second one in which the dental prosthesis is fitted over the implants once they have osseointegrated, which takes between three and six months. The provisionalization stage is key for the survival of the implant, in this stage the aim is to adapt the gingival tissues for future rehabilitation, provide comfort to the patient and restore aesthetics while the definitive rehabilitation is carried out [2].
For some years now, it has been proposed to place implants with immediate provisionalization, which allows maintaining bone and gingival tissue levels in a similar way to that obtained with the conventional two-phase technique, which also allows shorter treatments, and with immediate aesthetic results. which is more comfortable for patients, especially in the aesthetic area of the upper jaw [3]. Provisionalization of implants placed immediately after tooth extraction has also been reported to be an appropriate procedure due to its predictability, high success rate, and cosmetic results [4], [5].
It has also been reported that the immediate provisionalization of the inserted implants can be of a functional type in which the crown has occlusal contacts with the antagonist's teeth or of a non-functional type in which the provisional crown is modified so that it does not have contact in occlusion. centric or in any of the lateral displacements, with similar results in terms of maintaining bone levels and in relation to aesthetics [6].
In the process of provisional restoration of an implant, two elements are necessary: the provisional abutment that will support the provisional crown and the provisional crown itself, which is generally made of polymethylmethacrylate (PMMA); most temporary abutments are made of titanium, PMMA with a titanium base, or polyether ether ketone [7].
With the development of protocols for immediate provisionalization on implants, provisional abutments made of different materials such as titanium, ceramic and polymers emerged, each with advantages and disadvantages, but with comparable results in terms of aesthetics and resistance [8], [9].Currently, most of the provisional abutments available are made of polyether ether ketone (PEEK), a semi-crystalline and thermoplastic polymer that has been recognized for having very good mechanical properties and thermal stability , used in biomedical applications since 1982 [10], and widely used in dentistry [11]. the polymer most commonly used to make temporaries is PMMA, which has good mechanical strength, low cost, easy polishing, and the possibility of processing it by different techniques such as microwave, heat, cold or light [12]
For a provisional fixed prosthesis to fulfill its function, it must remain in position and resist the functional forces generated during mastication without suffering de-cementation, this is even more important in the rehabilitation of implants where the support of the crown is not a tooth but a abutment, and this provisionalization will not only guide the healing of the tissues but also create the emergence profile for the future prosthesis.
In the provisionalization process in implant rehabilitation, the provisional crown should be attached to the temporary PEEK abutment by means of PMMA to obtain a structure that can be screwed to the implants; however, poor adhesion has been reported due to the low surface energy of PEEK [13]. In order to improve it, surface treatments using abrasives, acids [14], plasma treatment [15], and the application of resin adhesives [16] have been proposed.
The development of technology and material sciences led to the emergence of additive manufacturing technologies and the appearance of new materials, including photopolymer resins for biomedical applications, which are characterized by good mechanical properties and for being biocompatible [17], [18]. This research proposed to elaborate temporary abutments for implantological rehabilitation by additive manufacturing technique using a photopolymer resin as an alternative to conventional PEEK abutments.
II. MATERIALS AND METHODS
Eighteen temporary abutments for implant rehabilitation were designed and fabricated by 3D printing using photopolymer resin and their mechanical and adhesion properties to PMMA were compared with those of PEEK abutments.
OnShape® software (Cambridge, USA) was used to model the temporary abutments, the devices were printed using CLEAR FLGP04 light-curing resin (Formlabs, Massachusetts, USA) and a Formlabs 2+ 3D printer (Formlabs, Massachusetts, USA) using the stereolithography technique. The printing parameters were layer height: 0.1mm; printing temperature: 190 degrees Celsius; and printing table temperature: 70 degrees Celsius.
For the adhesion tests, 12 temporary crowns were fabricated in self-curing PMMA (Veracryl, Antioquia, Colombia). The crowns were bonded to the PEEK abutments and to the photopolymer resin abutments with self-curing PMMA, without performing any type of surface treatment to the abutments and without using resin adhesives.
A. Mechanical Characterizations
By means of stress-strain curves, the mechanical properties in compression and bending of the experimental and commercial temporary columns were determined and compared.
To contrast the results, it was proposed as a null hypothesis that the experimental temporary abutments fabricated by 3D printing with Clear FLGPCL04 polymer resin have mechanical properties in compression, bending, and adhesion to PMMA similar to the commercial abutments made of PEEK.
Statistical analysis was performed with STATA 14 software (version 14, Statacorp, USA). The data were analyzed for differences between the PEEK and light-curing resin groups using the Wilcoxon Mann-Whitney test, as these were two independent samples of small size.
Values less than (p <0.05) were considered statistically significant in all tests and reject the null hypothesis of equality between the medians of the groups.
The tests were carried out at the Materials Engineering Laboratory of the Pontificia Universidad Javeriana in Cali, Colombia, using an Instron 3366 (Instrom, Norwood, Massachusetts, USA), equipped with a 10kN load cell. Compression bending and adhesion tests were performed on 18 experimental and 18 commercial temporary abutments made of PEEK (MIS, Galilee, Israel) using the same parameters and the same equipment.
1) Compression Tests. The abutments were tightened with a titanium set screw to a standard MIS® brand implant analog abutment (MIS, Galilee, Israel) with a torque of 15 N; the location of the analog and the abutment was done following the axiality of the load application and then compression forces were applied through a plate at a test speed of 0.5 mm/min until breakage. This process was repeated six times with each type of abutment.
To develop this test, an adaptation of the ASTM D695 (ISO 604) standard was made; as the standard does not contemplate compression in hollow cylinders (Figure 1), an adaptation of this was made, reducing the test speed to 0.5 mm/min, and calculating the stresses generated in the column as a function of the cross-sectional area (A) that supports the applied force [19] according to the equation.
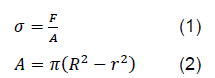
Where R is the outermost radius of the device and r is the innermost radius of the device.
2) Bending Test. The specimen was held at one end and a cantilever-type force was applied at the other end until the abutment failed; the test was performed at a rate of 1 mm/min. This process was repeated six times with the experimental abutments, and six times with the abutments of the control group.
To carry out this test, an adaptation of the ASTM D790 (ISO 178) standard was performed, which considers a three-point bending test. Therefore, according to the classical theory of solid mechanics, the stress generated in the specimens should be determined following the formula [19].

Where M, is the maximum moment generated in the specimen, c is the outermost point on the specimen from its center of inertia and I, is the inertia of the specimen.
3) Interfacial Adhesion Test. The abutments with their temporary crowns were held by the lower end of the analog in a vertical position; by means of the upper jaw of the equipment, which held the temporary tooth, a tensile force was applied until failure (detachment of the crown or fracture). This process was repeated six times with each type of abutment.
Regarding the interfacial adhesion test (Pull-out), so far there is no standard for the interfacial adhesion tests between two materials of the nature of the ones under study. However, there are several methods that have been tested and published [20] that can be adaptable to evaluate the interfacial adhesion between the abutment made with polymer and the resin that will bond the temporary tooth. In addition, the classical theory of solid mechanics [19] is followed, where the shear stress required to overcome the bonding of the materials is estimated as (4).

Where τ is the shear stress, F the applied force, and A is the bond area between the parts or materials.
To visualize the structure of the pillars after the adhesion tests, inspection was performed under a JEOL microscope Model JSM 6490 LV (Jeol co. 3-1-2 Musashino, Akishima, Tokyo 196-8558, JAPAN), these analyses were performed in the materials engineering laboratory at the Universidad del Valle, Cali, Colombia.
III. RESULTS AND DISCUSSION
During the masticatory function, the assembly of the provisional abutment and the provisional crown is subjected to stresses that can cause failure due to fracture or debonding, which makes it necessary to evaluate their performance through different mechanical tests as shown below.
A. Mechanical Characterizations
In this section, the results of the pillars made of PEEK and photopolymeric resin were compared, when they were subjected to compression, bending and interfacial adhesion tests.
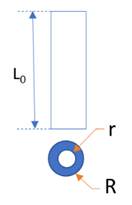
1) Compression Test. The figure 2 shows the results when comparing the medians of the two types of abutments in the compression test.
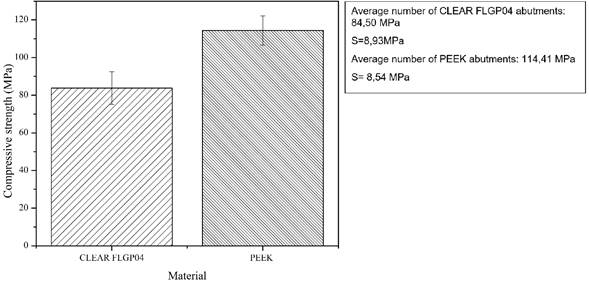
2) Bending Test. The following figure shows the results when comparing the averages of the two types of columns in the bending test.
In the review carried out, no studies were found where the mechanical properties of abutments printed in photopolymer resin were analyzed, because this material has been mainly used for the fabrication of temporary crowns by 3D printing, finding that, in general, they present good mechanical properties [21].
3) Interfacial Adhesion Test. The figure 4 shows the results when comparing the averages of the two types of abutments in the adhesion test.
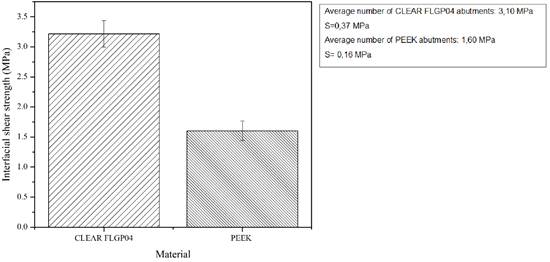
Figure 5 shows images of the abutments fabricated in PEEK during the adhesion tests; it can be seen how the temporary crown moves under the applied tensile force showing a failure in the union of the PEEK and the PMMA that acted as cementing material, evidencing an adhesive type of failure; remains of the cementing material can be seen by scanning electron microscopy.
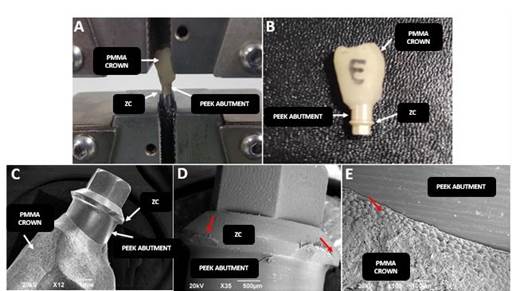
Fig. 5 Failures of PEEK abutments during adhesion tests. A: Abutment in Instron. B: Abutment with adhesion failure. C: 12X image. D: 35X image. E: 100X image. ZC: Area of the connection of the abutment to the analog. PEEK abutment: Observable area of the abutment. PMMA crown: Temporary crown. Red arrow: PMMA: PMMA fragment. SEM technique.
For some years different authors have drawn attention to the problems of bonding of devices made of PEEK with composite resin type materials due to the hydrophobic surface and its low surface energy, and the need to perform surface conditioning by different methods [22]. It has been recommended to perform surface treatments such as sulfuric acid 98% (sulfuric acid and hydrogen peroxide solutions), abrasives and resin adhesives [23], these treatments promote the formation of mechanical anchorages between the PEEK pillars and the PMMA used as adhesive.
Figure 6 shows the failure of an abutment made of photopolymer resin when subjected to adhesion tests, fracture of the abutment is observed in the connection area, by SEM it is possible to appreciate remains of the PMMA used as a cementitious material.
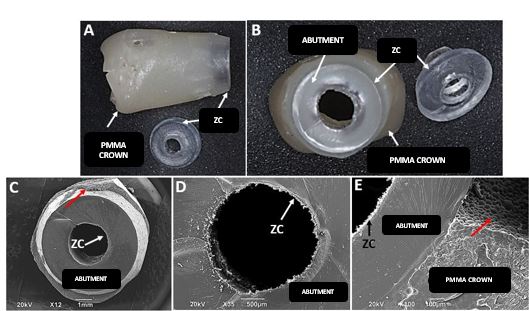
Fig. 6 Failures of the photopolymer resin abutments during adhesion testing. A: Longitudinal view. B: Cross-sectional view. C: SEM image at 12X. D: SEM image at 35X. E: SEM image at 100X. ZC: Connection zone. PMMA crown: Temporary crown. Red arrow: PMMA remains.
4) Statistical Analysis. The results obtained for each abutment in the different tests performed are presented in the Table 1.
Table 1 Mechanical properties of resin and PEEK abutments.
| Maximum resin value MPa | Maximum PEEK Value MPa | Statistical significance | ||
|---|---|---|---|---|
| Compression | 1 | 72.50629 | 111.00263 | 0.0039* |
| 2 | 78.80655 | 126.36095 | ||
| 3 | 88.82493 | 123.02025 | ||
| 4 | 78.03163 | 112.44906 | ||
| 5 | 99.38944 | 103.90524 | ||
| 6 | 85.01646 | 109.72842 | ||
| Flexion | 1 | 107.98246 | 111.36831 | 0.1093* |
| 2 | 137.09241 | 116.78464 | ||
| 3 | 77.95008 | 195.51279 | ||
| 4 | 161.84685 | 208.09194 | ||
| 5 | 120.05857 | 207.30653 | ||
| 6 | 118.52928 | 210.04601 | ||
| Adhesion | 1 | 3.29155 | 1.61819 | 0.039* |
| 2 | 3.38271 | 1.57223 | ||
| 3 | 2.57815 | 1.86006 | ||
| 4 | 3.52282 | 1.35194 | ||
| 5 | 2.79023 | 1.60581 | ||
| 6 | 3.0189 | 1.61886 |
* Statistical significance was calculated using the Mann Whitney U test.
In the Table 1, it can be observed that there is a significant difference in the medians between the resin and PEEK abutments group in the compression test, with the commercial abutments (PEEK) obtaining a better performance. As for the maximum stress in bending no significant differences were found, while in the adhesion tests the resin abutments had a better performance, the difference being statistically significant.
In the review carried out for this work, no articles that compared the mechanical properties of PEEK abutments with other polymeric abutments were found; there is only a few papers that tried to compare them with temporary titanium abutments, finding that PEEK abutments perform less well than metal abutments 18, 19 [18-19].
The few studies that were found on PEEK abutments were oriented to compare their mechanical properties with titanium abutments. Several articles were also found that mention the importance of improving adhesion with resins because this lack of adhesion has limited their use in dentistry, a topic that is still under discussion [19]. Among the techniques used to improve the adhesion of PEEK devices are sandblasting, plasma treatment, acid etching (98% sulfuric acid), laser treatment, and surface modifications with SiO2 or TiO2 20 [20].
In this research, the PEEK abutments were not subjected to any type of treatment because, being hollow cylinders with very little wall thickness, it was considered that any modification could affect their mechanical properties, which would affects the results.
IV. CONCLUSIONS
The abutments fabricated by 3D printing using photopolymer resin presented mechanical properties that make them suitable for use in the provisional rehabilitation of dental implants with a much greater capacity of bonding to PMMA acrylics than the abutments made of PEEK.
A significant difference in the medians between the resin and PEEK abutments group in the compression test was observed, 84,50 MPa for CLEAR FLGP04 and 114,41 MPa for the commercial abutments (PEEK) obtaining superior results.
As for the maximum stress in bending no significant differences were found in the medians between 123,09 MPa for CLEAR FLGP04 and 187,55 MPa for PEEK abutments.
While in the adhesion tests the resin CLEAR FLGP04 abutments had a better performance, a 3,10 MPa median with the difference being statistically significant to 1,60 MPa median for PEEK abutments group.

