










Services on Demand
Journal
Article
 text in
text in  Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Facultad de Odontología Universidad de Antioquia
Print version ISSN 0121-246X
Rev Fac Odontol Univ Antioq vol.23 no.1 Medellín July/Dec. 2011
ORIGINAL ARTICLES DERIVED FROM RESEARCH
Comparative in vitro study of root canal transportation , using three Nickel-Titaniu m rotar y systems: HERO Shaper, ProTaper Universal, and RaCe
Marcela Alcota Rojas1, Gabriela Compán Catenacci1, Juan Carlos Salinas Castro2, Ana MarÍa Palma Eyzaguirre1
1 Endodontics Area, Department of Conservative Dentistry, Facultad de
Odontología, Universidad de Chile
2 Department of Prosthesis, Facultad de Odontología, Universidad de Chile
SUBMITTED: MARCH 29, 2011-ACCEPTED: AUGUST 16, 2011
CORRESPONDING AUTHORMarcela Alcota Rojas
Sergio Livingston 943 Independencia,
Santiago, Chile
Telephone: 56-02-9781839
E-mail: malcota@u.uchile.cl
Alcota M, Compán G, Salinas JC, Palma AM. Comparative in vitro study of root canal transportation, using three nickeltitanium rotary systems: HERO Shaper, ProTaper Universal, and RaCe. Rev Fac Odontol Univ Antioq 2011; 23(1): 9-21.
ABSTRACT
INTRODUCTION:the objective of this in vitro study was to compare the degree of transportation of root canals using three rotary
systems: HERO Shaper, ProTaper Universal, and Race.
METHODS:a sample of thirty buccal root canals of upper molars with curvatures
between 25 and 35° was divided into three random groups of ten canals each, which were then instrumented by using the rotary systems
HERO Shaper, ProTaper Universal, and Race respectively, all to a diameter # 30 to the working length, using the motor NSK Endo-Mate TC
to control torque and speed. Radiographs were taken before and after mechanical instrumentation, and they were scanned with DuoScan
Agfa T1200 scanner at a resolution of 2400 dpi gray scale. Afterwards, by the method of lineal morphometry and using the computer system
for digital images NIH imageJ, a total of 12 measurements per root canal were done: 4 for the total root width, 4 for the concave wall and 4
for the convex wall, all at 1, 2, 4 and 6 mm respectively from the radiographic apex of the canal. The data were analyzed by using the Mann
Whitney Rank Sum and Kruskal Wallis nonparametric statistical analysis for independent samples.
RESULTS:Transportation was observed from
the root canal to the concave wall when the ProTaper Universal system was used, being statistically significant (p = 0,01).
CONCLUSION:the
ProTaper Universal rotary system produced the greatest number of transportations when compared with HERO Shaper and RaCe systems.
Key words: canal preparation, transportation, rotary systems.
INTRODUCTION
Since the emergence of the nickel-titanium alloy, a great variety of both manual and rotary instruments have been developed, trying to make the most of the advantages of this alloy.
Transportation is understood as a shift in the root canal location compared to its original position, resulting in a non-proportional wear of some dentin walls in relation to the canal’s original anatomy. This establishes one of the main concerns of the rotary instrumentation systems: avoiding canal transportation when using them, while achieving adequate and efficient enlargement all along the canal.1 Therefore, several authors suggest that using NiTi (nickel-titanium) rotary systems enable instrumentation of fine and curved canals, because they allow preparation of the canal with small or no transportation along the root canal axial shaft.2-4
Also, comparisons between the shaping ability of stainless steel hand files and the instrumentation used by the NiTi rotary systems have shown that, due to their rigidity, stainless steel files cause deformation of the natural shape of curved canals, enlargement of the apical foramen, apical transportation, and zip and elbow formation in the mid-third of the canal, which do not happen when using NiTi files, because of their flexibility.5 However, numerous reports show a great variety of results—many of them contradictory—on the degrees of root canal transportation and deformation caused by different rotary instrumentation systems.6-8
Thence the interest in an experimental comparison of HERO Shaper, ProTaper Universal and RaCe rotary systems, in order to determine which of them produces the minimum root canal transportation and deformation.
MATERIALS AND METHODS
This was an experimental, in vitro, blind study.
Operational description: A comparison will be made on the amount of dentin wear occurring at the upper molars’ mesial and distal (that is, concave and convex) walls when making rotary preparation of vestibular root canals with curvatures between 25 and 35°.
This comparison is based on the theoretical assumption that any instrumentation technique results in some canal wall dentin wear, with a possible change in the canal spatial location compared with its original position.
Variables
a) Independent variable: Technique
b) Dependent variable: Dentin wear
I. Tooth selection
The sample was made up by 30 root canals from first and second upper molars extracted from humans, according to the principle of morphological inspection, following these criteria:
- Vestibular root canals of 1st and 2nd upper molars.
- Fine root canals.
- Radicular curvatures between 25 and 35°, according to the S. W. Schneider curvature coefficient,9 in order to standardize the sample in accordance with this variable.
- Root canals with complete radicular formation.
The criteria for exclusion were as follows:
- Molars with their roots fused
- Molars with apical closure and incomplete radicular formation.
- Molars with root caries.
- Molars with root fracture.
- Molars with calcified and atresic root canals.
- Molars with previous endodontic treatment.
II. Sample preparation
1. Sample disinfection and storage:
The extracted molars were kept in a Formaline 10% Buffered solution until the process of disinfection and storage, when the following steps were taken.
- They were boiled in a recipient covered with a lid for 30 minutes in enough quantity (a liter) of running water (50%) and sodium hypochlorite (50%).
- Once boiled, they were drained and washed with a brush and soap, so as to wash out the remaining tissue adhered to them.
- They were rinsed with plenty of water and let to drain on absorbent paper.
- The molars were immersed in a hydrating solution (50% 10-volume hydrogen peroxide and 50% glycerine) until the time of their utilization.
2. Sample preparation before radiographic assessment:
- An access cavity was made on the molars using high- and low- speed burs with plenty of water irrigation. The vestibular root canals were selected from the upper molars.
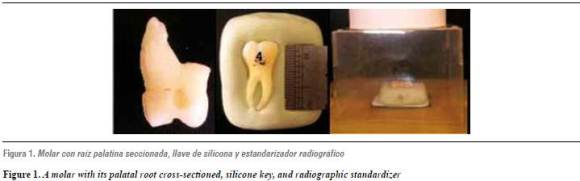
- The molars’ palatal roots were cross-sectioned, to facilitate radiographic assessment and to prevent overprojection on vestibular root canals (figure 1).
- A key of heavy silicone was made by pressing the molar against it, thus forming a mould that allowed pre- and post- surgical radiographic shots in the same angle and orientation of the molar curvature. Also, a 10-millimeter metal ruler was placed on each radiograph, as a way of scaling the sample and calibrating the measurements (figure 1).
- In order to identify the X-ray films corresponding to each molar, a lead metal sheet was placed on each top right corner along with the corresponding sample number.
- A bottom layer was made on yellow wax, in order to keep the film fixed on its position. The silicone keys were placed on this layer.
- In order to standardize the radiographic technique, an original method was crafted: a positioning device was designed as a support to the X-ray cone, so that it permanently stood in its position and at the same distance to the object to be radiographed (figure 1). The X-ray was taken under an exposure time of 0.25 sec and 60 kV. Previous tests were performed in order to verify that the radiographic shot was always taken under the same conditions of position and distance.
.
4. Root canal selection:
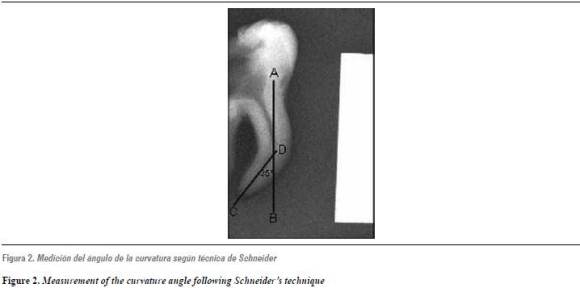
- Once the preliminary X-ray shots had been taken, the curvature angle was measured following Schneider’s technique9 (figure 2) including only the canals with angles between 25 and 35°.
III. Instrumentation procedure
Three experimental groups were formed, each having ten canals:
Group I: canals instrumented with the HERO Shaper system (Micromega, Besançon, France), according to the manufacturer’s directions up to file # 30, 0.04 taper.
Group II: canals instrumented with the ProTaper Universal system (Dentsply Maillefer, Ballaigues, Switzerland) according to the manufacturer’s directions up to file F3, which matches a file # 30 tip diameter and a progressive tapering of 0,09 to 0,05 of the active section.
Group III: canals instrumented with the RaCe system (FKG-Dentaire, Switzerland) up to file # 30, 0.04 tapering.
The working length for each canal was established by using a K-file #10 (Maillefer), which was introduced until reaching down the apical foramen. This distance was then measured subtracting 1 mm. All through the instrumentation, the canals were irrigated with 1 cm3 of 5.25% sodium hypochlorite before and after each instrument, and the irrigating needle was introduced as apically as possible before it was adhered to the canal, that is, being loose and supported by just one of the walls. The Endo-Mate TC NSK motor was used, with speeds of 250 to 350 rpm and torque 2.
All of the canals were instrumented by the same operator. In the three experimental groups, a set of files was used for every 5 instrumented canals.
Once they had been instrumented, the canals were X-rayed under the same preliminary conditions.
IV. Root canal preparation analysis
The pre- and post- instrumentation radiographs were digitalized with an Agfa Duoscan T 1200 scanner, with a resolution of 2400 dpi, in gray scale.
The images were modified by using Photo Shop v. 7.0 keeping the orientation of the selected canals in the same direction, so that all the measurements could be performed under identical conditions.
Random numbering from 1 to 60 was assigned in order to avoid biases and to carry out the blind study. Afterwards, the canals were analyzed and measured following the method of linear morphometry, using the NIH imageJ software.
An inter-observer calibration test was conducted for repeated measurements, in order to determine measurement reliability. It consisted of assessing a root randomly chosen, which was measured with the same methods and software two times a day for five days. Once the values had been obtained, a statistical t-test for dependent samples was applied.
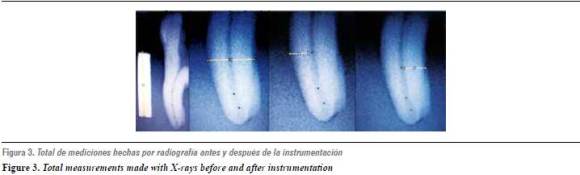
In order to standardize the measurement, it was scaled by means of the metal ruler used in the radiographs, which was of 10 mm. The measurements were made by placing parallel guides of 1, 2, 4 and 6 mm (figure 3) from the root canal radiographic vertex—which often coincided with the root radiographic vertex—. The images were analyzed under conditions of brightness and contrast adjustment in a random manner, in order to clearly determine dentin boundaries before and after instrumentation of the root canals. Per each radiograph, 12 measurements were made in total in order to determine the total length of the root width, the concave dentin wall and the convex dentin wall at 1, 2, 4 and 6 mm (figure 3). The obtained quantities were expressed in millimeters. Transportation of the root canal was supposed when a non-homogenous wear difference of 0,4 mm or greater occurred between the dentin walls in any of the measured spots.
For the statistical analysis, the t-test for dependent samples was used in order to establish the inter-observer record accuracy. The non-parametric Mann-Whitney Rank Sum test for independent samples was used to determine the difference between concave wall and convex wall wear for each of the 10 samples of each instrumentation system in all the spots measured (at 1, 2, 4 and 6 mm from the root canal vertex).
The Kruskal Wallis non-parametric variance test, with a 95% confidence interval and a p of ≤ 0.05, was used to establish differences in transportation percentages between the systems. Therefore, the transportation percentage of each system was determined, establishing the presence or absence of transportation in the 10 canals analyzed per system.
RESULTS
The results of the t-test for dependent samples, conducted with the intention of establishing reliability of the inter-observer record, revealed no significant differences in the inter-rater reliability analysis.
The results displayed on table 1 show the presence or absence of transportation for both the concave wall and the convex wall at the various levels of observation (1, 2, 4, 6 mm) in the 10 samples instrumented with the HERO Shaper rotary instrumentation system.
Absence of canal transportation is observed, in spite of the presence of greater wear at 1 and 6 mm. This difference is not statistically significant.
Table 2 shows differences between concave wall wear and convex wall wear when using the ProTaper Universal system at the different levels of measurement.



Canal transportation is observed towards the concave wall of the canal at 6 mm. This is statistically significant (p = 0.01).
Table 3 shows the presence or absence of transportation of the concave wall and the convex wall for the RaCe rotary instrumentation system, demonstrating the absence of transportation at the different levels of measurement.
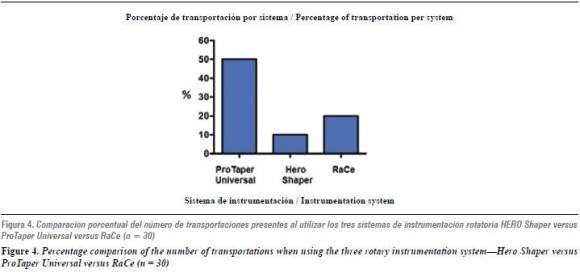
Figure 4 compares the transportation percentages of the three rotary instrumentation systems.
These results show that the system producing the highest percentage of transportation is the ProTaper Universal system (50%), since 5 of the 10 canals prepared with this rotary system exhibited transportation at any of the spots measured, this difference being significant when compared to the percentage of transportation occurred with the other systems (p = 0.05).
Finally, it is important to point out that during the procedures two S1 instruments of the ProTaper Universal system were fractured, and they had to be replaced, thus obtaining a final sample of 30 instrumented canals.
DISCUSSION
The objective of this study was to compare the level of transportation in canals with curvatures between 25 and 35°, when instrumented by the same operator using three rotary instrumentation techniques: HERO Shaper, ProTaper Universal, and RaCe.
In the course of this study, significant differences were observed in terms of the levels of wear of the root canal’s dentin walls, when using the ProTaper Universal system, finding the greatest wear in the concave dentin wall at 6 mm (mid third). This can be explained because of the greater rigidity of the instruments and for the progressive tapering presented in the same instrument, making it difficult to perform a selective handling of instruments according to the anatomic features of the root canal. These results agree with the findings reported by Yang et al, who demonstrated that the ProTaper Universal system removes a higher amount of dentin in the coronal and middle thirds of the canal.6 Other studies suggest that transportation produced by the ProTaper Universal instruments might be due to the progressive tapering along their cross-section surface, since it has been demonstrated that the transportations found were produced by instrument F3, and therefore it should be moderately used when preparing curved canals.10,11 This is why different studies recommend using a combination of rotary systems to prepare curved canals, since it has been demonstrated that the ProTaper Universal system alone produces transportation in the middle third of the root canal.7 Also, reducing instrument tapering is suggested, since an instrument #30 with 2% taper is more flexible than an instrument #30 with 6% taper, being lower taper safer when preparing the apical and middle thirds.12-13
Contrary to the results obtained in this study, Guelzow et al compared root canal preparation using six different Ni-Ti rotary systems (FlexMaster, System GT, HERO 642, K3, ProTaper, and RaCe) and demonstrated that all of them preserve the curvature of the root canal, without any significant difference among them. They also established that ProTaper is able to keep root canals with more regular diameters in their coronal, middle and apical thirds.8
Other studies also report the presence of fractures in S1 files of the instrumentation system during the procedure, which in most cases are produced by torsional defects, exhibiting circular abrasion marks at 4.3 ± 1.9 mm Do when stereo-microscopically evaluated.14-17 On these grounds, the reason why the apical third is not affected may be inferred: because the instruments are not usually in contact with the apical zone, different from the cervical and middle canal thirds, which in most cases coincide with the beginning or body of the curvature.
Several studies comparing the ProTaper Universal and HERO Shaper rotary instrumentation systems have demonstrated that the latter produces a smaller amount of transportation and a better centering capability in the apical section, which may be due to reduced tapering and lower instrument rigidity if compared with the ProTaper Universal system.7 Such finding is similar to the one in this study, in which the absence of canal transportation was observed when using the HERO Shaper mechanized instrumentation system. In contrast, Javaheri et al18 showed the presence of transportation towards the convex wall of the curvature in the middle and apical thirds, and towards the concave wall in the coronal third when using the HERO Shaper mechanized instrumentation system. However, these results were not statistically significant.
Concerning the RaCe mechanized instrumentation system, our findings suggest a low significant percentage of transportation during observations at 1, 2, 4 and 6 mm from the canal apex. This agrees with the reports by Schafer et al, who demonstrated that canals prepared with RaCe instruments are more capable of maintaining their centricity and their original canal curvature compared with those prepared with ProTaper files, especially in canals with curvatures of 35°.19 Other authors have also reported that root canals instrumented with RaCe display higher centering, compared with those instrumented with the ProTaper Universal rotary instrumentation system.20-23 In contradiction with this study, Guelzow et al demonstrated that all the systems analyzed in their research (FlexMater, System Gt, Hero 642, K3, ProTaper and RaCe) conserve the root canal curvature, without any significant differences among them. Similarly, Paque et al reported that when comparing root canal preparation by using RaCe and ProTaper Ni-Ti rotary instruments, both systems leave the canal’s original curvature intact.7
In the light of our results, we can state that the rotary systems that allow optimal shaping of fine canals with curvatures between 25 and 35°, leaving the anatomy of the curvature intact, are the HERO Shaper and RaCe mechanized instrumentation systems, differently from the ProTaper Universal instrumentation system, which statistically presents the highest number of transported canals with a significant difference.
1. Herrera de Luna AF, Durán J, án A. Evaluación de la transportación y ensanchamiento in vitro del sistema ProTaper. Rev ADM 2004; 61(1): 5-13. [ Links ]
2. Thompson SA, Dummer PM. Shaping ability of ProFile 04 taper series 29 rotary nickel-titanium instruments in simulated root canals: Part 1. Int Endod J 1997; 30(1): 1-7. [ Links ]
3. Thompson SA, Dummer PM. Shaping ability of ProFile 04 taper series 29 rotary nickel-titanium instruments in simulated root canals: Part 2. Int Endod J 1997; 30(2): 8-15. [ Links ]
4. Buchanan LS. The standardized taper root canal preparation- Part 2. File selection and safe handpiece-driven file use. Int Endod J 2001; 34: 63-71. instrumentation for root canal preparation. Int Endod J 2005; 38(10): 743-752. [ Links ]
5. K um KY, Spängberg L, Cha BY, Il-Young J, Seung-Jong L, Chan-Young L. Shaping ability of three profile rotary instrumentation techniques in simulated resin root canal. J Endod 2000; 26(12): 719-723. [ Links ]
6. Y ang GB, Zhou XD, Zheng YL, Zhang H, Shu Y, Wu HK. Shaping ability of progressive versus constant taper instruments in curved root canals of extracted teeth. Int Endod J 2007; 40(9): 707-714. [ Links ]
7. Paque F, Musch U, Hulsmann M. Comparison of root canal preparation using RaCe and ProTaper rotary NiTi instruments. Int Endod J 2005; 38 (1): 8-16. [ Links ]
8. Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium system and hand instrumentation for root canal preparation. Int Endod J 2005; 38(10): 743-752. [ Links ]
9. Schneider S. A comparison of canal preparations in straight and curved root canals. Oral Surg 1971; 32(2): 271-275. [ Links ]
10. Y ang GB, Zhou XD, Zhang H, Wu HK. Shaping ability of progressive versus constant taper instruments in simulated root canals. Int Endod J 2006; 39(10): 791-799. [ Links ]
11. Ounsi HF, Salameh Z, Al-Shalan T, Ferrari M, Grandini S, Pashley DH et al. Effect of clinical use on the cyclic fatigue resistance of ProTaper nickel-titanium rotary instruments. J Endod 2007; 33(6): 737-741. [ Links ]
12. L eonardo MR, Leonardo RT. Sistemas rotatorios en endodoncia: instrumentos de níquel-titanio. São Paulo: Artes Médicas, 2002. [ Links ]
13. West J. Progressive taper technology: rationale and clinical technique for the new ProTaper Universal System. Dent Today 2006; 25(12): 64, 66-69. [ Links ]
14. Cheung GS, Peng B, Bian Z, Shen Y, Darvell BW. Defects in ProTaper S1 instruments after clinical use: fractographic examination. Int Endod J 2005; 38(11): 802-809. [ Links ]
15. Wei X, Ling J, Jiang J, Huang X, Liu L. Modes of failure of ProTaper nickel-titanium rotary instruments ofter clinical use. J Endod 2007; 33(3): 276-279. [ Links ]
16. Peng B, Shen Y, Cheung GS, Xia TJ. Defects in ProTaper S1 instruments after clinical use: longitudinal examination. Int< Endod J 2005; 38(8): 550-557. [ Links ]
17. Guilford WL, Lemons JE, Eleazer PD. A comparison of torque to fracture rotary files with tips bound in simulated curved canal. J Endod 2005; 31(6): 468-470. [ Links ]
18. Javaheri HH, Javeheri GH. A comparison of three Ni-Ti rotary instruments in apical transportation. J Endod 2007; 33(3): 284-286. [ Links ]
19. Schafer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper v/s RaCe. Part 1. Shaping ability in simulated curved canals. Int Endod J 2004; 37(4): 229-238. [ Links ]
20. Ozurg Uyanik M, Cehreli ZC, Ozgen Mocan B, Tasman Dagli F. Comparative evaluation of three nickel-titanium instrumentation systems in human teeth using computed tomography. J Endod 2006; 32(7): 668-671. [ Links ]
21. Schafer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part 2. Cleaning effectiveness and shaping ability in severely curved root canals of extracted teeth. Int Endod J 2004; 37(4): 239-248. [ Links ]
22. Al-Sudani D, Al-Sudani S. A comparison of the canal centering ability of ProFile, K3, and RaCe Nickel-Titanium rotary systems. J Endod 2006; 32(12): 1198-1201. [ Links ]
23. Rangel S, Cremonese R, Bryant S, Dummer P. Shaping ability of RaCe rotary nikel-titanium instruments in simulated root canals. J Endod 2005; 31: 460-463. [ Links ]

